
Remember me

The section summarizes case-control studies that investigated the association between pesticide exposure and PD risk. An overview of the these studies and their results is presented in Table 1. The studies are grouped as follows: First, case-control-studies with multiple publications derived from the same study population. Next, larger case control-studies including more than 200 PD cases, presented in descending order of case group size. Last, smaller case-control studies with fewer than 200 PD cases, also presented by case group size. The quality of evidence was assessed using the GRADE criteria, with ratings ranging from very low and moderate. The main limitation preventing higher ratings was inherently low baseline level from the case-control designs. Reasons for downgrading included risk of bias in single center studies and imprecisions caused by wide confidence intervals. Reasons for upgrading included large effect sizes (odds ratios [OR] > 2) or very large effect sizes (OR > 5), as well as trends toward dose-response relationships. A detailed summary of the GRADE assessment is provided in the Supplementary material.
Table 1 Case-control studies that investigated the association between pesticide exposure and PD riskFrench case-control-studies, including members of the agricultural social mutualitySeveral French case-control studies have investigated pesticide exposure and PD risk, recruiting members of the Agricultural Social Mutuality (in French: Mutualité Sociale Agricole; MSA), where healthcare for PD is provided free of charge. In one study, MSA members who applied for free PD-related healthcare between February 1998 and August 1999 were recruited as cases and matched–MSA members who requested reimbursement for other health conditions. Pesticide exposure was assessed via questionnaires and home interviews conducted by occupational physicians (Galanaud et al. 2005; Elbaz et al. 2009). In this analyis, 247 PD cases were matched–676 controls. Professional pesticide use was associated with an increased PD risk (OR 1.8; 95% CI 1.1–3.1) compared with never users (Galanaud et al. 2005).
A follow-ups analysis of the same study population included 224 PD cases and 577 controls, focusing on exposure–different functional groups of pesticides. Interestingly, professional exposure–insecticides increased PD risk in men, while professional exposure–fungicides increased PD risk in women. In men over 65 years, higher cumulative exposure, defined as exposure above the median,–insecticides and fungicides was associated with increased PD risk (insecticides: OR 5.4; 95% CI 1.5–20.0; fungicides: OR 4.8; 95% CI 1.2–19.3). No significant increase was observed in men under 65, and the sample size was too small for age-stratification in women. Herbicide exposure was not significantly associated with increased PD risk in either sex. Analysis by chemical family revealed significant associations in men for organochlorides (OR 2.4; 95% CI 1.2–5.0), amides (OR 3.1; 95% CI 1.2–8.3), and dithiocarbamates (OR 2.1; 95% CI 1.0–4.3). Among men over 65, ssociations were even stronger for organochlorides (OR 4.2; 95% CI 1.5–11.9), nitriles (OR 11.4; 95% CI 1.4–93.7), and phenoxy pesticides (OR 2.9; 95% CI 1.1–7.3) (Elbaz et al. 2009).
In another French case-control study, involving only male MSA members, 133 farmers, who purchased antiparkinsonian drugs in the years 2006 and 2007, were matched–298 farmers without PD. The analysis was stratified by tremor-dominant and non-tremor-dominant PD. Although overall pesticide exposure time did not differ significantly between cases and controls, cumulative exposure (i.e. total number of applications) and average annual applications were significantly associated with PD risk. Subanalyses showed that fungicide use and higher average exposure intensity–insecticides were linked–increased PD risk, however only for tremor-dominant PD. By contrast, herbicide exposure was not significantly associated with PD risk (Moisan et al. 2015).
The farming and movement evaluation (FAME) studyThe FAME study, a case-control-study that was nested within the Agricultural Health Study (AHS), investigated pesticide exposure among 110 PD cases and 358 healthy controls who reported pesticide use (Tanner et al. 2011). The study found significant associations between PD and use of paraquat (OR 2.5; 95% CI 1.4–4.7) and rotenone (OR 2.5; 95% CI 1.3–4.7). A follow-up study in the same study population examined protective glove use among individuals involved in pesticide mixing or application. After adjustment for smoking, sex, age, and hygiene measures, including glove use, paraquat (OR 2.6; 95% CI 1.1–6.1) and rotenone (OR 5.5; 95% CI 2.0–15.3) use remained significantly associated with PD risk compared–never use (Furlong et al. 2015). The level of evidence for both publications was moderate, justified by the large effect sizes.
The Parkinson environment gene (PEG) studyThe PEG study, conducted in rural communities in California, generated nine publications identified in the literature search. Initially, 162 PD cases diagnosed between 1998 and 2003 were investigated and matched–controls (Kang et al. 2005). The study was later expanded–include PD cases diagnosed between 1998 and 2007, yielding 1167 PD cases, with case groups of ~ 360 in earlier publications and ~ 750 in later ones (Table 2).
Table 2 Cohort studies and registries that investigated investigated the association between pesticide exposure and PD risk.In one analyisis of 368 PD cases and 341 controls combined exposure–paraquat and maneb between 1974 and 1999 was associated with increased PD risk (OR 2.14; 95% CI 1.24–3.68). However, exposure restricted to 1990–1999 was not significantly associated (OR 0.93; 95% CI 0.45–1.94). Notably, exposure between 1974 and 1989 was significantly associated with PD risk in both younger (< 60 years; OR 4.17; 95% CI 1.15–15.16) and older (> 60 years; OR 2.15; 95% CI 1.15–4.02) individuals. Over the longer time window (1974–1999), increased risk remained significant only in younger individuals (< 60 years; OR 5.07; 95% CI 1.75 and 14.71), with only a trend observed in older participants (> 60 years; OR 1.36; 95% CI 0.83–2.23). The authors concluded that paraquat and maneb may act synergistically, particularly when exposure occurs early in life (Costello et al. 2009).
Another analysis examined well water concentrations of pesticides in different counties in the study area and found that diazinon, an organophosphate, was linked–a slightly elevated PD risk (OR 1.58; 95% CI 1.03–2.43) (Gatto et al. 2009), though the evidence was rated very low due–the indirect exposure measurement. In another study of 362 PD cases and 341 controls, ziram exposure at both residence and workplace was associated with a significantly increased PD risk (OR 3.01; 95% CI 1.69–5.38), whereas exposure at residence or workplace alone was not. A similar pattern was observed for paraquat (combined exposure: OR 1.5; 95% CI 1.03–2.18). By contrast, maneb exposure at residence (OR 1.71; 95% CI 1.06–2.77), workplace (OR 1.77; 95% CI 1.02–3.09), or both (OR 2.26; 95% CI 1.22–4.20) was consistently associated with increased PD risk (Wang et al. 2011).
Further analysis confirmed these associations. Paraquat exposure was linked–PD risk (OR 1.43; 95% CI 1.43; 95% CI 1.11–1.84) independent of traumatic brain injury, in an analysis that addressed the association between traumatic brain injury and paraquat exposure (Lee et al. 2012). In an analysis of 357 PD cases and 807 controls, household use of organophosphate pesticides was linked to PD (OR 1.71; 95% CI 1.21–2.41), with chlorpyrifos specifically showing a significant association (OR 2.73; 95% CI 1.03–7.24) (Narayan et al. 2013). In another analysis of 357 PD cases and 750 controls, a job exposure matrix–estimate pesticide exposure was used and exposure stratified this in low, medium, and high. Medium (OR 1.61; 95% CI 1.00–2.62) and high exposure (OR 1.97; 95% CI 1.11–3.48), but not low exposure (OR 1.17; 95% CI 0.61–2.24) was linked–increased PD risk (Liew et al. 2014).
In another analysis of 357 PD cases and 752 healthy controls, the authors investigated residence and workplace exposure–different organophosphates and found that workplace only (OR 4.74: 95% CI 2.27–9.92) and both workplace and residential exposure (OR 5.93; 95% CI 1.69–20.87)–demeton was associated with the highest PD risk, whereas residential only exposure to merphos (OR 3.13; 95% CI 1.67–5.79) was associated with the highest PD risk (Wang et al. 2014). Another analysis comapring occupational pesticide use with no occupational use in 360 PD cases and 827 controls found an overall increased PD risk pesticide (OR 2.5; 95% CI 1.5–4.5). Stratification by functional class revealed significant associations for herbicides (OR 2.45; 95% CI 1.37–4.36), insecticides (OR 2.1; 95% CI 1.22–3.60), and fungicides (OR 3.11; 95% CI 1.65–5.88) (Narayan et al. 2017). Among chemical families carbamates were significantly associated with PD (OR 5.55; 95% CI 1.81–17.04), whereas organochlorine and organophosphates showed non-significant trends (Narayan et al. 2017). The levels of evidence from the PEG study ranged from very low–moderate, with large effect sizes and dose-response trends supporting upgrading.
Case-control study from the NetherlandsA Dutch case-control study recruited 444 PD cases and 876 controls between April 2010 and June 2012 across five hospitals in four regions of the country (van der Mark et al. 2014). Correlations between exposure–different pesticide classes (herbicides, fungicides, insecticides) were strong (r = 0.73–0.83), indicating concurrent exposure–multiple pesticides. While there were trends towards increased PD risk associated with high pesticide exposure and individual functional groups, no association was statistically significant and no clear dose-response effect could be observed. High exposure–benomyl was significantly associated with PD risk (OR 2.46; 95% CI 1.16–5.22), but low exposure showed a trend toward decreased risk (OR 06.9; 95% CI 0.29–1.66) (van der Mark et al. 2014). The general level of evidence for low, despite a trend toward dose-response effects. Nevertheless, this study highlights the challenge of disentangling individual pesticide exposures due to correlated usage patterns.
A follow-up analysis estimated exposure based on residential proximity–the place of pesticide use. The strongest association was observed for fenpropimorph (OR 2.79; 95% CI 1.33–5.89). Other pesticides, including paraquat, lindane, maneb, and benomyl, showed non-significant trends toward increased PD risk (Brouwer et al. 2017). Despite the strong association with fenpropimorph evidence quality remained low due–indirect exposure estimation.
Group health Cooperative, Washington State, USAThe Group Health Cooperative recruited 156 PD cases and 241 controls between 1992 and 2002 (Firestone et al. 2005), later expanding–404 PD cases and 526 controls (Firestone et al. 2010). In one analysis, the authors found no increased PD risk associated with overall occupational pesticide exposure (1.01; 95% CI 0.53–1.92). Herbicide exposure showed a trend towards higher PD risk (OR 1.41; 95% CI 0.51–3.88), whereas insecticide (OR 0.88; 95% CI 0.44–1.76) and fungicide (0.38; 95% CI 0.07–2.05) showed opposite trends. A similar pattern was observed for home-bases pesticide use with no association for overall pesticide use (OR 0.95; 95% CI 0.66–1.37), a trend towards increased risk with herbicides (1.41; 95% CI 0.51–3.88), and opposite trends with insecticides (OR 0.88; 95% CI 0.44–1.76) and fungicides (OR 0.55; 95% CI 0.29–1.05) (Firestone et al. 2005). In the extended study groups, the authors investigated differences in PD risk between men and women and found a trend towards reduced PD risk in men (OR 0.6; 95% CI 0.3–1.29), and a trend towards elevated PD risk in women (OR 3.9, 95% CI 0.39–39.4). However, the number of exposed women was too low–draw conclusions (Firestone et al. 2010). In summary, the Group Health Cooperative did not provide convincing evidence of an association between pesticide exposure and PD risk, resulting in a very low GRADE rating.
Geoparkinson studyThe Georparkinson study was conducted in five regions across Europe. In one publication the authors investigated 767 PD cases and matched them to 1989 controls. Using a job exposure matrix, they estimated exposure to several environmental factors, including pesticides, stratified into low and high exposure. While low exposure was associated with a trend towards higher PD risk (OR 1.09; 95% CI 0.77–1.55), high exposure significantly increased the risk for PD (1.39; 95% CI 1.02–1.89) (Dick et al. 2007). No factors were identified to downgrade or upgrade the level of evidence in this study, resulting in an overall low level of evidence.
Case-control study from ItalyA case control study conducted in six neurology departments in Italy enrolled 694 PD cases and 640 controls. The authors investigated multiple lifestyle factors, including pesticide exposure, which was associated with a significantly increased PD risk (OR 2.99; 95% CI 1.8–5.1) (Belvisi et al. 2020). Due to the large effects observed and absence of reasons for downgrading, the level of evidence of this study was rated as moderate.
Case-control study from PakistanA large case-control study conducted in Pakistan, matched 600 PD cases–1200 controls. The authors investigated the association between PD risk and the use of several pesticides. While pesticide use in general was associated with a strong increase in PD risk (OR 4.52; 95% CI 2.49–8.19), only the use of aldrin, an organochloride, was individually associated with a significantly increased PD risk (OR 11.0; 95% CI 4.02–30.07). However, the group exposed–aldrin was by far the largest (132 cases and 30 controls), whereas the number of users of other pesticides ranged from only 6–30, leading–very wide confidence intervals (Tufail 2019). Despite the strong effect—the second strongest among all studies - the quality of evidence was rated very low due–a very high risk of bias, as the study was conducted a single hospital. Although the effect of aldrin would qualify for upgrading, the general pesticides did not.
Case-control study from the united States and CanadaIn a case-control study performed in seven regions in the United States and one region in Canada, 519 PD cases were matched–511 controls. The authors assessed use of pesticides in general as well as the use of eight specific pesticides. General use of pesticide was associated with a significantly increased PD risk (OR 1.90; 95% CI 1.12–3.21). Furthermore, the use of 2,4-dichlorophenoxyacetic acid was associated with an elevated PD risk (OR 2.59; 95% CI 1.03–6.48), while no significant associations were found for other pesticides, most likely due–the low number of exposed individuals (0–9 per group) (Tanner et al. 2009). The overall level of evidence of this study was rated low.
Case-control study from GermanyIn a German case control study, PD patients were recruited from nice neurological clinics. A total of 380 patients were matched–controls. Among various environmental factors, pesticide exposure was quantified in “dose-years”, weighted by frequency of use (rarely = 1; for special indications = 2; seasonally = 3). The study found a trend toward increased PD risk associated with herbicide use (OR 2.2; 95% CI 0.9–5.2) and insecticide use (OR 1.6; 95% CI 0.7–3.4) compared–neighborhood controls, and a statistically significant risk associated with herbicide use compared–regional controls (OR 2.4; 95% CI 1.0–6.0). Specifically, exposure to organochlorides, alkylated phosphates and carbamates was associated with elevated PD risk (Seidler et al. 1996). Despite the large effect, the overall quality of evidence was rated low due–wide confidence intervals.
Case control study from North CarolinaIn a family-based case control study conducted in North Carolina between 2000 and 2006, 319 PD cases were matched to 296 controls, of whom 252 were relatives of the cases. Pesticide exposure was assessed by telephone questionnaires. The authors found a significantly increased PD risk associated with a history of direct pesticide application (OR 1.61; 95% CI 1.13–2.29). Higher risk was observed with more frequent exposure (> 10 days/year: OR 2.07; 95% CI 1.26–3.42), longer duration (> 26 years: OR 1.86; 95% CI 1.16–3.00) and greater cumulative exposure (> 215 days (OR 2.37; 95% CI 1.42–3.94). Interestingly, in a sub-analysis stratified by family history of PD, the association between pesticide exposure and PD risk was present only in individuals without a family history of PD, suggesting a stronger impact of pesticides in sporadic PD (Hancock et al. 2008). No factors were identified–downgrade or upgrade the evidence, resulting in a low level of evidence.
Case-control study from AustraliaIn a case-control-study conducted in the 1990 s in Australia, 224 PD cases were matched to 310 controls. The authors asked about pesticides/herbicides exposure (used as one variable) and found no significant association with PD risk (OR 1.2; 95% CI 0.8–1.5). They also assessed rural residency, which was associated with increased PD risk (OR 1.8; 95% CI 1.7–2.5), but the association did not remain significant in logistic regression (McCann et al. 1998). The overall level of evidence was rated as very low.
Case-control study from Hong KongA case-control-study conducted in the 1990 s in Hong Kong investigated several PD risk factors in 215 PD cases and 313 controls. There was a trend towards increased PD risk associated with pesticide exposure in farming (OR 1.80; 95% CI 0.903–3.58). I a sex-stratified analysis, women showed a significantly elevated risk (OR 6.84; 95% CI 1.90–24.7), whereas men showed a non-significant trend towards reduced risk (OR 0.68; 95% CI 0.25–1.83) (Chan et al. 1998). These contradictory results combined with wide confidence intervals led–downgrading of the evidence to very low level.
Smaller case-control-studies with fewer than 200 casesThe literature search revealed 11 smaller case-control studies with fewer than 200 PD cases investigating the association between pesticide exposure and PD risk. One study conducted in Eastern India reported the highest risk estimate (OR 17.4; 95% CI 4.97–58.84) (Sanyal et al. 2010), but evidence quality was very low. A study from Minnesota, USA, found an increased PD risk only in men (OR 2.4; 95% CI 1.1–5.4) and a non-significant trend towards reduced risk in women (0.6; 95% CI 0.2–1.9) (Frigerio et al. 2006). A study from New York, USA, reported a significantly increased PD risk (OR 2.84; 95% CI 1.34–6.00), though its reliance on self-administered paper surveys introduced high risk of bias (Shermon et al. 2022). A study from the Detroit area found elevated PD risk associated with herbicide (OR 4.1; 95% CI 1.37–12.24) and insecticide exposure (OR 3.55; 95% CI 1.75–7.18), but not with fungicides (OR 1.60; 95% CI 0.47–5.45) (Gorell et al. 1998). In Calgary, Canada, herbicide use was associated with increased PD risk (OR 2.36; 95% CI 1.10–5.04) (Semchuk and Love 1995). A study from Taiwan identified significantly increased PD risks linked to rural residence (OR 2.04; 95% CI 1.23–3.38), farming (OR 1.81; 95% CI 1.25–2.64) and use of herbicides/pesticides (OR 2.89; 95% CI 2.28–3.66). Paraquat use in particular was associated with elevated PD risk (OR 3.22; 95% CI 2.41–4.31) (Liou et al. 1997). A study from Belgrade reported increased PD risk with insecticide exposure (OR 3.22; 95% CI 1.32–7.87) (Vlajinac et al. 2010). In Brazil, direct management of pesticides at workplace (OR 3.78; 95% CI 1.92–7.45) and history of pesticide exposure at workplace (OR 2.35; 95% CI 1.36–4.06) was associated with increased PD risk (Silvestre et al. 2020). A study from southwestern France found significantly increased PD risk (OR 2.20; 95% CI 1.11–4.34) associated with pesticide exposure (Baldi et al. 2003a). A case-control study from east Texas examined multiple pesticides and reported strong associations with rotenone (OR 10.0; 95% CI 2.9–34.3) and chlorpyrifos (OR 2.0; 95% CI 1.02–3.8) use (Dhillon et al. 2008).
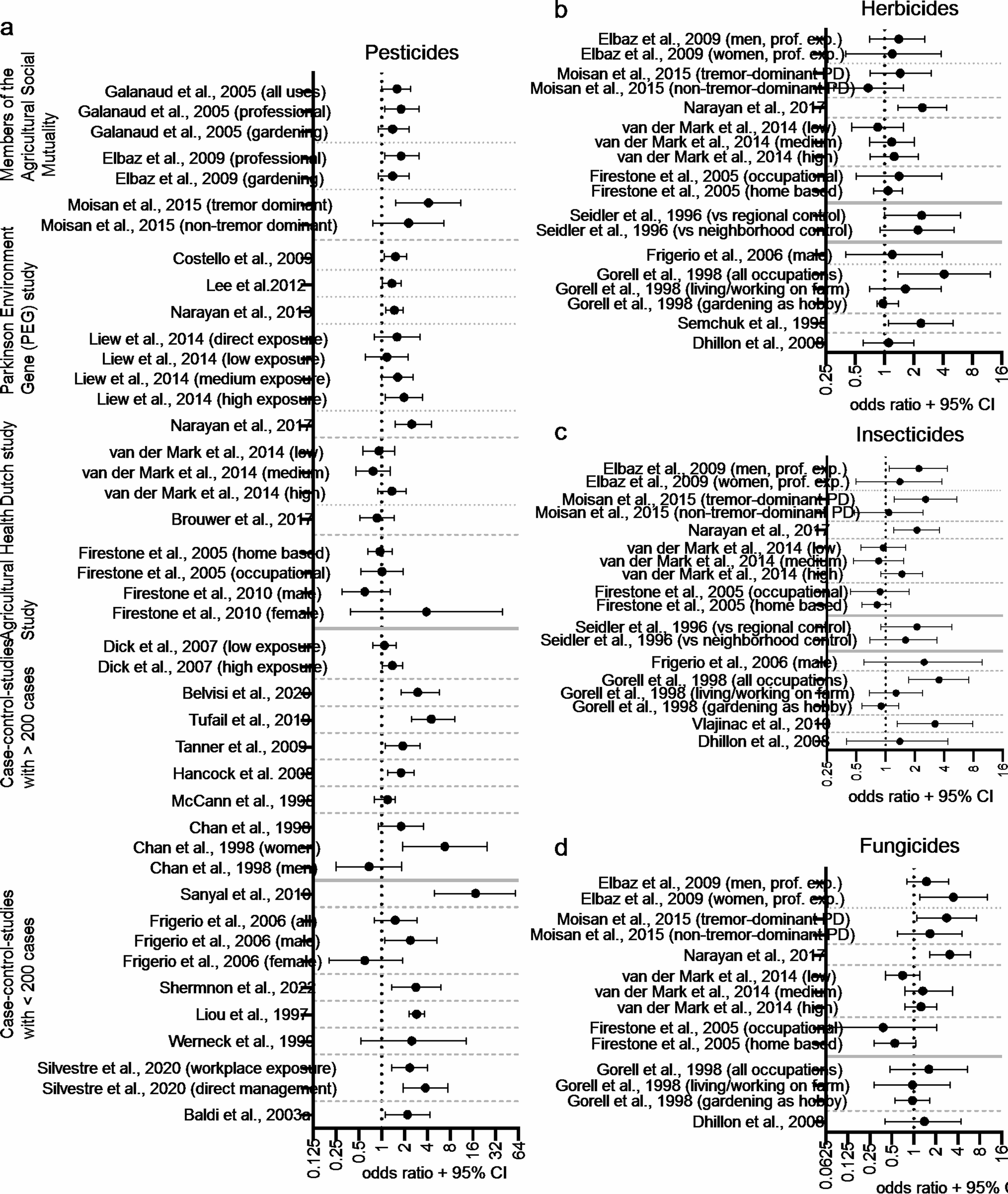
The available data on PD risk in association with pesticide exposure from case-control studies are illustrated in Fig. 1a with a distinction by functional groups illustrated in Fig. 1b–d. Figures 2 and 3 show the data from studies that reported an association between PD risk and individual pesticides.
Overall, most case-control studies demonstrated trends or significant associations between pesticide exposure and increased PD risk. However, the overall quality of evidence was low to moderate. Only a few studies (Dick et al. 2007; Liew et al. 2014; van der Mark et al. 2014) were designed to assess dose-response effects. Furthermore, only some studies distinguished between functional groups of pesticides (Fig. 1b–d), and even fewer analyzed individual pesticides (Figs. 2 and 3). Results were not always consistent: for example, some studies reported higher risks in women (Firestone et al. 2010; Chan et al. 1998), whereas others suggested the opposite (Frigerio et al. 2006). Subgroup analyses were often limited by small case numbers, reducing data quality and leading to wide confidence intervals.
Fig. 1
Forest plots showing results of case-control studies. The plots shows the odds ratios with the error bars indicating the 95% confidence intervals. a Results of case-control studies that reported an overall effect of pesticide exposure on PD risk. Dotted horizontal lines separate different publications with the same or overlapping study populations. Dashed horizontal lines separate studies within the same category (i.e. studies with more than one publication, larger studies with > 200 cases, smaller studies with fewer < 200 cases). Solid lines separate the different categories. b Results from studies that reported effects of herbicides. c: Results from studies that reported effects of insecticides. d Results from studies that reported effects of insecticides
Cohort studies and registriesThe following section presents cohort and registry studies. Because of their purely observational nature and the heterogeneity of study design, a GRADE rating was not performed. The results of these studies are presented in Table 2.
Fig. 2
Forest plots showing results of individual pesticide with three or more studies available. The plots shows the odds ratios with the error bars indicating the 95% confidence intervals. For the quaternary ammonium paraquat (a), most data were available. Other studies reported on the insecticide rotenone (b), the pyrethroid permethrin (c), the organophosphates chlorpyrifos (d), diazinon (e), and parathion (f), the organochloride lindane (g), the benzimidazole benomyl (h), and the dithiocarbamate maneb (i)
PAQUID study in FranceIn prospective cohort study from France, which enrolled participants from 1987 to 1998, the authors investigated individuals aged over 65 years at inclusion. In total, 1507 participants were enrolled, of whom 320 reported pesticide exposure. During follow-up, a significant association was observed between PD incidence and occupational pesticide exposure, but only in men (OR 5.63; 95% CI 1.47–21.58), with no significant association in women (OR 1.02; 95% CI 0.11–4.82). Interestingly, more women (922) than men (585) were included in this study (Baldi et al. 2003b).
French agricultural cohort AGRICAN, Mutualité sociale agricole (MSA)The AGICAN cohort enrolled all active and retired agricultural workers between 2005 and 2007. In the French health system, all agricultural workers are affiliated with the Mutualité Sociale Agricole (MSA), the agicultural health insurance provider. In AGRICAN, data of 1,728 self-reported PD cases and 148,078 healthy controls were analyzed. Pesticide exposure was assessed using the crop-exposure-matrix PESTIMAT (Pouchieu et al. 2018), which is based on annual reports about crops and active pesticide agents (Baldi et al. 2017). The authors reported increased PD risk among individuals with a history of pesticide poisoning (OR 1.51; 95% CI 1.14–1.99 for once poisoning; OR 2.25; 95% CI 1.52–3.38 for multiple poisonings). They also found significantly elevated risks associated with exposure to several dithiocarbamates (ORs 1.31–1.52; 95% CI from 1.08–1.60–1.26–1.83), rotenone (OR 1.57; 95% CI 1.08–2.29), paraquat (OR 1.43; 95% CI 1.17–1.75), and diquat (OR 1.39; 95% CI 1.14–1,68) (Pouchieu et al. 2018).
Another French study used the French National Health Insurance database–identify individuals reimbursed for antiparkinsonian drugs between 2009 and 2015. Newly diagnosed PD cases were identified via algorithm and filtered by MSA affiliation. In total, 10,282 PD cases were analyzed, and pesticide expenditures were stratified by farming type. A significantly increased PD incidence was found in vineyards areas with high pesticide expenditures (incidence rate ratio (IRR): 1.16, 95% CI 1.06–1.28), while no significant effect was observed for other types of farming (Perrin et al. 2021). This study is notable, because the French health system allowed a near-complete coverage of the French population during the observation period.
The TRACTOR project in FranceThe largest French epidemiological study, the TRACTOR project, analysed insurance data from 1,088,561 farm managers, betweeb 2002 and 2016. Among these, 8,845 developed PD (Petit et al. 2025). Harzard ratios (HRs) for PD incidence were calculated across different agricultural activities. Arboriculture, pig farming, dairy farming, mixed cattle farming, and crop farming were associated with significantly elevated HRs (> 1.3). Other activities, including cow farming, truck farming, and mixed or unspecific farming, showed moderately elevated HRs (> 1, < 1.2). Trends towards increased HRs were alss observed for viticulture and ovine/caprine farming. By contrast, gardening, landscaping, and reforestation, and small animal farming, were associated with reduced HRs (Petit et al. 2025).
Italian longitudinal study on aging (ILSA)The ILSA investigated randomly selected individuals aged 65–84 years across eight Italian regions in March 1992. Of 44,737 individuals, approximately 5,000 were screened for PD, and 113 PD cases were identified. The authors examined several risk factors and reported increased PD risk among persons holding a pesticide-use license (OR 3.68; 95% CI 1.57–8.64). However, only 7 PD cases and 83 controls possessed such a license, limiting meaningfulness (Baldereschi et al. 2003).
Netherlands cohort study on diet and cancerThe Netherlands Cohort Study on diet and cancer enrolled 120,852 individuals aged 55–69 years in 1986. In a follow-up analysis, PD-related deaths were assessed up to 2003. Pesticide exposure was estimated using a job-exposure-matrix and stratified into low and high exposure and cumulative exposure. In total, 402 PD-related deaths occurred in men and 207 in women. Trends towards increased PD mortality were observed (low exposure: HR 1.35; 95% CI 0.81–2.26), high exposure: HR 1.27; 95% CI 0.86–1.88). Significantly increased PD mortality was found in the group with the shortest cumulative exposure 1 to 27 unit years; HR: 1.89; 95% CI 1.11–3.22), whereas longer exposure durations did not yield a significant associations (Brouwer et al. 2015). This is particularly interesting, because the case numbers in the different exposure groups were comparable.
The agricultural health study (AHS)The AHS, initiated in the 1990 s in Iowa and North Carolina, USA, is a prospective observational study of pesticide users and their spouses (Alavanja et al. 1996). Exposure was assessed by questionnaires. Both prevalent PD at baseline (1993–1997) and incident PD during follow-up (1999–2003) were analyzed (Kamel et al. 2007). Interestingly, the study observed inverse trends between pesticide use and PD prevalence. Among never pesticide use, 15 PD cases occurred among 13,837 individuals, whereas 67 cases occurred among 65,183 pesticide users (OR 0.5; 95% CI 0.2–1.1). Similar non-significant trends were observed with pesticide mixing and application. When cumulative lifetime days of exposure were assessed, higher exposure groups showed no increased prevalence (65–200 days: 0.7; 95% CI 0.3–1.3; 201–396 days: 0.7; 95% CI 0.4–1.4; ≥ 397 days: 0.8; 95% CI 0.4–1.5) compared–individuals with 0–64 days of pesticide exposure, but PD incidence was elevated among those with ≥ 397 exposure days (OR 2.3; 95% CI 1.2–4.5). PD incidence was also linked–specific pesticide-related tasks (mixing pesticides > 50% of the time: OR 1.2; 95% CI 0.5–2.7; pesticide application: <50% of the time: OR 1.2; 95% CI 0.5–3.1; >50% of the time; OR 1.9; 95% CI 0.7–4.7). Compound-specific analyses revealed increased PD prevalence with several herbicides, including paraquat, a quaternary ammonium compound (OR 1.8; 95% CI 1.0–3.4), and cyanazine, a triazine (OR 2.6; 95% CI 1.4–4.9) and a trend (OR ≥ 1.4) for pendimethalin, a dinitroaniline (OR 1.4; 95% CI 0.8–2.6). Regarding PD incidence, increased risks were found for trifuralin, a dinitroaniline (OR 1.7; 95% CI 1.0–3.2), and 2,4,5-trichlorophenoxyacetic acid (OR 1.8; 95% CI 1.0–3.3) and a trend for butylate, a thiocarbamate (OR 1.4; 0.8–2.5). In the group of insecticides, trends towards a higher PD incidence were observed with exposure–lindane, an organochloride (OR 1.4; 95% CI 0.8–2.5), and phorate, an organothiophosphate (OR 1.4; 95% CI 0.8–2.5). Among fungicides, similar trends were observed with chlorothalonil, an aromatic compound (OR 2.0; 95% CI 0.9–4.4), and benomyl, a benzimidazole (OR 1.7; 95% CI 0.7–3.7). However, none of the insecticides or fungicides were associated with a statistically significant increased PD prevalence or incidence (Kamel et al. 2007). In a follow-up analysis, 66,110 individuals were included, of which 491 w
Comments (0)