2.1 Pharmacodynamics
Gepotidacin has a dual targeting mechanism of action and inhibits DNA replication by inhibiting Type II topoisomerases [including bacterial topoisomerase II (DNA gyrase) and topoisomerase IV] that play a role in bacterial replication [8]. In vitro, gepotidacin displayed well-balanced dual-targeting of gyrase and topoisomerase IV in E. coli cells. Gepotidacin induced gyrase/topoisomerase IV-mediated single-stranded, but not double-stranded, DNA breaks [11].
In vitro and in clinical studies, gepotidacin showed activity against most isolates of E. faecalis, S. saprophyticus, C. freundii complex, E. coli, K. pneumoniae and N. gonorrhoeae [8]. In vitro, gepotidacin showed activity against clinical isolates of E. coli [6031 isolates, including nitrofurantoin-resistant, fosfomycin-resistant, extended-spectrum β-lactamase (ESBL) screen-positive, and multi-drug-resistant (MDR)] (MIC90 2–4 mg/L) [12,13,14,15], K. pneumoniae (1608 isolates, including ESBL-producing and MDR) [MIC90 8–32 mg/L] [16, 17], S. saprophyticus (436 isolates) [MIC90 0.12 mg/L] [13, 15] and N. gonorrhoeae (346 isolates, including MDR) [MIC90 0.25–1 mg/L] [18,19,20].
Gepotidacin also showed activity (MIC90 ≤ the susceptible breakpoint for gepotidacin against isolates of similar genus or organism group) against other aerobic bacteria, including C. koseri, K. aerogenes, K.oxytoca/Raoltella ornithinolytica, Morganella morganii, Proteus mirabilis and Providencia rettgeri; however, gepotidacin efficacy in treating clinical infections caused by these organisms has not been established in clinical trials [8].
In time-kill studies, gepotidacin showed bactericidal activity against a range of pathogens [8]. In vitro studies demonstrated a gepotidacin post-antibiotic effect of 1.8– 2.2 h for E. coli, 1.0 to > 6.6 h for K. pneumoniae, 1.4–3.0 h for P. mirabilis, 1.0–2.6 h for C. freundii complex, 2.7–4.3 h for S. saprophyticus, 1.2–2.7 h for E. faecalis and 0.7–1.0 h for N. gonorrhoeae at 5 x the MIC [8, 20].
The 24-h free-drug AUC/MIC ratio (fAUC24/MIC) has been shown in animal infection and in vitro PK-PD models to be the index predictive of gepotidacin antibacterial efficacy [8, 21,22,23]. In vitro, the median gepotidacin fAUC24/MIC associated with net bacterial stasis and 1- and 2-log10 CFU reductions in E. coli isolates (gepotidacin MIC 1–4 mg/L) was 33.9, 43.7 and 60.7, respectively [23]. In a 10-day E. coli (gepotidacin MIC 2 mg/L) hollow-fiber in vitro infection model, gepotidacin fAUC24/MIC ≥ 275 suppressed on-therapy resistance amplification [23]. In a 7-day N. gonorrhoeae hollow-fiber in vitro infection model, single- or divided-dose gepotidacin regimens totalling ≥ least 4.5 g prevented on-therapy resistance amplification and sterilized the model system [22]. In a phase 2 clinical trial of gepotidacin in uUGC (NCT02294682), fAUC24/MICs ≥ 48 predicted 100% microbiological success [19].
In vitro, no antagonism against Enterobacterales or gram-positive isolates was observed for gepotidacin in combination with other antibacterials, including fluoroquinolones, sulfonamides, cephalosporins, macrolides, tetracyclines, aminoglycosides, glycopeptides, carbapenems, nitrofurans, monobactams, and oxazolidinones [8].
While no clear mechanisms for gepotidacin resistance have been identified, potential mechanisms include gepotidacin-specific alterations of DNA gyrase (gyrA, gyrB) and/or topoisomerase IV (parC, parE) gene targets, plasmid-mediated quinolone resistance genes (especially qnr), and efflux [8]. Amino acids that may be important for gepotidacin activity are: GyrA P35, V44, D82, A175, GyrB D426, P445 and ParC D79, as shown through studies with isogenic mutants in E. coli and K. pneumoniae. A single target-specific mutation may not significantly impact gepotidacin activity [8]; however, when mutations in GyrA and ParC amino acid residues that interact with gepotidacin were present in both DNA gyrase and topoisomerase IV, gepotidacin activity was reduced against a mutant E. coli strain in vitro [11]. The relationship between gepotidacin and fluoroquinolone susceptibility does not appear to include amino acid substitutions in gyrA and parC that are known to reduce fluoroquinolone susceptibility in E. coli. Gepotidacin activity against E. coli and K. pneumoniae is unrelated to beta-lactam resistance mechanisms [8].
The frequency of resistance development to gepotidacin due to spontaneous mutations in the gram-negative and gram-positive uropathogens tested in vitro at 10 times MIC ranged from 10−9 to 10−10 [8]. Target-specific cross-resistance with other classes of antibacterial drugs has not been identified; consequently, isolates resistant to other drugs may be susceptible to gepotidacin. However, isolates of Enterobacterales with ≥4-fold increases in gepotidacin MIC have been identified in vitro and in clinical studies. During clinical studies, gepotidacin demonstrated activity against some isolates of the following multilocus sequence typing (MLST) for E. coli: ST10, ST131, ST1193, ST69, ST95 and ST73 [8]. Single-step resistance selection studies did not recover gepotidacin-resistant N. gonorrhoeae mutants (spontaneous single-step mutation rate < 1.25 × 10−9) [20]; however, in a phase 2 clinical trial of gepotidacin in uUGC (NCT02294682), resistance to gepotidacin (MICs increased ≥ 32-fold) emerged with additional GyrA A92T mutations in two N. gonorrhoeae isolates with a pre-existing ParC D86N mutation [19].
In a thorough QT study of IV gepotidacin (not an approved route of administration), a dose-related and concentration-dependent QTc prolongation effect of gepotidacin was evident; the dose used in the phase 3 trial was adjusted to address this issue. The mean placebo-corrected change from baseline QTcF values around Tmax were 12 msec with a 1000 mg IV infusion over 2 h and 22 msec with an 1800 mg IV dose. Gepotidacin Cmax after a single 1000 mg IV dose is ≈ 1.7 times greater than Cmax,ss for oral gepotidacin 1500 mg twice daily (approved dose and administration route) [8, 24].
2.2 Pharmacokinetics
The pharmacokinetics of oral gepotidacin are approximately dose proportional over a 1500–3000 mg dose range [8]. In patients with uUTI and normal renal function (eGFR ≥ 90 mL/min), steady state is achieved by day 3 of administration of gepotidacin 1500 mg every 12 h for 5 days. At steady state, mean Cmax is 4.2 µg/mL, Tmax is ≈ 2 h and mean AUC12 is 22.8 µg·h/mL. Accumulation of gepotidacin after oral administration is 40% and absolute bioavailability is ≈ 45%. Gepotidacin is ≈ 25% to ≈ 41% plasma protein bound and mean Vss is 172.9 L [8]. Gepotidacin is primarily metabolized by CYP34; the major metabolite is M4, which accounts for ≈ 11% of circulating drug-related materials. At steady state, mean t1/2 is 9.3 h and mean CL/F is 33.4 L/h. The major elimination route for absorbed gepotidacin route is via urine (≈ 31%; 20% as the unchanged drug). Gepotidacin is also excreted in faeces (≈ 52%; 30% as the unchanged drug) [8]. Clinically relevant increases in gepotidacin exposure are seen in patients with severe renal impairment or kidney failure (eGFR <30 mL/min) [Cmax and AUC 1.7-fold and 2.1-fold higher than matched healthy controls], including those receiving dialysis (Cmax and AUC 2.3-fold and 2.5-fold higher before intermittent haemodialysis and 6.2-fold and 4.2-fold higher after intermittent haemodialysis] and in patients with severe hepatic impairment (Child-Pugh Class C) [Cmax and AUC ≈ 1.9-fold and 1.7-fold higher] [8].
Features and properties of gepotidacin
Alternative names
Blujepa; GSK 2140944; GSK-2140944E
Class
Acenaphthenes; Anti-infectives; Antibacterials; Aza compounds; Ketones; Piperidines; Pyridines; Pyrones; Small molecules; Urinary anti-infective agents
Mechanism of action
DNA gyrase inhibitors; DNA topoisomerase IV inhibitors
Route of administration
Oral
Pharmacodynamics
In vitro and clinical activity against most isolates of E. faecalis, S. saprophyticus, C. freundii complex, E. coli, K. pneumoniae, N. gonorrhoeae
Dose- and concentration-dependent QTc prolongation observed
Pharmacokinetics
Cmax, 4.2 µg/mL, Tmax ≈ 2 h, AUC12 22.8 µg·h/mL, ≈ 25% to ≈ 41% plasma protein bound, Vss is 172.9 L, t1/2 9.3 h, CL/F 33.4 L/h, excreted via urine and faeces
Adverse events
Most frequent (incidence ≥ 1%)
Diarrhoea, nausea, abdominal pain, flatulence, headache, soft faeces, dizziness, vomiting, vulvovaginal candidiasis
ATC codes
WHO ATC code
J01 (Antibacterials for Systemic Use); R07 (Other Respiratory System Products)
EphMRA ATC code
J1 (Systemic Antibacterials); R7X (All Other Respiratory System Products)
Chemical name
(3R)-3-[[4-(3,4-dihydro-2H-pyrano[2,3-c]pyridin-6-ylmethylamino)piperidin-1-yl]methyl]-1,4,7-triazatricyclo[6.3.1.04,12]dodeca-6,8(12),9-triene-5,11-dione
Concomitant administration with strong CYP3A4 inhibitors increased gepotidacin Cmax and AUC ≈ 1.4-fold and ≈ 1.5-fold, respectively, and concomitant administration with strong CYP3A4 inducers decreased gepotidacin AUC∞ by 52% [8]. Drug-drug interaction simulation results suggest that gepotidacin AUC would decrease ≈ 50% when co-administered with a moderate CYP3A4 inducer [25]. Concomitant administration of gepotidacin with digoxin resulted in a 1.5-fold increase in the digoxin Cmax (at 3 h post dose), a 1.1-fold increase in the digoxin AUC∞ and a delayed digoxin Tmax. Concomitant administration with midazolam resulted in a 1.9-fold increase in midazolam AUC∞ [8]. In vitro, gepotidacin does not induce CYP1A2, CYP 2B6 or CYP 3A4 and is not a substrate of OATP1B1, OATP1B3, OATP2B1, OAT1, OAT2, OAT3, OCT2 and OCT3. In vitro, gepotidacin inhibited MATE1 and MATE2-K and is a substrate of BCRP [8].
2.3 Therapeutic Trials2.3.1 Uncomplicated Urinary Tract Infections
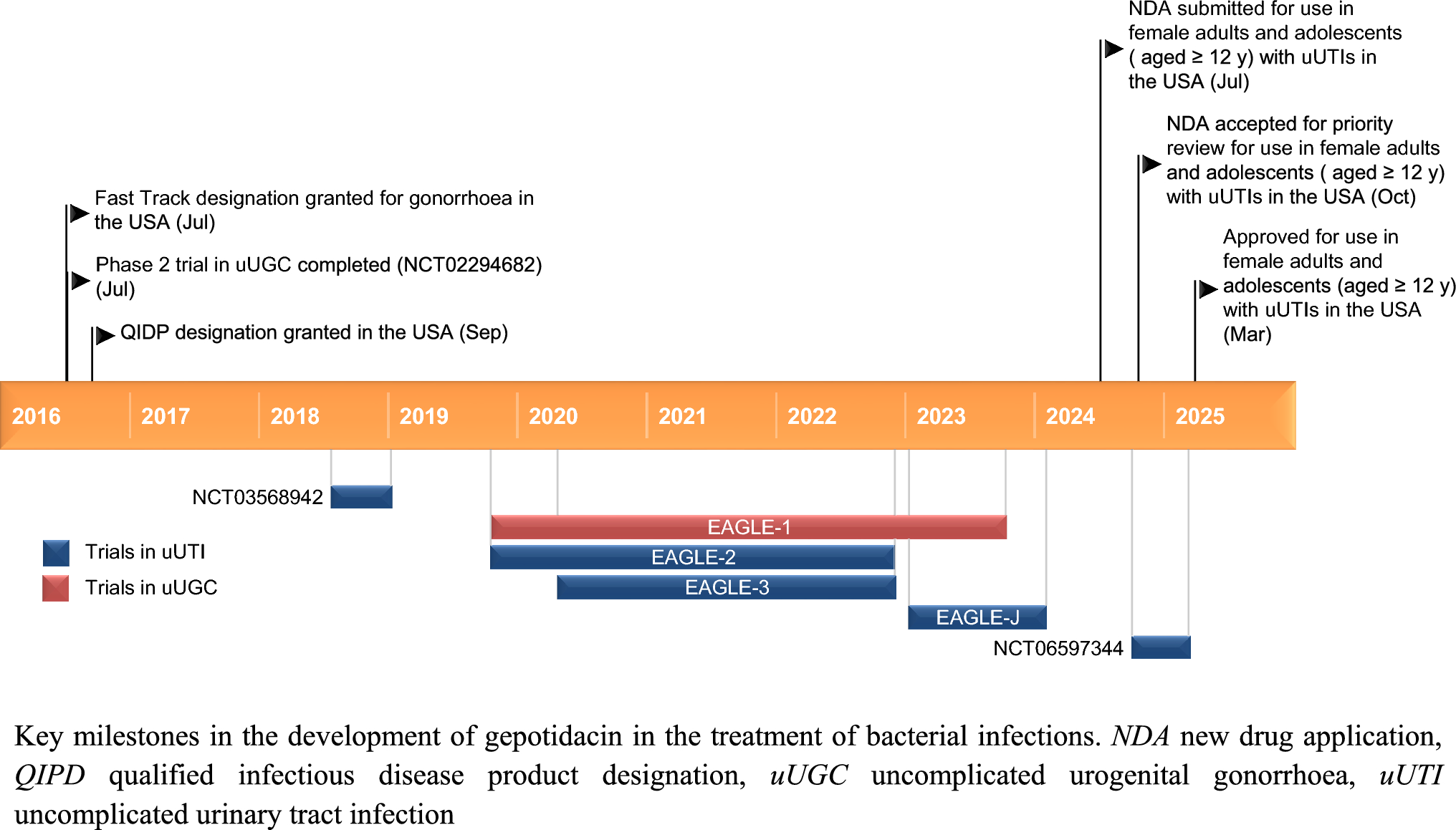
Gepotidacin showed efficacy in the treatment of uUTIs in female adult and paediatric patients aged ≥ 12 years in EAGLE-2 (NCT04020341), a randomised, double-blind, phase 3 comparison with nitrofurantoin [8, 26]. At the test-of-cure (TOC) visit (study days 10–13) in the microbiological intent-to-treat nitrofurantoin-susceptible (microITTS) population, gepotidacin (n = 336 evaluable) was noninferior (noninferiority margin 10%) to nitrofurantoin (n = 298 evaluable) in terms of the composite therapeutic response (51.8% vs 47.0%; treatment difference 5.3; 95% CI − 2.4 to 13.0) [primary endpoint]. A clinical cure was seen in 66.7% of gepotidacin recipients and 65.8% of nitrofurantoin recipients (treatment difference 1.5; 95% CI − 5.8 to 8.8) and a microbiological response was seen in 72.6% and 66.8% of patients in the respective treatment groups (treatment difference 6.0; 95% CI − 1.2 to 13.1) [8].
Gepotidacin showed efficacy in the treatment of uUTIs in female adult and paediatric patients aged ≥ 12 years in EAGLE-3 (NCT04187144), a randomised, double-blind, phase 3 comparison with nitrofurantoin [8, 26]. At the TOC visit (study days 10–13) in the microITTS population, treatment with oral gepotidacin (n = 292 evaluable) was noninferior (noninferiority margin 10%) and superior (p = 0.003) to oral nitrofurantoin 100 mg twice daily for 5 days (n = 275 evaluable) in terms of the composite therapeutic response (58.9% vs 44.0%; treatment difference 14.4; 95% CI 6.4–22.4) [primary endpoint] [8, 26]. A clinical cure was seen in 68.2% of gepotidacin recipients and 63.6% of nitrofurantoin recipients (treatment difference 4.3; 95% CI − 3.4 to 12.0) and a microbiological response was seen in 72.9% and 57.5% of patients in the respective treatment groups (treatment difference 15.5; 95% CI 7.9–23.1) [8].
In pooled data from EAGLE 2 and EAGLE 3, the composite response rates by baseline uropathogen in gepotidacin and nitrofurantoin recipients (microITTS population) were 55.1% (312/566) and 45.0% (234/520) in those infected with E.coli; 42.9% (6/14) and 37.5% (6/16) in those infected with K. pneumoniae; 60.0% (9/15) and 78.6% (11/14) in those infected with S. saprophyticus; 57.1% (8/14) and 28.6% (2/7) in those infected with E. faecalis; and 66.7% (8/12) and 40.0% (2/5) in those infected with C. freundii complex [8]. Results in patient subgroups at risk of having resistant uropathogens were generally consistent with those in the overall population in both EAGLE-2 and EAGLE-3 [26].
In EAGLE-2 and EAGLE-3 [8, 26], eligible patients weighed ≥ 40 kg, had ≥ 2 symptoms consistent with uUTI (dysuria, frequency, urgency, or lower abdominal pain) with onset within 96 h of trial entry, evidence of urinary nitrite and/or pyuria and had nitrofurantoin-susceptible qualifying uropathogens at baseline [≥ 105 colony forming units (CFU)/mL). Patients received 5 days’ treatment with oral gepotidacin 1500 mg or oral nitrofurantoin 100 mg twice daily. Therapeutic efficacy was defined as a composite of clinical cure (complete resolution of acute cystitis signs symptoms and no new symptoms) and microbiological success (reduction of baseline qualifying uropathogens from ≥ 105 to < 103 CFU/mL) at TOC without other systemic antimicrobial use. 1531 patients were enrolled in EAGLE-2 (767 in the gepotidacin group and 764 in the nitrofurantoin group) and 1605 in EAGLE-3 (805 in the gepotidacin group and 800 in the nitrofurantoin group). After a prespecified interim analysis of efficacy and safety, enrollment was stopped early because of efficacy following a recommendation of the Independent Data Monitoring Committee. Consequently, the primary analysis population included only patients who, at the time of the interim analysis data cutoff, had reached the test-of-cure visit or had not attained therapeutic success before the test-of-cure visit [8, 26].
Key clinical trials of gepotidacin (GSK)
Drug(s)
Indication
Phase
Status
Location(s)
Identifier
Gepotidacin
uUTI
3
Completed
USA
NCT06597344
Gepotidacin, nitrofurantoin, placebo
uUTI
3
Completed
Japan
NCT05630833; EAGLE-J
Gepotidacin, nitrofurantoin, placebo
uUTI
3
Completed
Global
NCT04187144; EAGLE-3;
EudraCT 2020-000553-27
Gepotidacin, nitrofurantoin, placebo
uUTI
3
Completed
Global
NCT04020341; EAGLE-2;
EudraCT 2018-001801-98
Gepotidacin
uUTI
2
Completed
USA
NCT03568942
Gepotidacin, ceftriaxone, azithromycin
uUGC
3
Completed
Global
NCT04010539; EAGLE-1;
EudraCT 2018-001780-23
Gepotidacin
uUGC
2
Completed
USA, Puerto Rico, UK
NCT02294682;
EudraCT 2015-005120-26
uUGC uncomplicated urogenital gonorrhoea, uUTI uncomplicated urinary tract infection
In a single-centre phase 2a trial (NCT03568942) in female inpatients with uUTI and a qualifying baseline uropathogen (growth; ≥ 105 CFU/mL), 5 days’ treatment with orally administered gepotidacin 1500 mg twice daily resulted in a therapeutic [combined clinical and microbiological (no growth; < 103 CFU/mL)] successful response in 6 (75%) and 5 (63%) of 8 participants at the test-of-cure (days 10–13) and follow-up (day 28 ± 3) visits [27].
2.3.2 Uncomplicated Urogenital Gonorrhoea
Gepotidacin was an effective treatment for uUGC in a phase 3 trial (NCT04010539; EAGLE-1) in male and female patients aged ≥ 12 years [28]. In the microITT population, culture-confirmed eradication of urogenital N. gonorrhoeae (microbiological success) rates at the TOC visit (3–7 days post-treatment) [primary endpoint] in gepotidacin recipients (n = 202) were non-inferior to those with ceftriaxone plus azithromycin (n = 204) [92.6% vs 91.2%; adjusted difference − 0.1%; 95% CI − 5.6 to 5.5%]. In the microbiologically evaluable (ME) population, microbiological success was 100% in both the gepotidacin (n = 187) and ceftriaxone plus azithromycin (n = 186) arms at the TOC visit. No bacterial persistence for urogenital N. gonorrhoeae was detected in either treatment group at the TOC visit in the microITT and ME populations [28] Gepotidacin recipients received two 3000 mg oral doses (second dose 10–12 h after the first dose) and ceftriaxone plus azithromycin recipients received a single intramuscular 500 mg dose of ceftriaxone plus a single oral 1 g dose of azithromycin. The microITT population consisted of patients who received at least one dose of their study treatment and had confirmed ceftriaxone-susceptible N. gonorrhoeae isolated at baseline. The ME population consisted of those in the microITT population who received all planned allocated treatment doses, had a urogenital specimen collected at the TOC visit with available culture results, had not taken any systemic antibacterial other than those included in the study before the TOC visit, and had no major protocol deviation that prevented evaluation of efficacy. Noninferiority was achieved if the lower limit of the two-sided 95% CI was > − 10% [28].
In a phase 2 dose-ranging trial (NCT02294682) in 69 adult patients with microbiologically confirmed uUGC [29], microbiological eradication of N. gonorrhoeae was achieved by 97% of those receiving a single dose of gepotidacin 1500 mg (n = 30), 95% of those receiving a single dose of gepotidacin 3000 mg (n = 39), and 96% of those in the overall population (n = 69) at the test-of-cure visit (4–8 days post-treatment). Microbiological cure was achieved in 66/69 (96%) of urogenital infections; N. gonorrhoeae isolates from the three microbiological failures had baseline gepotidacin MICs of 1 μg/mL, were quinolone resistant and had a pre-existing D86 substitution in the parC gene [29].
2.4 Adverse Events
The most common adverse reactions (incidence ≥ 1% of gepotidacin recipients) reported with gepotidacin (n = 1570) or nitrofurantoin (n = 1558) in pooled data from the EAGLE-2 and EAGLE-3 trials in in female adult and pediatric patients aged ≥ 12 years with uUTI (median treatment duration 5 days) [8] were diarrhoea (16% vs 3%), nausea (9% vs 4%), abdominal pain (4% vs 2%), flatulence 3% vs < 1%), headache (2% vs 3%), soft faeces (2% vs < 1%), dizziness (2% vs 1%), vomiting (2% vs < 1%) and vulvovaginal candidiasis (1% vs 1%). Adverse reactions associated with acetylcholinesterase inhibition in gepotidacin recipients were infrequent, as was CDI (incidence < 1% of patients) [8]. Adverse reactions leading to treatment discontinuation in EAGLE-2 and EAGLE-3 occurred in 5% (79/1570) of gepotidacin recipients and 2% (30/1558) of nitrofurantoin recipients. Serious adverse reactions occurred in 1/1570 gepotidacin recipients (dysarthria) and 1/1558 nitrofurantoin recipients. No deaths due to adverse reactions occurred in either treatment group [8]. The adverse events profile of gepotidacin in the EAGLE-1 trial in patients with uUGC was consistent with that reported in EAGLE-2 and EAGLE-3. The most frequently occurring adverse events in EAGLE-1 were gastrointestinal and those potentially related to AChEi; no drug-related serious adverse events occurred [28].







Comments (0)