Study design and data source
This study utilized a cross-sectional design to investigate the association between socioeconomic deprivation and polypharmacy among adults in England, using data from the Health Survey for England (HSE) 2021. The HSE is an annual survey commissioned by NHS England (formerly NHS Digital), designed to provide nationally representative data on the health and lifestyles of individuals living in private households in England [13]. The 2021 survey, conducted by the National Centre for Social Research (NatCen) and University College London (UCL), adapted its methodology due to the COVID-19 pandemic, shifting from face-to-face interviews to remote telephone and video interviews, with nurse visits resuming in October 2021 for a subset of participants [13].
The HSE 2021 employed a stratified random probability sample of households, selecting 12,798 addresses across 711 postcode sectors, comprising 9774 addresses in 543 postcode sectors for the core sample and 3,024 addresses in 168 postcode sectors for the reserve sample [13]. Fieldwork was conducted from January 2021 to June 2022, achieving a household response rate of 32%. In total, 5880 adults aged 16 and over and 1240 children aged 0 to 15 were interviewed, with 1,705 adults and 250 children completing a nurse visit. Data collection involved a Stage 1 interview (via telephone or video) and, for 89% of participating households, a Stage 2 nurse visit, which included physical measurements and biological sample collection.
Participant selection and study population
For this analysis, we focused on adults aged 16 years and older who completed the HSE 2021 nurse visit, as the nurse questionnaire included detailed questions on medication use necessary for defining polypharmacy. In 2021, not all households were eligible for the nurse visit due to adaptations in the survey methodology. In each primary sampling unit (PSU), 16 out of 18 addresses were selected at random in advance; within these households, all adults and children who were interviewed during the Stage 1 interview were eligible for the nurse visit. In the remaining two households per PSU, nurse visits were not offered. This process resulted in 1,705 adults completing the nurse visit, which is the final analytical sample. All participants were included regardless of multimorbidity status to allow for a comprehensive population-level analysis of polypharmacy. This approach enabled us to assess whether area-level socioeconomic deprivation is associated with increased medication burden independently of diagnosed chronic conditions.
VariablesOutcome: polypharmacy
Polypharmacy was defined as the concurrent use of five or more prescribed medications within the past seven days, a threshold commonly used in the literature to indicate increased risk of adverse drug interactions and healthcare burden [1,2,3]. Medication use was assessed based on participant self-report of prescribed treatments taken in the previous week, excluding contraceptives and nicotine-dependence therapies in accordance with standard practice. Responses were grouped into nine categories representing the number of medications taken, from none to eight or more. Medications covered a wide range of treatments for diverse conditions, including cardiovascular drugs (e.g. diuretics, ACE inhibitors), lipid-lowering agents, antidiabetic medications (e.g. metformin), respiratory treatments for asthma and chronic obstructive pulmonary disease (COPD), mental health medications (e.g. antidepressants, antipsychotics, and hypnotics), proton pump inhibitors (PPIs), non-steroidal anti-inflammatory drugs (NSAIDs), analgesics, and antibacterials. For analysis, a binary outcome variable was created: individuals reporting the use of five or more prescribed medications were classified as having polypharmacy (coded as 1), while those reporting fewer than five were classified as not having polypharmacy (coded as 0).
Exposure: socioeconomic deprivation
The primary exposure was socioeconomic deprivation, measured using the Index of Multiple Deprivation (IMD) 2019, a composite measure of deprivation across seven domains: income, employment, education, health, crime, barriers to housing and services, and living environment [14]. IMD scores were assigned to participants based on their residential postcode and categorized into quintiles, with Quintile 1 representing the least deprived areas and Quintile 5 the most deprived. The IMD was chosen as the exposure variable because it provides a robust, area-based measure of socioeconomic deprivation, widely used in UK health research to assess social inequalities [14].
Covariates
We adjusted for several covariates known to influence medication use and deprivation, collected during the Stage 1 interview and nurse visit. These included age (categorized as 16–44, 45–54, 55–64, and 65 + years), sex (male/female), and ethnicity (categorized as White, Non-White, and Others, based on self-reported ethnic origin, with Non-White including Black, Asian, and Mixed categories). Clinical factors included multimorbidity (defined as the presence of two or more doctor-diagnosed conditions such as hypertension, diabetes, or raised cholesterol, as reported in the nurse interview, and categorized as none, 1 condition, 2–3 conditions, or 4 + conditions) and obesity status (categorized as Obese, Not Obese, or missing, based on body mass index measurements taken during the nurse visit). Lifestyle factors comprised cigarette smoking status (current smoker, ex-regular smoker, never regular smoker) and alcohol consumption (categorized as non-drinker in the last 12 months, low-risk drinker [up to 14 units per week], higher-risk drinker [> 14 units per week], or missing, based on self-reported drinking behaviour). Healthcare access was assessed by the frequency of GP visits in the past 12 months (categorized as 0, 1 or 2, 3 to 5, or 6 or more visits), derived from general health questions asked of all participants during the Stage 1 interview. These covariates were selected based on their established associations with polypharmacy and deprivation in prior studies [15,16,17,18]. Missing and unreported values in the covariates were classified in a separate category.
Statistical analysis
Descriptive statistics were used to summarize the characteristics of the study population, stratified by polypharmacy status, and presented as unweighted frequencies and percentages. Chi-square tests were used to examine differences between categorical variables across polypharmacy status. Fisher’s exact test was applied where expected cell counts were less than 5, ensuring accurate statistical inference in small sample sizes. To estimate the association between socioeconomic deprivation and polypharmacy, we employed multivariable logistic regression, modelling polypharmacy as a binary outcome, with IMD quintiles as the primary exposure (reference: Quintile 1, least deprived). The model adjusted for age, sex, ethnicity, multimorbidity, obesity, smoking status, alcohol consumption, and GP visit frequency to control for potential confounding. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported to quantify the strength of the association.
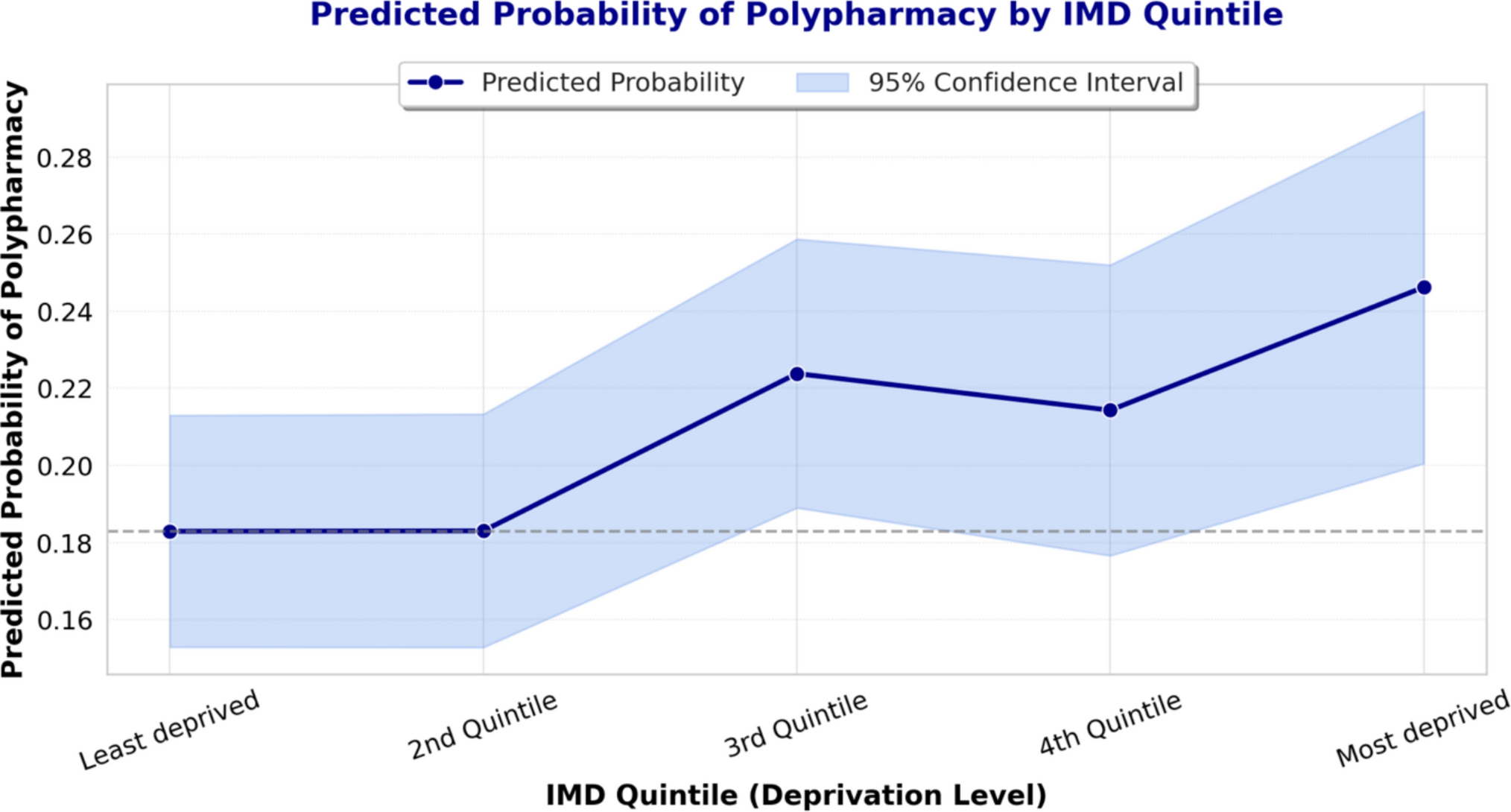
A polynomial contrast test was used to assess the trend in the association between deprivation and polypharmacy, testing for a linear relationship across deprivation quintiles. To illustrate the relationship graphically, we computed adjusted predicted probabilities of polypharmacy across IMD quintiles, accounting for all covariates in the model. Statistical significance was set at p < 0.05. To assess the robustness of our findings, we conducted sensitivity analyses using alternative polypharmacy definitions: ≥ 4 medications and a stricter ≥ 6 medications within the past seven days. The logistic regression model was repeated with these modified thresholds to determine if the association between deprivation and polypharmacy persisted. All regression analyses incorporated survey weights to account for unequal selection probabilities, non-response, and ensure representativeness of the English adult population [13]. All analyses were conducted using Stata (version 18).
Ethics approval
This study is a secondary analysis of Health Survey for England (HSE) 2021 data, so ethical approval was not sought. The original HSE 2021 study received approval from the East Midlands Nottingham 2 Research Ethics Committee (Reference no. 15/EM/0254), ensuring the protection of participants’ rights, safety, and wellbeing.


Comments (0)