PTBD often presents a more complex clinical and pathophysiological scenario than the alterations associated with CKD-MBD. In de novo KTRs treated with a steroid minimization immunosuppressive protocol, BMD changes especially in the first post-transplant year are highly variable, with 30–40% of patients showing substantial bone loss. Decreasing levels of PTH and bone turnover markers within the first 3 months post-transplant are associated with reduced BMD loss, and in some cases even BMD gain. Conversely, persistently elevated bone resorption markers throughout the first post-transplant year are linked to greater BMD loss. Delayed mineralization is present in KTRs in a variable range between 22 and 88%. This variability is related to the definition used in the studies to describe abnormal mineralization and with no clear trends in mineralization depending on the time since transplantation [22,23,24,25].
Although in KTRs, osteomalacia often results from vitamin D deficiency pre-existing to the kidney transplant, immunosuppression may influence the vitamin D metabolism [26]. Jorgensen et al. reported that commonly used immunosuppressive agents can adversely affect bone metabolism [25]. Glucocorticoids enhance the activity of 24-hydroxylase; this leads to reduced levels of 1,25-dihydroxyvitamin D. Additionally, glucocorticoids may downregulate VDR expression, thereby inducing a state of vitamin D resistance [4, 16, 25, 27].
Calcineurin inhibitors, such as cyclosporine A and tacrolimus, impair vitamin D metabolism by suppressing VDR expression in the kidney, leading to decreased expression of vitamin D-dependent calcium-binding proteins [19]. This suppression results in kidney calcium wasting despite elevated plasma levels of 1,25(OH)2D, suggesting a state of vitamin D resistance. Furthermore, both calcineurin inhibitors and 1,25(OH)2D are substrates of the cytochrome P450 enzyme CYP3A4. Collectively, these alterations contribute to an increased risk of bone disease and underscore the importance of tailored vitamin D supplementation in immunosuppressed populations [28].
Vitamin D deficiency results in hypocalcemia, hypophosphatemia, bone loss, deranged bone turnover, and mineralization. Osteomalacia is characterized by the accumulation of unmineralized osteoid, leading to bone softening and reduced strength. In severe cases, mineralization may halt completely, but lesions can reverse with correction of metabolic abnormalities [23, 24]. Hypophosphatemia and vitamin D deficiency often coexist in KTRs, and both contribute to osteomalacia: adequate PO4 and vitamin D levels are necessary for normal biomineralization [29]. In KTRs, histomorphometry findings often show increased osteoid volume and a higher likelihood of delayed mineralization as compared with patients with normal phosphate levels [22, 26].
Hypophosphatemia occurs in the early months following kidney transplantation, often due to persistent hyperparathyroidism and elevated FGF23 levels, which increase urinary phosphate excretion [3]. These abnormalities usually resolve within one year, but can contribute to osteomalacia by reducing phosphate availability for bone mineralization. FGF23 also suppresses 1α-hydroxylase and induces 24-hydroxylase, leading to lower active vitamin D levels, while PTH exerts the opposite effect. In our patient, hypophosphatemia related to high PTH, vitamin D deficiency, probable excess FGF23, likely amplified the metabolic milieu for osteomalacia [14, 15].
Although vitamin D deficiency is common in KTRs and can contribute to osteomalacia, it is often overlooked if hypercalcemia is present, and in this circumstance its supplementation is avoided. Moreover, persistence of this deficiency is clinically relevant since the coexistence with hyperparathyroidism may worsen skeletal fragility despite normalized kidney function [23, 25, 27].
Hypercalcemic hyperparathyroidism and widespread bone and joint pain (four months after kidney transplant) are the causes for patient referral to our clinic dedicated to bone and mineral disease. The coexistence of hypercalcemia and hyperparathyroidism is considered a distinct though less frequent (21.5%) phenotype of persistent hyperparathyroidism, referred to as tertiary hyperparathyroidism [25]. Moreover, it must be emphasized that hypercalcemic hyperparathyroidism may not necessarily be an expression of high skeletal remodeling but may be related to increased renal calcium reabsorption (lower levels of calciuria): the mechanisms underlying this atypical presentation remain currently unknown [28,29,30,31].
Clinically, osteomalacia manifests as diffuse skeletal pain, proximal myopathy, fractures of ribs/vertebrae/femoral neck, gait disturbance, and in severe cases, deformities; electrolyte imbalances may cause neuromuscular irritability [29, 32].
Radiographic signs of osteomalacia are discrete and appear in combination with other characteristic features of kidney bone disease. In osteomalacia, bone density is decreased, with loss of definition of the cortical bone and swelling of trabecular pattern. A rare but pathognomonic feature is the presence of Looser’s zones (i.e., Milkman’s fractures, pseudofractures), which are more common in the medial part of the femoral neck, pubic rami, ilii, scapulae, ribs, and acromion. Looser’s zones represent unmineralized osteoid and are seen as lucent symmetric lines perpendicular to the cortex; typically radiolucent lines do not extend across the whole width of the bone unless the fracture has occurred through it [33].
In osteomalacia, imaging techniques such as DEXA, vertebral morphometry, and MRI can support the diagnosis, although none are specific when used alone. DEXA typically shows reduced BMD in the spine, hips, or forearm; however, it cannot reliably distinguish osteomalacia from osteoporosis [29].
Subchondral insufficiency fractures may also be observed in weight-bearing joints, such as the knees. Vertebral morphometry may show biconcave or “codfish” vertebrae in chronic cases, although vertebral fractures are less frequent than in osteoporosis and early disease can present only with subtle vertebral height loss [34].
In our patient, due to the clinical worsening with progressive inability to ambulate independently, an MRI was performed following orthopedic recommendation, revealing diffuse bone marrow edema involving the patella, tibial plateaus, and femoral condyles. MRI may reveal bone marrow edema—which frequently occurs in various bone pathologies, appearing as high signal intensity on STIR or T2-weighted images—and bilateral.
In the patient described in this case report, several differential diagnoses were considered and excluded, including arthropathies, infection, osteonecrosis, and neoplastic lesions, based on clinical, laboratory, and imaging findings [35,36,37]. Although bone biopsy remains the gold standard, it was not performed. The combination of characteristic radiologic features (Looser’s zones, bone marrow edema), severe vitamin D deficiency, hypophosphatemia, elevated bone turnover markers, and the rapid clinical and imaging improvement after vitamin D supplementation supported osteomalacia as a major contributor. However, the overall clinical presentation was likely due to a combination of osteomalacia and persistent hyperparathyroid bone disease, both of which were addressed through treatment of vitamin D deficiency and post-transplant hyperparathyroidism.
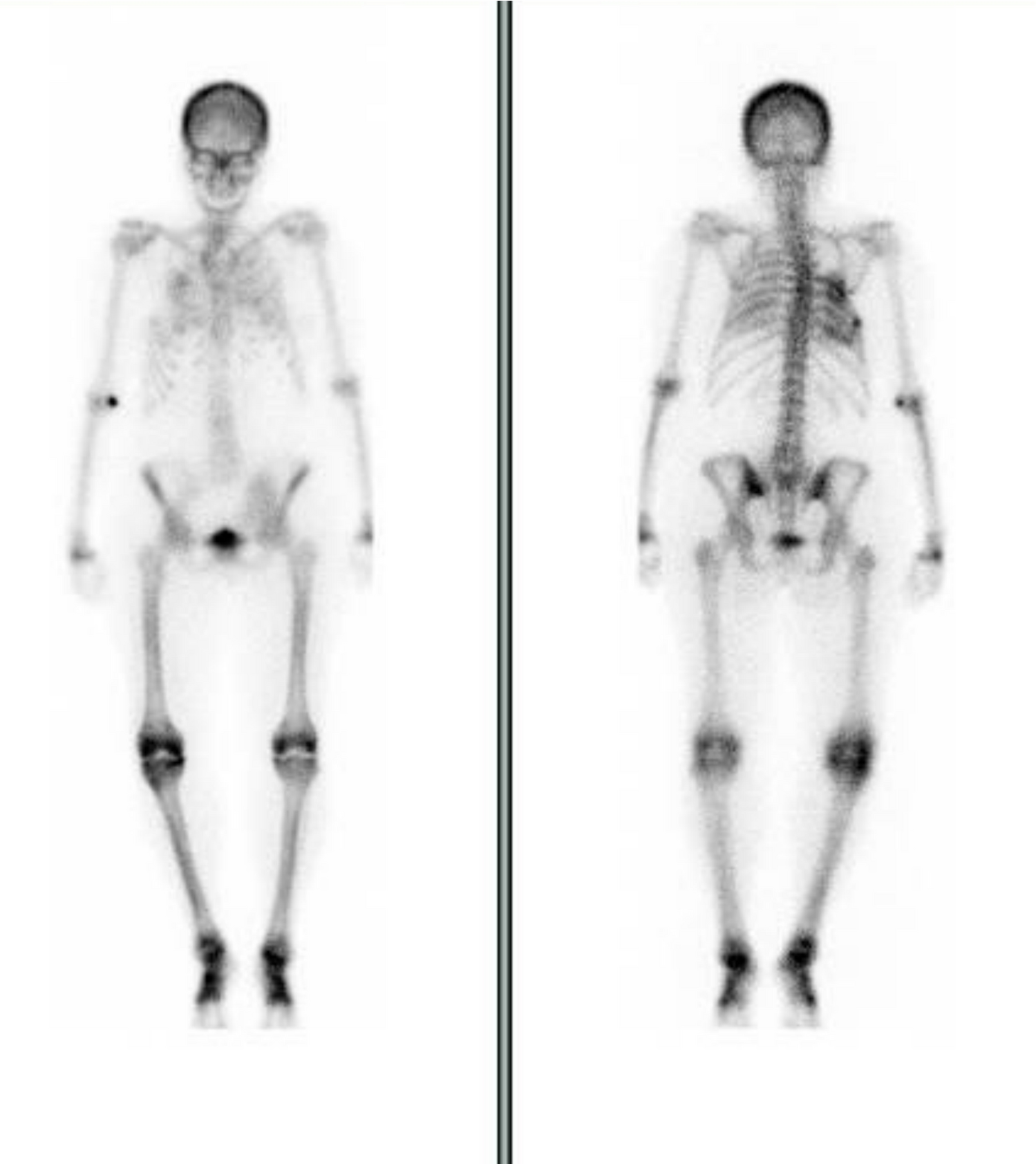
In summary, bone marrow edema is not a primary pathology but rather a shared radiologic manifestation of underlying bone weakness and varied pathologies, highlighting the need to evaluate and address the root causes of reduced bone quality in affected patients (Table 3) [38, 39]. In our patient, the post‑transplant bone disease was not attributable to a single mechanism. The persistent hyperparathyroidism, already present before transplantation, continued to drive high‑turnover bone disease after engraftment. At the same time, the inappropriate suspension of native vitamin D supplementation and the introduction of glucocorticoids unveiled a significant pre‑existing vitamin D deficiency. This combination created the metabolic setting for osteomalacia to emerge, as confirmed by imaging and bone turnover markers. Therefore, the skeletal involvement in this case should be interpreted as the consequence of both persistent hyperparathyroidism and superimposed osteomalacia, rather than being explained by one mechanism alone. Due to the persistence of bone pain and in the absence of specific clinical or radiological signs of metabolic bone disease, skeletal scintigraphy was performed to rule out Paget’s disease. Skeletal scintigraphy with 99mTc-MDP revealed a focal area of radiotracer hyperaccumulation near the lateral wall of the right fourth rib, with no other significant areas of increased uptake suggestive of multifocal lesions or Paget’s disease .
Table 3 Types of osteomalaciaOsteomalacia is also a common cause of metabolic superscan, a characteristic bone scan pattern seen in various metabolic bone diseases [36]. This pattern is marked by diffuse and intense uptake of the radiotracer throughout the skeleton. Despite decreased bone mineralization in patients with osteomalacia, osteoid formation, calcium deposition, bone turnover, and PTH levels are increased and cause superscan patterns. Additionally, foci of increased uptake in pseudofractures (also known as Looser zones) can be observed in the femoral neck and scapula of patients [40].
An interesting finding in our case was the pattern of bone turnover markers before and after vitamin D treatment, reflecting coexistence of persistent hyperparathyroidism and vitamin D deficiency–related osteomalacia. Both conditions can elevate bone turnover markers, albeit with different mechanisms, and contribute to skeletal fragility; nevertheless, the rapid clinical and radiological improvement after vitamin D repletion suggests osteomalacia was the dominant factor in the acute presentation, while hyperparathyroidism persisted as a chronic background process. This distinction is important for the case interpretation and management in similar post-transplant scenarios.
DEXA and vertebral morphometry assess bone mass and detect subclinical fractures but cannot determine bone turnover, which is essential for identifying the disease phenotype and guiding therapy [41].
Emerging data suggest that bone turnover markers in CKD and KTRs might be used for the assessment of bone turnover, providing crucial insight into the dynamics of bone metabolism. To avoid bias related to kidney retention, in the setting of CKD, bone turnover markers that are not cleared by the kidneys, such as BALP, trimeric PINP1 and tartrate-resistant acid phosphatase-5b (TRAP-5b), must be considered and correlate more specifically with histological bone turnover in CKD compared to PTH alone. The use of PTH together with bone turnover markers improves the sensitivity and specificity of prediction models for both low and high bone turnover [41,42,43]. Monitoring their trend over time allowed us to evaluate therapeutic efficacy as well as patient compliance, helping to optimize therapy while minimizing the risk of adynamic bone disease [44, 45].
In our case, the clinical picture proved to be more complex than a classic vitamin D deficiency–related osteomalacia, as persistent hyperparathyroidism despite pharmacotherapy led to a simultaneous elevation of both bone formation and resorption markers and not to an isolated increase in BALP as typically seen in osteomalacia. Unfortunately, we were not able to determine PINP1 and TRAP-5b, as the assays were unavailable at that time. It can be postulated that the constellation of severe vitamin D deficiency, hypophosphatemia, imaging features such as Looser zones and bone marrow edema favored the diagnosis of osteomalacia rather than classic persistent hyperparathyroid bone disease. The underlying osteomalacia was likely already present in a subclinical form before transplantation and was unmasked and exacerbated by post‑transplant factors, including reduced sun exposure, steroid therapy, and discontinuation of vitamin D supplementation. The rapid clinical and radiological response to aggressive vitamin D replacement further supports osteomalacia as the predominant mechanism of bone fragility in this case.
The rationale for selecting solitary parathyroidectomy prior to transplantation remains unclear, particularly whether this choice was guided by preoperative findings or the identification of a single enlarged parathyroid gland, as the patient’s pre-transplant care was conducted at a different nephrology center.
In addition to severe vitamin D deficiency, the coexistence of a hypophosphatemia condition may have likely contributed to this patient’s onset of osteomalacia. These changes, including high FGF23, PTH, and increased urinary phosphate excretion (phosphaturia), typically resolve within a year post-transplant [14, 15]. Unfortunately, FGF23 was not measured; therefore, we cannot exclude that excess phosphatonin contributed to both vitamin D deficiency and hypophosphatemia.
The clinical presentation of osteomalacia is highly variable and often asymptomatic; however, in more severe cases, symptoms of hypocalcemia may appear along with marked muscle weakness and difficulty walking. The prevalence of osteomalacia in patients with advanced CKD and KTRs is probably much more frequent than expected. It is a fact that in KTRs bone biopsy studies, the presence of focal or generalized osteomalacia was surprisingly widespread even if the calcitriol levels were normal [20]. In the case described here, vitamin D deficiency was documented prior to transplantation and was likely longstanding. The effect of immunosuppressive therapy on this condition of severe vitamin D deficiency was evident, which might have contributed further, alongside the inappropriate discontinuation of cholecalciferol. The consensual presence of hypophosphatemia with multifactorial genesis (high PTH and FGF23 levels, vitamin D deficiency) feasibly played a further role in the onset of osteomalacia. It is important to underline that the observed improvement in biochemical and clinical parameters should not be attributed to vitamin D supplementation alone. In this case, the ongoing therapy with cinacalcet contributed significantly to the early control of hyperparathyroidism and hypercalcemia, while the later initiation of bisphosphonate treatment further supported the consolidation of bone metabolism and stabilization of BMD.
The evidence clearly indicates that vitamin D supplementation exerts a favorable effect on bone outcomes after kidney transplantation, likely mediated through improved control of hyperparathyroidism.
The target to be achieved in patients with CKD as well as KTRs remains a matter of debate. Our case suggests that preventing or correcting vitamin D deficiency in KTRs is likely a mandatory approach, given their unique pathophysiological and clinical profile and the heightened risk they face from the consequences of vitamin D deficiency. Given the vitamin D deficiency present in many transplant candidates, its identification and correction should be systematic and timely, in a clinical and pathophysiological context that inherently accentuates its severity. Similarly, the therapeutic regimen should not be limited to the simple correction of vitamin D deficiency but should be extended to all the complex alterations of mineral metabolism present in KTRs.

Comments (0)