
Remember me






The eligibility criteria for participants in ONWARDS 1–5 were broad and designed to closely mimic real-world clinical practice, reflecting the criteria used for daily basal insulins (e.g., degludec, glargine U100, and glargine U300) [6,7,8,9,10,11]. As a result, the eligibility criteria for icodec in clinical practice are similarly broad, covering insulin-naïve individuals and those transitioning from daily basal insulin [18].
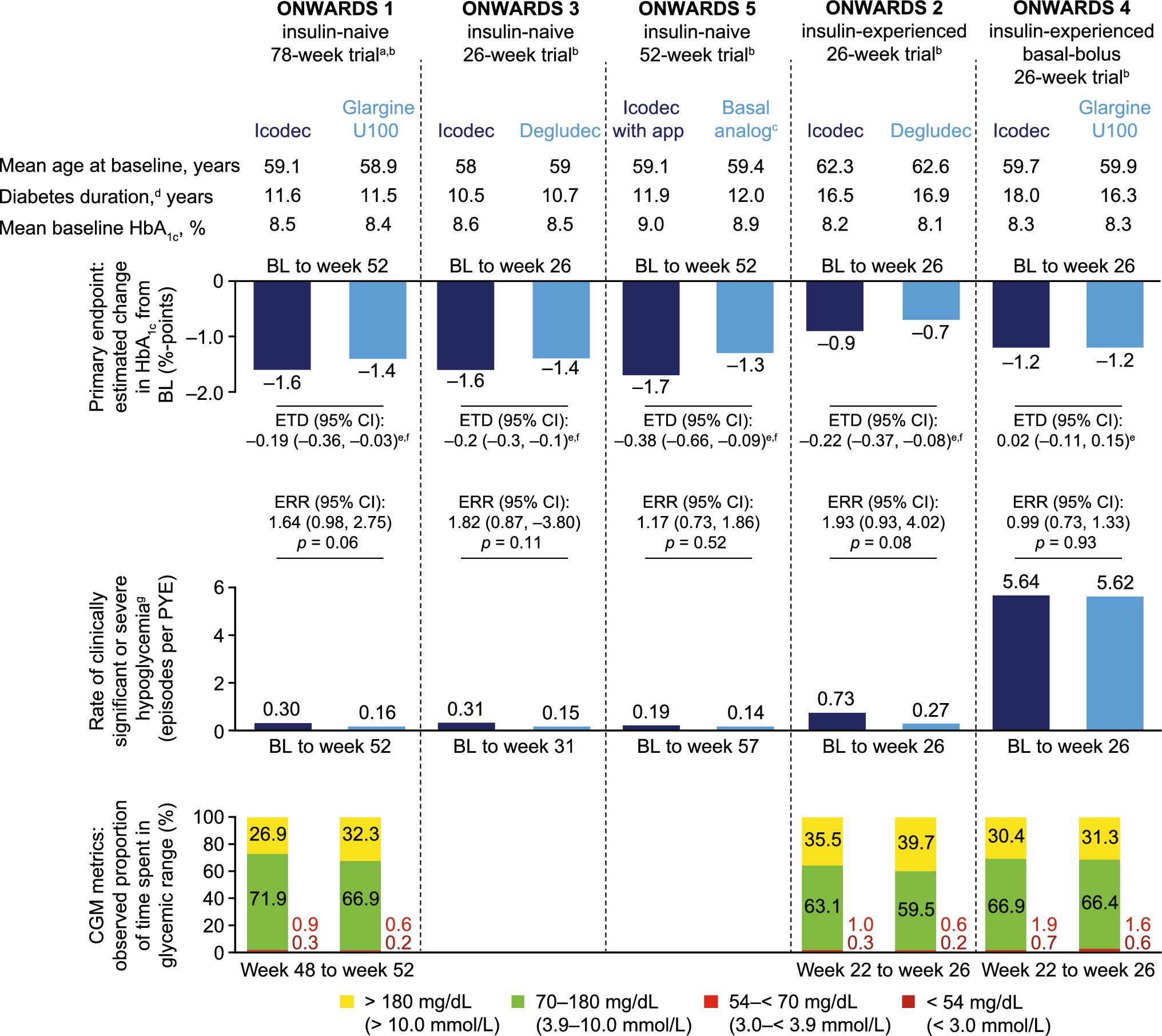
ONWARDS 1–5 included insulin-naïve (ONWARDS 1, 3, 5) or insulin-experienced (ONWARDS 2, 4) adults (≥ 18 years of age) with T2D (HbA1c 7.0–10.0% [ONWARDS 2, 4], 7.0–11.0% [ONWARDS 1, 3], or > 7.0% [ONWARDS 5]) and a body mass index (BMI) of 40.0 kg/m2 or less (ONWARDS 1–4; no BMI restrictions in ONWARDS 5) [6,7,8,9,10,11].
Individuals who had hypersensitivity to trial products, cardiovascular events in the 180 days before screening, chronic heart failure, or severe renal impairment were excluded from the trials, except ONWARDS 5, in which severe renal impairment was permitted. In ONWARDS 2 and 4, individuals who had hypoglycemia unawareness, recurrent severe hypoglycemia episodes, and/or uncontrolled blood pressure were also excluded [6,7,8,9,10,11]. In clinical practice, caution should be exercised for similar individuals, particularly those with a history of severe hypoglycemia or hypoglycemia unawareness [expert opinion].
Although most adults with T2D would be eligible for icodec, practical considerations such as cost, coverage, and access may affect icodec initiation in real-world practice [expert opinion].
3.1.2 Initiation of Icodec Treatment in Insulin-Naïve Individuals with T2DIn ONWARDS 1, 3, and 5 (insulin-naïve individuals with T2D), icodec was initiated at 70 U/week (equivalent to 10 U of daily basal insulin), maintaining the same injection volume as a 100 U/mL daily basal insulin owing to its seven-times concentration (700 U/mL) [6, 8, 10]. The recommended starting dosage of icodec in clinical practice is 70 U/week, followed by individual once-weekly dose adjustments [18]. However, according to expert opinion, as is common practice with OD basal insulin, icodec may be started at a different dose depending on the individual and the clinical situation (Fig. 2; Step 1). For certain individuals with T2D, such as those who also have chronic kidney disease with a reduced glomerular filtration rate or low BMI, a lower starting dosage (e.g., 50 U/week) may be appropriate [expert opinion], similar to what is commonly given when initiating daily basal insulin in such individuals (e.g., initiating at 6 U/day instead of 10 U/day).
Fig. 2
Treatment algorithm used for individuals with type 2 diabetes (T2D) in ONWARDS 1–5. Weekly dose adjustment is based on three prebreakfast SMBG values, measured 2 days prior to and on the day of titration. If any of the three prebreakfast SMBG values are below the lower limit of the target range, titration is based on the lowest recorded value. If all three SMBG values are above the lower limit of the target range, titration is based on the mean of the three measurements. aWhen switching individuals from OD or twice-daily basal insulin, the recommended once-weekly icodec dose is the total daily basal dose multiplied by seven. When switching individuals from OD or twice-daily basal insulin, for the first injection only (week 1 dose), a 50% one-time additional icodec dose is recommended (for the first injection only) if seeking faster achievement of glycemic control in individuals with type 2 diabetes; however, this one-time additional dose is not mandatory. If the 50% one-time additional icodec dose is administered, the week 1 dose should be the total daily basal insulin dose multiplied by seven and then multiplied by one and a half, rounded to the nearest 10 U. The 50% one-time additional dose must not be added for the second injection. bExpert opinions regarding the initiation and titration of icodec. cFor individuals with T2D and low body mass index or chronic kidney disease, a lower starting dose (e.g., 50 U/week) may be appropriate, while higher doses may suit those with high insulin resistance or HbA1c [expert opinion]. For Asian individuals, 30–70 U/week may be considered, per local labels in China (70 U/week) and Japan (30–70 U/week). dClinicians may decide to titrate less aggressively for individuals who are at greater risk of hypoglycemia, such as those with preserved insulin sensitivity, hepatic or renal impairment, or elderly individuals [expert opinion]. The prefilled insulin pen injector used to administer icodec can be dosed either up or down by a minimum of 10 U, so clinicians may also consider fine tuning in increments or decrements of 10 U for dose optimization or in special situations once a stable dose has been established [expert opinion]. In some situations, such as during prolonged hospital admission and pregnancy, it may be preferable to switch from icodec to daily insulin. Icodec insulin icodec, OD once-daily, SMBG self-measured blood glucose, U units.
For Asian individuals, a starting dosage ranging 30–70 U/week could be considered [expert opinion]. According to the approved labels, the recommended weekly starting dosage in China is 70 U, with individual adjustments based on the individual’s condition; in Japan, treatment may be initiated with 30–70 U, adjusted according to the individual’s condition [19, 20] (corresponding to approximately 4–10 U/day) [20].
Occasionally, as is true in clinical practice for other insulins, higher starting doses of icodec might be preferred, particularly among individuals with high levels of insulin resistance or a high HbA1c [expert opinion]. However, icodec may not be the most suitable option when rapid glycemic control is required [expert opinion].
3.1.3 Switching from Daily Basal Insulin to Icodec in Insulin-Experienced Individuals with T2DIn ONWARDS 2 and 4, to prevent a potential transient increase in fasting plasma glucose levels that may occur until steady state of icodec is achieved, the weekly icodec dose, calculated as the pretrial total daily dose multiplied by seven, was increased by 50% for the first injection only. From week 2 (second injection), participants received the calculated once-weekly icodec dose [7, 9].
In an open-label, phase I trial (NCT04582435) of 46 adults (≥ 18 years) with T2D, a pharmacokinetic modeling analysis demonstrated that clinical steady state was reached 2–4 weeks after subcutaneous injection when initiating icodec without a one-time additional dose, and 2–3 weeks after subcutaneous injection when initiating icodec with a 50% one-time additional dose [16]. Additionally, in a phase II trial (NCT03922750), switching from daily insulin to icodec with a 100% one-time additional dose reduced the transient increase of fasting plasma glucose and TAR in the first 4 weeks following the initial icodec injection when compared with icodec administered without an additional dose [21]. A pharmacokinetic/pharmacodynamic modeling analysis using data from ONWARDS 2 and 4 investigated efficacy outcomes and hypoglycemia rates when switching from daily basal insulin to icodec with or without a 50% one-time additional dose. The model predicted a mild, transient (1–2 weeks) increase in prebreakfast self-measured blood glucose (SMBG) after initiation without sustained differences in HbA1c, clinically significant hypoglycemia, or weekly insulin dose at week 26, suggesting no sustained difference from omitting the 50% one-time additional dose [22]. A clinical trial is ongoing currently exploring the switch from daily basal insulin to icodec without a one-time additional dose (NCT0634085; results have not yet been posted at the time of writing), thus providing further evidence to support tailoring of clinician decisions to suit the needs of individuals.
Therefore, in clinical practice, if seeking faster achievement of glycemic control when switching to icodec, the first (week 1) icodec dose should be the total daily basal insulin dose multiplied by seven and then by one and a half (i.e. the 50% one-time additional dose) (Fig. 2; Step 1); for practical purposes, this can also be calculated by multiplying the daily basal insulin dose by 10.5, rounded to the nearest 10 U [18]. Based on the clinician’s judgment, the 50% one-time additional dose may be omitted, including if the individual tends to miss daily basal insulin injections because this may lead to an overestimation of the actual insulin need [expert opinion]. From the second week onwards, the calculated weekly basal insulin dose will be reduced to the daily basal insulin dose multiplied by seven [18]. Care should be given to avoid dosing errors, such as overdosing or forgetting to remove the one-time additional dose after the first injection, which could lead to hypoglycemia. Subsequent insulin titration (see Sect. 3.2) requires a minimum of three prebreakfast SMBG measurements per week, from week 2 if not using a one-time additional dose, and from week 3 if using a one-time additional dose (Fig. 2; Step 1). Individuals should be instructed to consult their physician if they are uncertain about the correct dose.
3.2 Icodec Dose Titration in Insulin-Naïve and Insulin-Experienced Individuals with T2DThe titration strategy used in the phase IIIa ONWARD 1–5 trials is summarized in Fig. 2; Step 2. In insulin-naïve individuals with T2D, the titration was ± 20 U weekly (or no change) if prebreakfast SMBG was above or below the target range of 80–130 mg/dL [4.4–7.2 mmol/L] on the 2 days prior to and on the day of the next injection.
Clinicians may decide to titrate less aggressively for individuals who are at greater risk of hypoglycemia, such as those with preserved insulin sensitivity, or hepatic or renal impairment, or elderly individuals (aged ≥ 65 years) [expert opinion]. The prefilled insulin pen injector used to administer icodec can be dialed either up or down by a minimum of 10 U, so clinicians may also consider fine-tuning in increments or decrements of 10 U for dose optimization or in special situations once a stable dose has been established [expert opinion].
With the advancement of digital health technologies, insulin titration tools are being explored to potentially support healthcare professionals and individuals with diabetes [23]. In ONWARDS 5, icodec titration was guided by an app providing weekly dose recommendations based on SMBG levels [10]. A post hoc analysis investigated clinical outcomes for icodec according to adherence to the app guidance, and categorized participants into three adherence subgroups: low (≤ 1 week adherent per 4 weeks), medium (> 1 to ≤ 3 weeks), and high (> 3 weeks) [24, 25]. Modeling analyses assessed associations between app adherence, estimated prebreakfast SMBG, and weekly insulin dose. In the modeling analyses, higher adherence was linked to statistically significantly lower SMBG levels compared with low adherence, and there were trends toward higher weekly insulin doses in high- versus low-adherence subgroups [24, 25]. The observed rate of clinically significant hypoglycemia was lower in the high- versus low-adherence subgroups [24, 25]. The results of this study support the use of app-based titration strategies for icodec in real-world clinical practice, where available.
3.3 Factors to Consider when Administering Icodec and its Use in Special Populations3.3.1 Ethnicity and RaceA post hoc analysis of ONWARDS 1–5 assessed the effects of ethnicity (Hispanic/Latino and nonHispanic/Latino) and race (Asian, Black/African American, White, and 'Other' (American Indian or Alaska native, and native Hawaiian or other Pacific islander)) on the efficacy and hypoglycemia outcomes of icodec versus OD comparators [26].
Overall, efficacy and hypoglycemia outcomes were consistent for icodec versus OD comparators across ethnicity and race subgroups. The estimated change in HbA1c from baseline to EOT generally favored icodec, with no statistically significant treatment by subgroup interactions. Rates of combined clinically significant or severe hypoglycemia were also consistent among these subgroups [26].
Based on these data, no blanket dose adjustments would be required for icodec based solely on ethnicity or race; however, specific considerations, such as the potential for lower starting doses in some Asian individuals, as discussed is Sect. 3.1.2, may still apply [18].
3.3.2 Age: Elderly IndividualsMost people with T2D are elderly adults (≥ 65 years), which can make diabetes management challenging owing to comorbidities and potential cognitive decline. As the global population ages, the prevalence of T2D among elderly adults is expected to rise, further emphasizing the need for individualized treatments across age groups [27,28,29].
A post hoc analysis of ONWARDS 1–5 demonstrated that the efficacy and hypoglycemia outcomes were consistent for icodec versus OD comparators across all age groups (< 55, 55–64, and ≥ 65 years) [26]. The estimated change in HbA1c from baseline to EOT was generally higher for icodec than OD comparators, with no statistically significant treatment by subgroup interactions. Rates of combined clinically significant or severe hypoglycemia were low and consistent across age groups [26]. Based on these data, no blanket dose adjustments are required for icodec with older users [18], and no excess risk of hypoglycemia is expected with icodec in older users.
Icodec may be particularly appropriate for those with frailty who have high perceived pill burden or do not tolerate non-insulin glucose-lowering medications, those who are recommended relaxed glycemic targets that are not being achieved with their current non-insulin antihyperglycemic regimen, those who have difficulty remembering daily injections, people in nursing homes, or those who are dependent on caregivers/family members for insulin administration [expert opinion].
3.3.3 Pediatric PopulationsPreliminary data from a phase 1 trial (NCT05790681) of icodec use in an insulin-experienced pediatric population (< 18 years) with T2D demonstrated that icodec was well tolerated, with a pharmacokinetic profile that was similar to that in adults with T2D [30]. Further trial data are expected to become available in the future.
3.3.4 Hepatic ImpairmentHepatic impairment can affect insulin clearance and glucose regulation, potentially necessitating adjustments in insulin dosing to avoid hypoglycemia or suboptimal glycemic control [31, 32]. A phase I trial (NCT04597697) found no clinically relevant differences in icodec pharmacokinetics after a single 1.5 U/kg dose in adults with normal or impaired hepatic function [33]. Owing to the relatively few numbers of individuals with hepatic impairment included in the ONWARDS trials, there are no additional efficacy and safety data for icodec in these individuals. Based on the available data, no specific icodec dose adjustments are required in individuals with hepatic impairment. However, the increased icodec exposure due to reduced clearance in individuals with mild and moderate hepatic impairment suggests more frequent glycemic monitoring may be needed, as recommended for daily insulin preparations [18, 33].
3.3.5 Renal ImpairmentReduced kidney function can decrease insulin elimination, thereby prolonging insulin activity and potentially increasing the risk of hypoglycemia [34].
In a phase I trial (NCT03723785), icodec exposure was slightly higher in adults with renal impairment or end-stage renal disease (ESRD) than in those with normal renal function after a single subcutaneous icodec dose (1.5 U/kg) [33]. Furthermore, a post hoc analysis of ONWARDS 1–5 examined efficacy and hypoglycemia outcomes by renal function category (excluding ESRD and severe renal impairment (in ONWARDS 1–4)], per trial eligibility criteria). Outcomes with icodec versus OD comparators were generally consistent regardless of kidney function, with no statistically significant treatment interactions by kidney function subgroup for HbA1c change, and no consistent trend by kidney function subgroup for overall rates of combined clinically significant or severe hypoglycemia or weekly basal insulin dose during the last 2 weeks of treatment [35].
Based on these data, no specific dose adjustments are required among individuals with renal impairment because icodec should be dosed according to individual needs. However, the increased icodec exposure associated with reduced insulin clearance in individuals with, versus without, renal impairment [33] suggests that more frequent glycemic monitoring may be required, as with other insulin preparations [expert opinion].
3.3.6 HypoalbuminemiaAt steady state, in individuals with a normal serum albumin level (approximately 4.0 mg/dL [0.6 mmol/L]), the maximum serum concentration of icodec is lower than that of albumin. The ratio of albumin to icodec is approximately 2000:1 meaning that icodec occupies < 0.05% of all available albumin molecules in circulation. Additionally, each albumin molecule has at least four high-affinity binding sites for icodec, resulting in an excess of binding capacity even at relatively high concentration of icodec [14]. Consequently, displacement of icodec from albumin due to reduced levels of albumin (e.g., from hypoalbuminemia) or the presence of other medications such as GLP-1 RAs that bind to albumin is likely minimal, with no clinically relevant effect on icodec activity [14]. In vitro data show no clinically relevant displacement of icodec by fatty acids or anionic protein-bound medicinal products [18].
Across the ONWARDS 1–5 trials, only three participants of the 1,881 who received icodec reported hypoalbuminemia [35]. These individuals experienced HbA1c reductions from baseline to planned EOT ranging from − 1.1% points to − 2.1% points, with one participant reporting two episodes of clinically significant hypoglycemia. Current data does not show any correlation between serum albumin levels and icodec exposure, suggesting that increased icodec exposure due to hypoalbuminemia is unlikely [35].
3.3.7 PregnancyTreatment guidelines stipulate that insulin should be administered alongside medical nutrition therapy to control pre-existing T2D among pregnant individuals [36]. Although animal reproduction studies with icodec have not revealed any effects regarding embryotoxicity and teratogenicity, there are no clinical data regarding the use of icodec during pregnancy available, and there are no registered clinical trials (ClinicalTrials.gov, accessed 14 January 2025). Therefore, women of childbearing potential should be advised to discontinue icodec if they become pregnant or wish to become pregnant [18], and, if indicated, switch to another insulin regimen approved for use during pregnancy [expert opinion].
3.3.8 Coadministration of Icodec with GLP-1 RAs and SGLT2isA post hoc analysis of ONWARDS 1–5 showed that icodec had consistent efficacy and hypoglycemia outcomes versus OD comparators among adults with T2D regardless of baseline GLP-1 RA or SGLT2i use [37] (Fig. S1 and S2, OSM). Overall, across GLP-1 RA and SGLT2i subgroups, there were no statistically significant treatment by subgroup interactions with respect to change in HbA1c from baseline to EOT, change in body weight from baseline to EOT (except for SGLT2i use in ONWARDS 5), mean weekly basal insulin dose during the last two weeks of treatment (except for SGLT2i use in ONWARDS 5), and the proportions of participants who achieved an HbA1c < 7% without combined clinically significant or severe hypoglycemia. Irrespective of baseline GLP-1 RA and SGLT2i use, the rates of combined clinically significant or severe hypoglycemia were low (less than one episode per PYE) across the treatment arms of ONWARDS 1, 2, 3, and 5. The weekly basal insulin dose during the last two weeks of treatment was similar or higher with icodec than OD comparators, irrespective of baseline GLP-1 RA and SGLT2i use, but the treatment difference was generally equivalent to approximately 1–3 U/day, corresponding to typical daily basal insulin adjustments in clinical practice [38].
Based on these post hoc data, the efficacy and hypoglycemia profile of icodec appeared generally consistent regardless of concomitant GLP-1 RA or SGLT2i use.
In addition to GLP-1 RAs and SGLT2is, other non-insulin glucose-lowering medications, such as sulfonylureas and glinides, may affect insulin requirements and need consideration when co-administered with basal insulin [expert opinion]. As noted in the European product label, certain medicinal products may increase (e.g., corticosteroids, oral contraceptives) or decrease (e.g., sulfonylureas, GLP-1 RAs) insulin needs [18]. Pretrial sulfonylureas and glinides were discontinued in ONWARDS 1, 2, and 4, and reduced by 50% in ONWARDS 3 and 5 (changes to other background non-insulin glucose-lowering medications in ONWARDS 5 were allowed at the investigator’s discretion) to minimize the risk of hypoglycemia. This highlights the importance of adjusting these medications when combined with insulin therapy to reduce the hypoglycemia risk while maintaining optimal glycemic control [6,7,8,9,10,11].
3.4 Treatment Monitoring and Management of Icodec Use During Practical Situations3.4.1 Hypoglycemia MonitoringGiven the risk of hypoglycemia with insulin therapy, regular glucose monitoring is imperative to improve treatment outcomes. CGM is advisable, particularly for individuals with impaired hypoglycemia awareness [39, 40].
CGM was used in insulin-naïve individuals (ONWARDS 1) and insulin-experienced individuals with T2D (ONWARDS 2 and 4) at treatment initiation/switch (from week 0 to week 4), during/at the EOT (from week 22 to week 26, and week 48 to week 52, and week 74 to week 78 for ONWARDS 1), and follow-up (from week 27 to week 31 for ONWARDS 2 and 4; week 78 to week 83 for ONWARDS 1) [6, 41].
In an exploratory analysis of ONWARDS 1, during/at the EOT, TIR was statistically significantly greater, whereas TAR was lower, with icodec than with glargine U100 [41]. TBR < 54 mg/dL (< 3.0 mmol/L) and TBR < 70 mg/dL (< 3.9 mmol/L) remained below recommended targets (< 1% and < 4%, respectively) [42, 43] across time periods and treatment arms; TBR < 54 mg/dL (< 3.0 mmol/L) was slightly higher on days 1–2 versus other days of the week after icodec injection [41]. In a post hoc analysis of ONWARDS 2 and 4, there were no statistically significant differences in TIR, TAR, or TBR < 54 mg/dL (< 3.0 mmol/L) for icodec versus OD comparators [
Comments (0)