No significant difference was found after lobar radioembolization compared to baseline in SULmean in both treated and untreated non-tumorous liver regions. The SULmean ratio between treated and untreated lobes did not differ posttreatment either. While dosimetry is critical for ensuring safety and effective radiation delivery, non-tumorous liver absorbed dose does not appear to evidently impact liver metabolism as reflected by SUL on [18F]FDG-PET-CT following 90Y-glass microsphere radioembolization.
The results of this study tend to support the retrospective study of Bienert et al. [16]. Their analysis included five patients and found no difference in [18F]FDG-uptake in the treated compared to the untreated non-tumorous liver tissue after 90Y-resin radioembolization. Although Nakahara et al. [17] described an increased [18F]FDG-uptake in their case report at 26 days after external beam radiation therapy, this finding normalized after 4 months. Therefore, it is possible that the [18F]FDG-uptake returned to its previous state by the time of the follow-up [18F]FDG-PET-CT scan in this analysis, three months after treatment. However, it should be noted that in contrast to external beam radiotherapy, which delivers a homogeneous radiation dose, radioembolization results in a heterogeneous dose distribution within the targeted liver. This variability may influence the timeline and pattern of metabolic changes observed on [18F]FDG-PET-CT. Furthermore, a mildly positive correlation was observed between the SULprior and SULpost in both the treated and untreated liver parenchyma. This correlation suggests that in both lobes, there is a relationship between changes in liver metabolism and treatment. When correlating the ratio (SULmean in treated liver divided by SULmean in untreated liver) before and after radioembolization, the correlation was smaller and no longer statistically significant. This could indicate that while both lobes respond to unilobar radioembolization, the extent of metabolic changes in the treated/untreated liver varies among patients.
Comparison of [18F]FDG-uptake in the liver with previous reported data is challenging, because of different ways of quantification or correction of liver [18F]FDG-uptake. These variations include, e.g., use of different VOIs; use of SUVmax, SUVmean or TLG; or various correction methods, including body surface area (BSA), body weight or LBM (SUL). VOI size is of relevance as SUVs measured in a larger and fixed VOI are more reproducible and precise than using a smaller VOI [18]. Spheric VOIs with a diameter Of 3 cm are sufficient for measuring SUVmean [19], similarly to the approach used in this study. SUL was chosen in this study, as this correction method is more consistent from patient to patient than body weight [20] or BSA [21]. In addition, this is not affected by clinical parameters, i.e., age, sex, blood glucose level or diabetes [22,23,24].
In a retrospective review by Viner et al. [20] including 116 patients, who had undergone an [18F]FDG-PET-CT for oncologic staging, the liver SULmean values had low interreader and intersite variability, regardless of VOI placement within the right liver lobe. The intraclass correlation coefficients (ICC) of SULmean, adjusted for readers, were 0.986 (95%CI 0.98, 0.991; p = 0.0001) for reader 1 and 0.987 (95%CI 0.981, 0.991; p = 0.0001) for reader 2. When adjusted for location, the ICC for SULmean measurements by two readers were 0.986 (95%CI: 0.979–0.99) at the upper level and 0.98 (95%CI 0.971–0.986) at the lower level. This demonstrates that the method used in the current study, VOI placement in non-tumorous liver tissue, is a robust measurement with low interobserver variability. While automated VOI placement tools can enhance efficiency, their outputs should not be accepted without careful review. Reader experience by reporting physicians remains crucial when assessing liver uptake on [18F]FDG-PET-CT. Misplacement due to tumor involvement or artifacts may lead to inaccurate SUL measurements. In this study, all VOIs were manually reviewed and adjusted as needed. (Supplemental Fig. 1).
Prior received systemic therapy may introduce changes in SUVmean measurements and therefore SUL, as was described in patients with lymphoma treated with chemotherapy, but that is also reported to resolve over time [25,26,27]. Taking the results Of this study and previous reports into consideration, the liver seems adequate as a reference at 3 months posttreatment for the assessment of metabolic response on [18F]FDG-PET-CT following radioembolization.
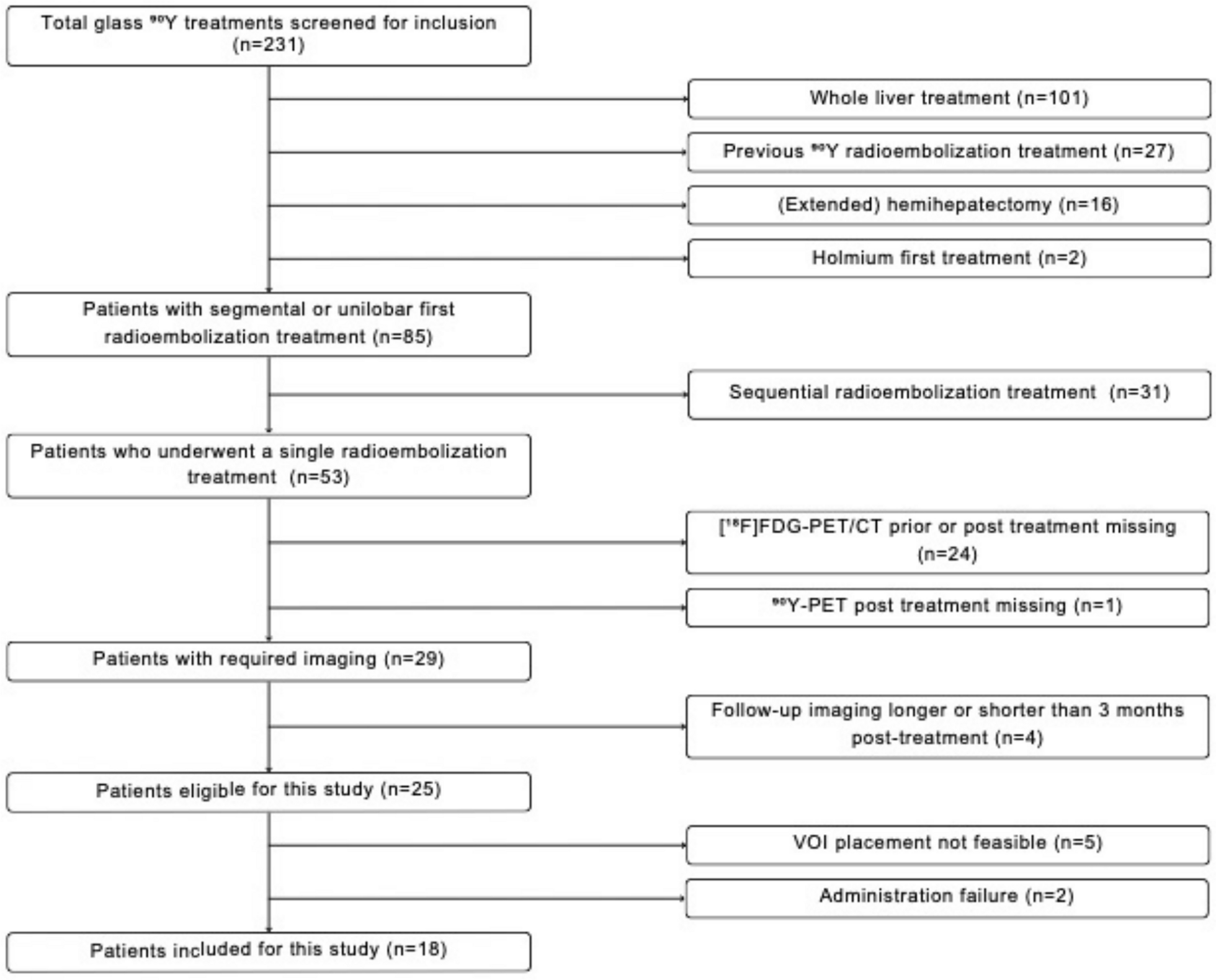
This study has several limitations. Firstly, although approximately 200 patients were screened for this study, only a limited number of patients met all study criteria, leading to a small sample size. This limitation does affect the statistical power and limits generalizability of the results. Secondly, the quantitative results of [18F]FDG-PET-CT depend On e.g., hardware, image acquisitions, reconstruction and analyses. As treatments and imaging data Over 15 years were included in the analyses, improvements in imaging techniques and PET scanners may introduce variability in SUL measurements [28]. However, in this monocenter study all imaging studies were performed with the same accredited image acquisition and reconstruction protocols (EARL). In addition, the [18F]FDG-PET-CT analyses were semi-automated and corrected by one researcher (LSH) under supervision of an experienced nuclear physician (AB, > 10 years experience). Therefore, we have limited the effect of technical differences. Thirdly, the sample size of this study was too small to correct for confounding factors, like previous systemic therapies and potential underlying liver disease (chemotherapy induced liver steatosis).
Future larger studies incorporating [18F]FDG-PET-CT before and after radioembolization should investigate metabolic changes Over time before the 3-month time-point and the influence of other factors, like systemic therapies. In addition, prospective studies should incorporate the use of [18F]FDG-PET-CT and PERCIST as response assessment after radioembolization, to further validate its use.



Comments (0)