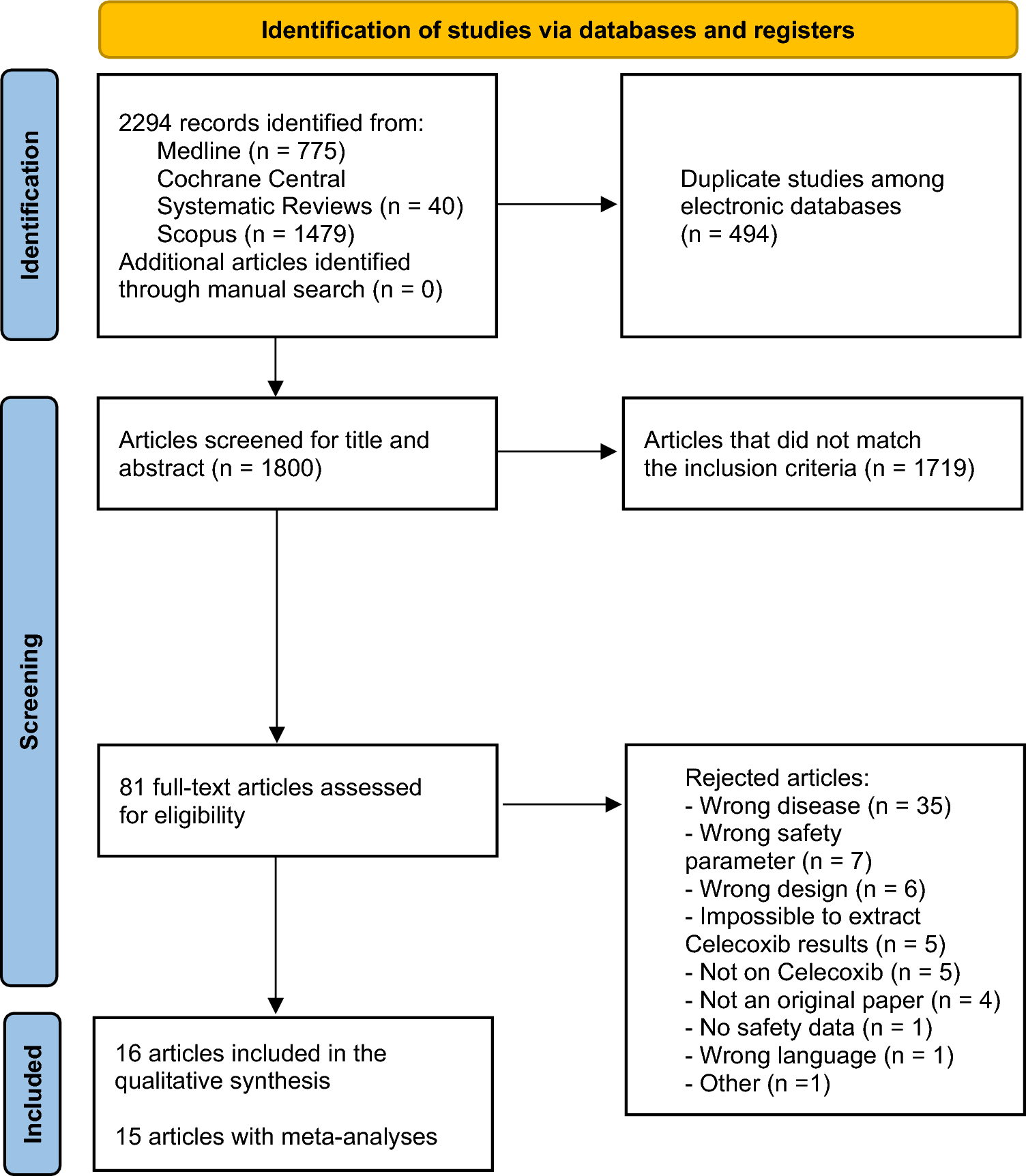
A total of 16 systematic reviews, all based on RCTs, were included in this umbrella review after a comprehensive search and selection process. Most studies focused on patients with OA or RA and assessed both the efficacy and the safety of celecoxib, primarily compared with placebo or traditional NSAIDs. Although cardiovascular safety outcomes were generally neutral, one high-quality meta-analysis reported a reduced risk of cardiovascular mortality with celecoxib compared with non-selective NSAIDs. Regarding gastrointestinal safety, celecoxib was consistently associated with a lower risk of gastroduodenal ulcers than were non-selective NSAIDs, although findings were more heterogeneous for other gastrointestinal outcomes. Notably, although based on a limited number of low-quality meta-analyses, celecoxib appeared to be associated with a lower risk of renal adverse events and reduced all-cause mortality than non-selective NSAIDs, suggesting a potentially more favorable overall safety profile that warrants further investigation. Overall, despite the predominance of critically low-quality reviews, some consistent trends suggest a favorable gastrointestinal profile for celecoxib and potentially reduced all-cause or cardiovascular mortality compared with traditional NSAIDs.
Our findings are largely consistent with the existing body of literature concerning the safety profile of celecoxib [31, 32]. The observed reduction in the incidence of gastroduodenal ulcers compared with traditional non-selective NSAIDs aligns with previous individual studies and some clinical guidelines, which have recognized the more favorable gastrointestinal safety profile of celecoxib [33,34,35]. Several pharmacological studies have attributed this effect to the selective inhibition of COX-2 by celecoxib, thereby sparing COX-1-mediated gastroprotective prostaglandin synthesis [36]. In contrast, the evidence regarding cardiovascular safety remains less definitive. Earlier concerns were raised after the withdrawal of rofecoxib, another selective COX-2 inhibitor, because of an increased cardiovascular risk [37]. Subsequent investigations have sought to determine whether celecoxib carries a similar risk profile [38]. Notably, the PRECISION trial, a large, pragmatic RCT, demonstrated non-inferiority of celecoxib compared with naproxen and ibuprofen with respect to cardiovascular outcomes in patients with OA or RA at moderate cardiovascular risk [39]. In addition to cardiovascular safety, PRECISION provided valuable insights into other organ-specific outcomes. A prespecified secondary analysis focusing on major NSAID toxicity, including cardiovascular, gastrointestinal, and renal events and all-cause mortality, showed that celecoxib was associated with a significantly lower incidence of composite major toxicity than both ibuprofen and naproxen [40]. Specifically, the numbers needed to harm were 82 for ibuprofen and 135 for naproxen compared with celecoxib, highlighting a more favorable overall safety profile of celecoxib. In terms of gastrointestinal safety, a dedicated sub-analysis of PRECISION confirmed a significantly lower incidence of clinically significant gastrointestinal events and iron deficiency anemia with celecoxib [41]. Celecoxib also maintained its advantage when used in combination with low-dose acetylsalicylic acid (aspirin) or corticosteroids, suggesting a robust gastrointestinal safety profile across different risk profiles. In addition, the PRECISION ABPM sub-study, which evaluated the impact of these NSAIDs on ambulatory blood pressure, showed a significantly lower increase in 24-h systolic blood pressure with celecoxib than with ibuprofen [42]. The incidence of new-onset hypertension was also significantly lower with celecoxib, which may contribute to its superior cardiovascular tolerability. Finally, renal outcomes, a growing concern with chronic NSAID use, were also evaluated in a recent secondary analysis of the PRECISION trial [43]. Celecoxib was associated with a lower incidence of renal events, including acute kidney injury and hospitalization for heart failure or hypertension, than were ibuprofen and naproxen. These findings were consistent in both intention-to-treat and on-treatment analyses, reinforcing the favorable cardiorenal safety profile of celecoxib. Taken together, the data from the PRECISION program suggest that celecoxib is not only as safe as non-selective NSAIDs but may be safer, particularly when gastrointestinal, blood pressure, and renal outcomes are considered in addition to cardiovascular risk. Furthermore, the distinct methodology of the PRECISION trial compared with most other RCTs included in our review is important to emphasize. As a large-scale, long-term RCT with a mean treatment duration of approximately 20 months, PRECISION incorporated independently adjudicated outcomes and was conducted independently of industry influence. This distinguishes PRECISION from other trials, which often involve shorter treatment durations and less rigorous, more heterogeneous endpoint evaluation processes. When interpreting comparative safety findings between celecoxib and non-selective NSAIDs, this distinction in trial quality should be acknowledged.
It must be noted that many of the systematic reviews included in our umbrella review excluded observational studies, which could have provided interesting complementary information, particularly regarding long-term and rare adverse events. For example, the population-based observational study by McGettigan and Henry [44] provided robust comparative data on the cardiovascular risks associated with different NSAIDs in real-world settings. Their findings showed that, although celecoxib was associated with a modest increase in cardiovascular risk (RR 1.17 [95% CI 1.08–1.27]), this risk remained lower than that observed with diclofenac or rofecoxib, and was comparable to that of ibuprofen, particularly at typical doses. Such studies offer valuable insights that complement randomized evidence, particularly with regard to populations not commonly included in clinical trials. In fact, large-scale observational studies and real-world evidence have generally supported that celecoxib, when used at recommended doses, does not increase the cardiovascular risk compared with traditional NSAIDs [38]. Consequently, the reliance on RCT-derived data only, as observed in most of the included reviews, may limit the generalizability of findings to patients seen in routine clinical practice. Taken together, the current literature suggests that, although celecoxib offers distinct gastrointestinal safety advantages over non-selective NSAIDs, emerging evidence—albeit limited and of low quality—also indicates a potentially more favorable renal and all-cause mortality profile. Cardiovascular safety appears generally comparable to that of non-selective NSAIDs, but further high-quality studies are needed. These findings highlight the importance of considering both the available evidence and individual patient risk factors when selecting anti-inflammatory treatment.
Recent studies have further emphasized the importance of patient context when evaluating the safety of celecoxib. Antonioli et al. [45] reported an increased risk of postoperative heart failure among patients with type 2 diabetes mellitus undergoing total knee arthroplasty when celecoxib was used perioperatively, compared with meloxicam. Although the study was observational in nature, these findings suggest that celecoxib may not be the optimal choice in certain high-risk settings. Similarly, Kim et al. [46] found no significant cardiovascular or gastrointestinal safety advantage for celecoxib over non-selective NSAIDs in patients with AS, a younger group at lower risk, potentially indicating that safety benefits are more apparent in older, comorbid populations. Taken together, these results emphasize that NSAID safety profiles are highly dependent on context, and there remain patient groups for whom the use of NSAIDs or COX-2 inhibitors is either inappropriate or poorly characterized in the literature.
This umbrella review has several important strengths. It followed a registered protocol and adhered to established methodological standards (PRISMA 2020, Joanna Briggs Institute guidelines), ensuring transparency and rigor. A comprehensive search strategy across multiple databases and additional manual searches minimized the risk of missing relevant studies. The methodological quality of the reviews included was critically appraised using the AMSTAR-2 tool, providing important information for interpretation of the level of evidence. Finally, the focus on clinically meaningful outcomes based on RCT data enhances the internal validity of the findings, despite recognized limitations in generalizability.
Several limitations should be acknowledged. Most of the included systematic reviews did not provide detailed information on participant demographics or comorbidities, limiting our ability to draw conclusions for subpopulations such as older adults or those with prior cardiovascular or renal conditions. Earlier RCTs typically included relatively homogeneous and healthier adult populations, often excluding patients at higher risk for adverse events. However, the PRECISION trial included individuals with established cardiovascular disease or elevated cardiovascular risk, improving the generalizability to more complex real-world populations. This distinction highlights the need for more granular safety data across age groups and comorbidity profiles, particularly in older adults who represent a large proportion of those treated for chronic musculoskeletal conditions. Another important limitation is that most included systematic reviews were of critically low methodological quality, reducing confidence in the overall findings. Substantial heterogeneity across studies regarding populations, interventions, and outcome definitions complicates interpretation. The exclusive reliance on randomized trial data, often limited by short follow-up periods, may underestimate long-term or rare adverse events. The limited inclusion of observational studies further restricts the assessment of real-world safety. In addition, potential publication bias, particularly from industry-sponsored trials, cannot be entirely ruled out. Also, an important potential limitation of this review is the use of the AMSTAR-2 checklist to assess the methodological rigor of the included reviews. Although AMSTAR-2 is a widely accepted tool for assessing risk of bias, it does not really provide an overall “quality score” and instead focuses on the presence or absence of critical and non-critical methodological areas. As a result, reviews may be rated as “critically low” because of the absence of items that are not necessarily central to the reliability of their findings (e.g., lack of protocol registration or funding source reporting). This severe downgrading may limit the overall value of some reviews, especially if core methodological components such as study selection, data extraction, and risk-of-bias assessment have been adequately addressed. Therefore, AMSTAR-2 ratings should be interpreted as indicators of potential bias rather than as absolute judgments of quality. Finally, another important limitation of this umbrella review is the deliberate restriction of the target population to patients with OA, RA, or AS. As a result, the findings should be interpreted strictly within the context of these specific conditions and cannot be generalized to other musculoskeletal disorders. Several potentially relevant systematic reviews were excluded because they included mixed populations (e.g., patients with OA or RA alongside those with low back pain or other non-inflammatory conditions) without reporting separate outcomes for the populations of interest. In such cases, our inability to extract stratified data limited their inclusion and may have led to the omission of useful evidence related to OA, RA, or AS.
The results of this umbrella review suggest that celecoxib may be a preferable therapeutic option for patients at increased gastrointestinal risk who require long-term NSAID therapy, as it has a lower incidence of gastroduodenal ulcers than traditional non-selective NSAIDs. Nevertheless, clinical decision-making should be individualized and take into account each patient's comorbidities, risk factors, and treatment goals, particularly in high-risk populations. Future research should prioritize the integration of high-quality randomized and observational data to better assess the long-term safety of celecoxib, especially with regard to rare cardiovascular and renal events. Systematic reviews using methods capable of synthesizing evidence from different study designs are warranted to provide a more comprehensive and applicable assessment of the benefit–risk profile of celecoxib in routine clinical practice.







Comments (0)