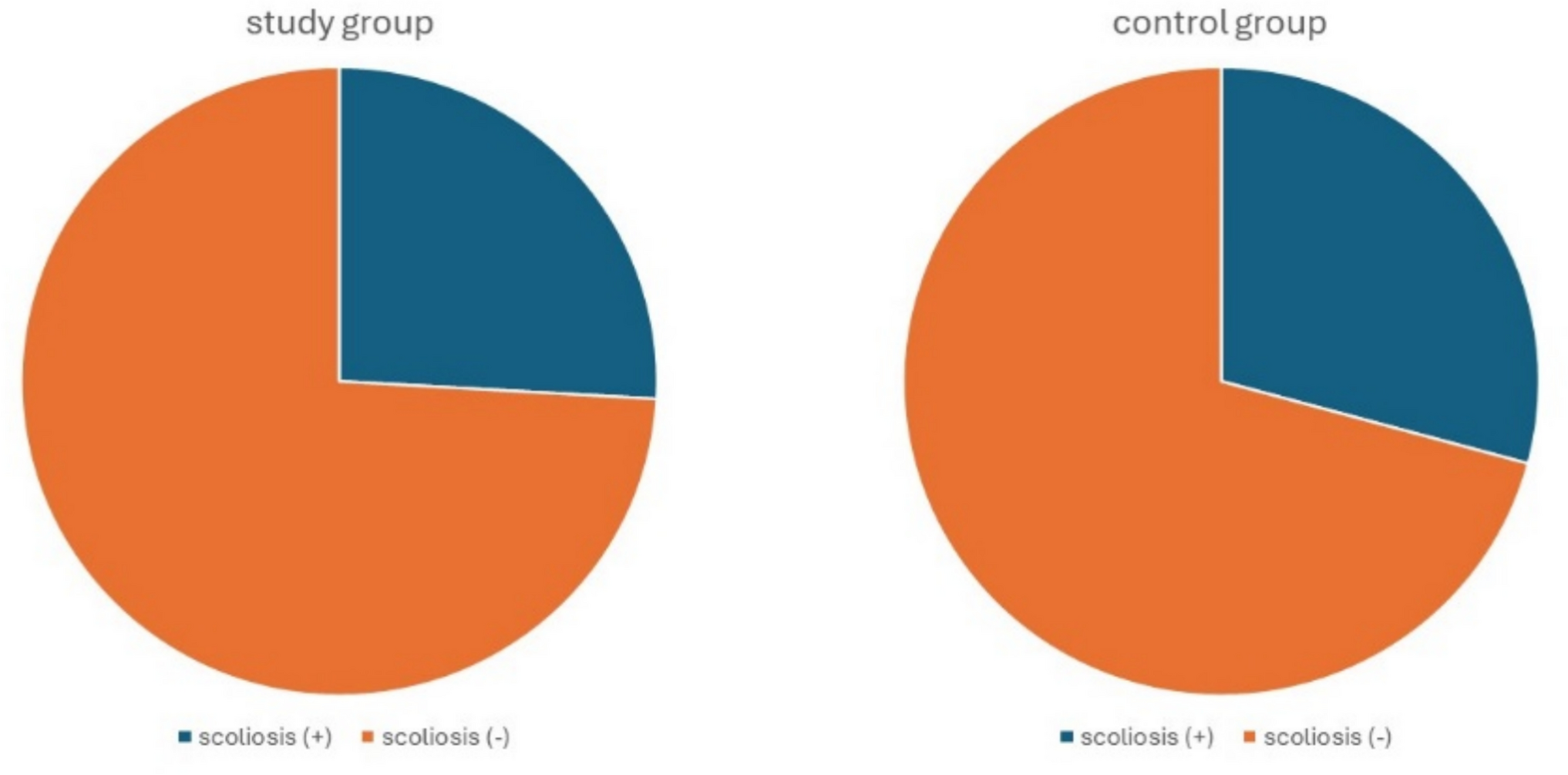
Our hypothesis that ADPKD may be associated with an increased prevalence of scoliosis was supported by the fact that in both clinical entities, disorders of connective tissue are present [7, 8]. Additionally, enlargement of kidneys and liver in ADPKD, which is often asymmetric, may lead to chronic postural alteration [10]. Moreover, disorders of calcium and phosphate metabolism are involved in the development of scoliosis [11]. Hypophosphatemia and suppressed bone formation were observed in children with ADPKD and preserved renal function [12]. Furthermore, in contrast to other etiologies of chronic kidney disease (CKD), in ADPKD bone defects has been observed already at early stages of CKD [13]. It was also shown that patients with ADPKD have lower bone turnover and better preserved cortical bone mineral density compared to patients with ESKD of different etiology [14]. Lastly, patients with co-existence of ADPKD and scoliosis were reported in the literature [9, 15]. Taking these facts together, suspicion of higher risk for scoliosis development in ADPKD compared to other conditions leading to CKD seemed reasonable. However, despite metabolic disorders, the incidence of fractures in ADPKD patients with ESKD is not different compared to other diseases leading to ESKD [13]. Similarly, we failed to show that ADPKD is associated with increased risk for scoliosis development; according to our results (Fig. 1), the prevalence of scoliosis is not different in patients with ADPKD compared to non-ADPKD controls.
Data on the epidemiology of scoliosis in Poland are limited. Among urban children and adolescents, scoliosis was observed in 14.6–22.2% of boys, and 17–25.7% of girls, depending on the method of assessment [16]. Scoliosis prevalence in the population of our study was higher, what may be attributable to adult degenerative scoliosis, which develops after 40 year of age [17], and may progress with age [18]. However, according to our analysis, the prevalence of scoliosis was not increased in renal transplant patients after 60 year of age, compared to younger subjects, neither in ADPKD group, nor in non-ADPKD group. It should be noted that the median age of the study group was higher compared to the control group. It can be explained by the fact that in ADPKD, ESKD develops relatively late; the median age at which ESKD appears is 58 years in type 1 and 79 years in type 2 of the disease [19]. On the other hand, in other diseases leading to ESKD and being indications for renal transplantation, the age of ESKD development may be lower. As a result, the median age of renal transplant recipients with ADPKD may be higher compared to those without ADPKD. However, according to our analysis, the age was not associated with the prevalence of scoliosis in included population.
All patients included in our study were Caucasians. It was due to the fact that the Polish population contains only an infinitesimal percent of other races. However, it may limit the possibility of generalization of our results because race counts for the prevalence of scoliosis [20].
Renal function was comparable between the study group and the control group. We did not observe an association between renal function, and scoliosis prevalence. As far as we know, association between scoliosis development and renal function has never been reported [20].
Scoliosis was more common in female compared to male patients. In multivariable analysis, female sex remained a significant predictor of scoliosis. It is in line with the current knowledge, according to which scoliosis is more frequent in women [8, 20].
In addition to the above-mentioned limitations, it should be noted that some factors that may be of importance for the development of scoliosis were omitted in our analysis due to its preliminary character, e.g., body mass index, environmental factors, and lifestyle [20]. We feel that lack of data on parathyroid hormone, alkaline phosphatase, vitamin D, calcium, and phosphorus levels is the major limitation of our analysis; however, they were omitted due to the incompleteness of the data on these factors. Moreover, most probably, levels of these factors at random time could be of low significance; and only levels of these parameters at the moment preceding scoliosis development, or progression, would be significant in our analysis. However, we did not record the time of scoliosis development, or progression, in our study. Additionally, data on the type of mutation responsible for ADPKD occurrence were lacking, and therefore, they were not analyzed. There are over 1400 mutations that may cause ADPKD [21], and it could not be excluded that only some of them may be associated with increased risk of scoliosis. Moreover, data on the size of kidneys and liver in patients with ADPKD were omitted in our analysis due to their incompletness. It could not be excluded that the risk of scoliosis development may be increased in patients with liver enlargement, or significant asymmetry in the size of kidneys. Therefore, we think that further studies are needed to examine the role of above factors.

Comments (0)