This project aimed to test a new study design and quality parameter to evaluate medication history taking: It assesses updates instead of discrepancies to avoid taking two medication histories. We used this design to evaluate the feasibility of medication history taking by telephone. The design and the results of the feasibility study will be discussed separately.
Methodology
Our design aimed to provide a low-resource alternative to evaluate the quality of medication histories. The gold standard requires additional, time-intensive interviews (on average 30 min [4]) and places burden on patients. Our quality parameter requires only one interview per patient, as existing documents (PVML) serve as comparators instead of additionally acquired BPMHs. This reduces the time spent on patients and research resources.
Beforehand, there were two expected weaknesses of our design [15]: First, the availability of the PVML was expected to limit patient recruitment, but only 10% of patients lacked PVML information. The most common exclusion reason was discharge before written consent could be obtained. This might be linked to our specific intervention being conducted remotely and requiring an additional in-person contact, which is consistent with a similar study [25], but would not apply to all interventions. At this point, our design is suitable for settings with recurring admissions. With increasing standardization in documentation and the introduction of broad consent, these weaknesses will not affect the feasibility of the design significantly.
This pilot study revealed an important consideration in regard to the PVML: Although the distribution of days elapsed since its documentation in the patient population was relatively symmetric, we encountered a few outliers and a wide range (3 days to 15 years). Our exploratory analyses indicated a potentially significant impact of this factor on the primary endpoint. Therefore, future studies should introduce a maximum number of days elapsed as exclusion criterion or conduct stratified analyses. A previous study showed that most medication lists > 30 days old are outdated [28]. However, the appropriate maximum may also depend on the frequency of hospital visits in the studied population. In our setting, a maximum of 90 days, the usual time period between two visits, could have been set.
Secondly, our outcome parameter assumes that all updates are changes made to a patient’s medication therapy in primary care and, therefore, are correct, but naturally they could also be caused by errors in history taking. Like the BPMH technique, we followed a systematic approach for the interviews with specific questions to cover all types of medicines. Further, we used the PVML to verify apparent changes. Most updates found in our study were “changed” and “newly initiated” medicines, which we consider expectable modifications in the course of therapy. This was confirmed by the similar distribution of types of updates in both groups. In previous research, the most common discrepancies were omissions [29, 30], which indicates that dose and commission errors are less likely. Our BPMH phase showed that most discrepancies between standard-care histories and BPMH were caused by the PVML being adopted unchanged, not by recording incorrect information. We therefore believe that our outcome parameter—despite higher uncertainty compared to the gold standard—is a sufficiently reliable proxy. However, it has to be validated by comparison with the BPMH method.
Medication history taking by telephone
Telephone interviews proved feasible with a mean time expenditure of 15.7 min per patient. In general, patients were open to medication history taking by telephone in both groups, which aligns with previous studies [31]. The exploratory staff surveys showed that physicians were satisfied with the intervention and suggests 0–40 min saved daily per physician. Recording medication histories before admission could distort the admission day and render the telephone approach especially useful in time-sensitive settings with high workload and patient turnover.
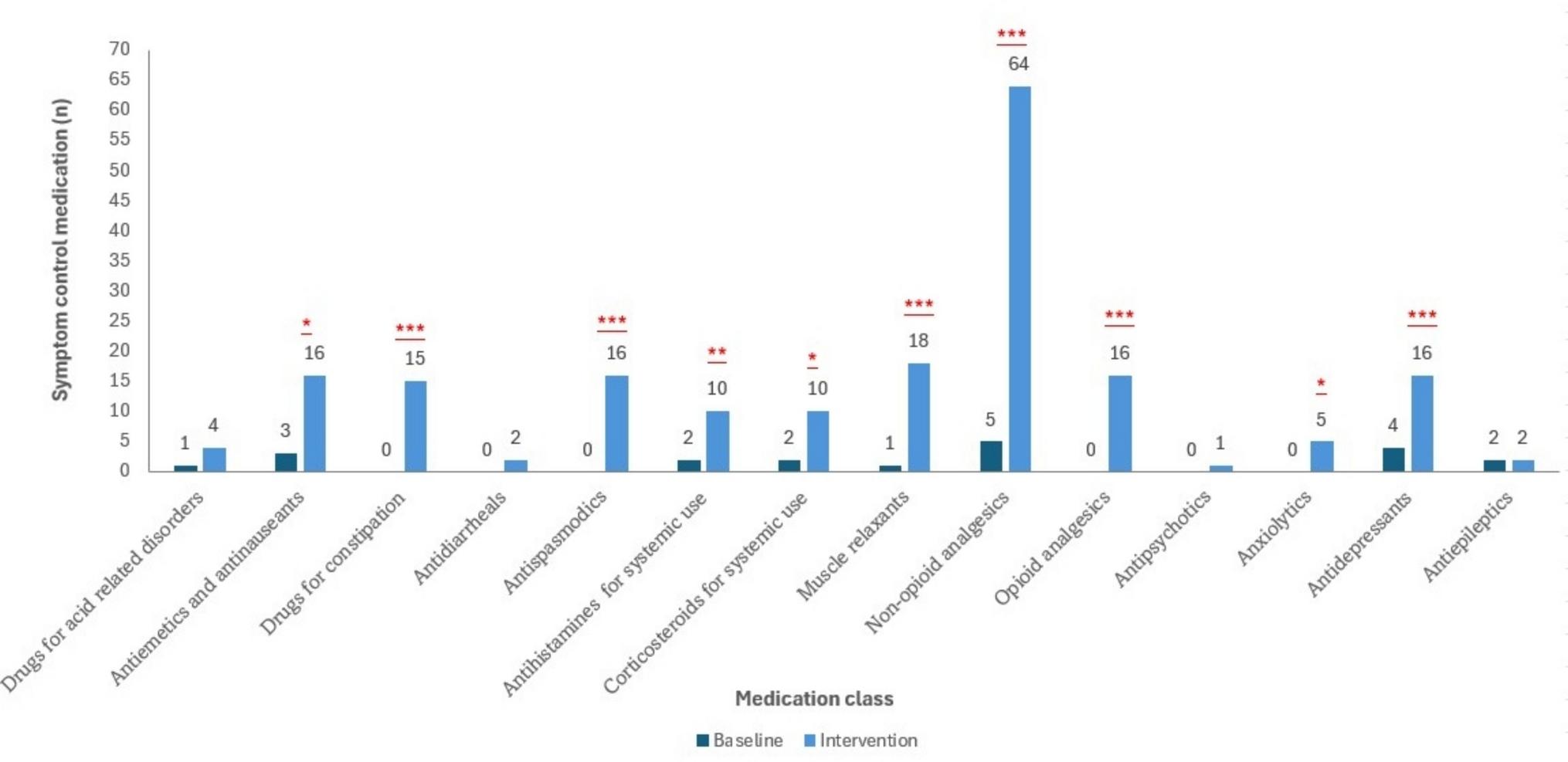
The statistically significant increase in the number of updates in favour of the intervention group suggests that the telephone approach might result in more comprehensive medication histories. However, we did not formally evaluate the clinical significance of this difference. Our analyses showed that updates mostly affected medicines used in the alimentary system (mainly anti-diabetics, drugs for acid-related disorders) and cardiovascular system (mainly diuretics, beta-blockers, lipid modifying agents), particularly update types “newly initiated” and “changed”. A previous study found the same drug classes to be affected the most by medication discrepancies (predominantly omissions and discrepancies in dose and/or frequency). Additionally, this study reported that errors concerning cardiovascular medicines and antidiabetics were potentially harmful [32]. Therefore, we assume that not identifying updates in these medicines might accordingly increase the risk of harm.
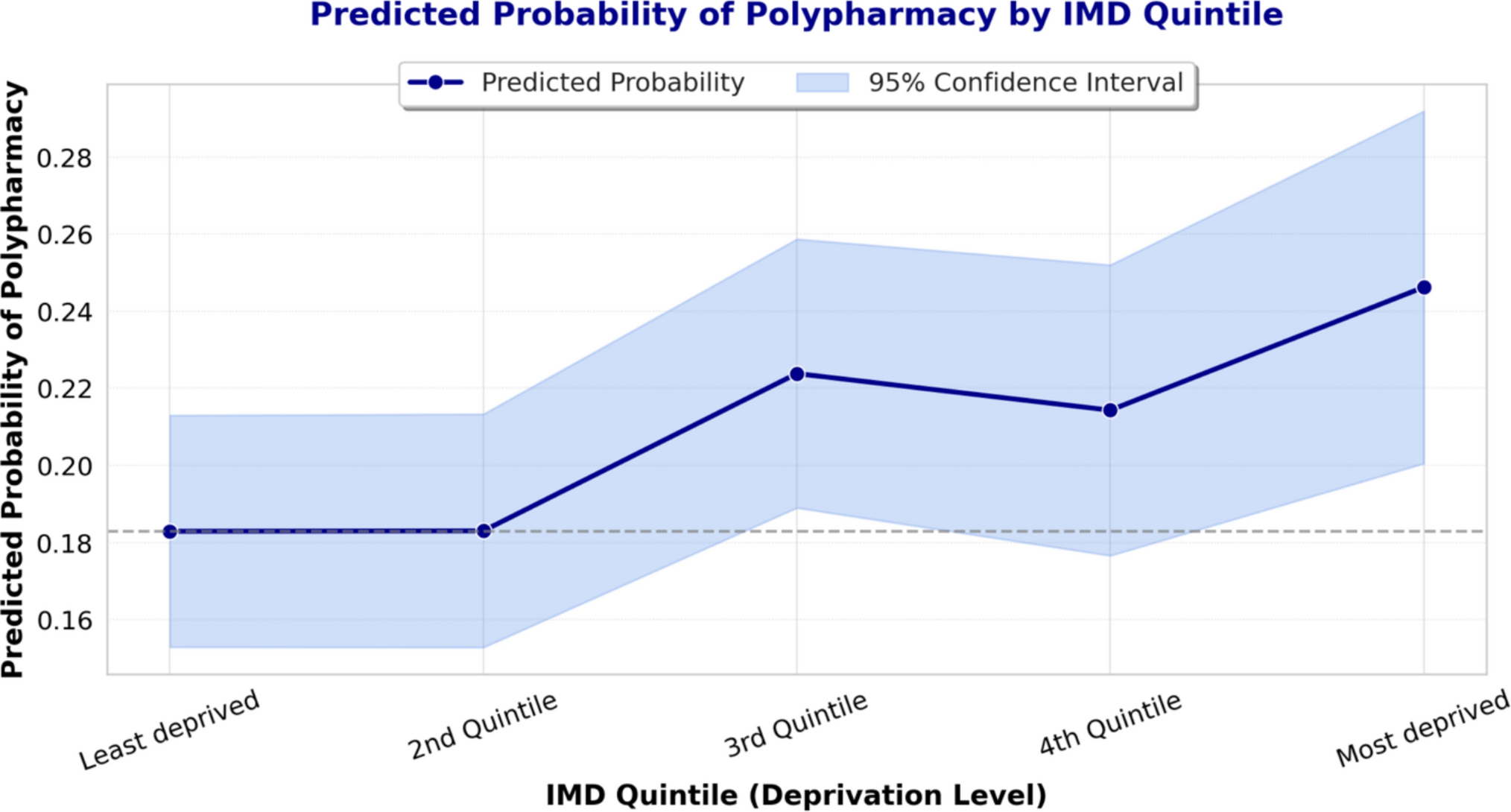
Similar to previous studies, we identified factors associated with a higher number of updates: hyperpolypharmacy (≥ 10 home medicines), increasing age, and a PVML documented ≥ 30 days before admission. Although these associations remain inconclusive across studies [28, 33,34,35,36], patients with these characteristics should be assessed more closely.
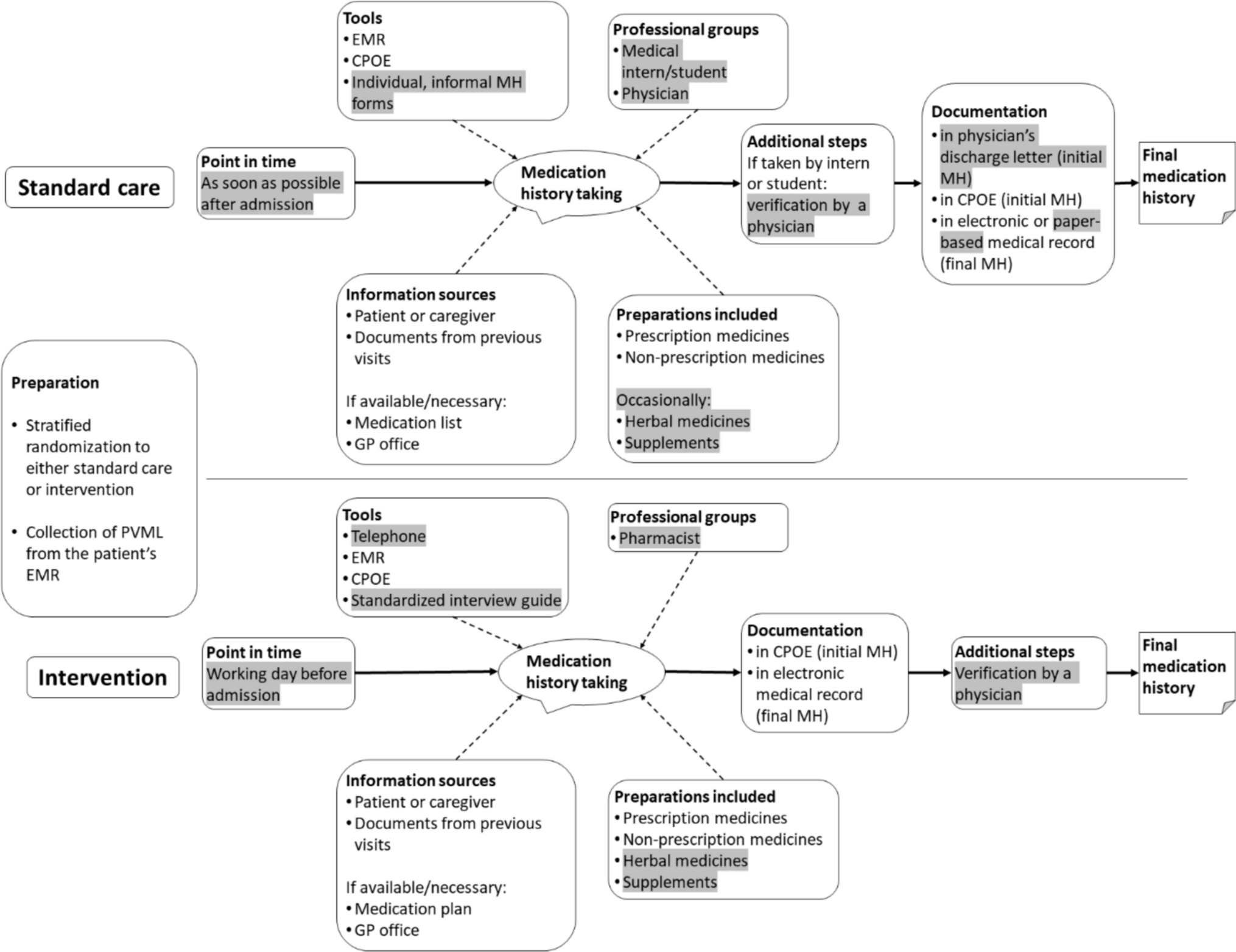
The observed difference in the number of updates could be explained by several aspects in which our intervention differed from standard-care: Histories were taken by a pharmacist instead of medical staff. It has been shown that these professions differ in the type of medicines they record [37] and that pharmacists tend to gather more comprehensive histories [31, 38,39,40]. Additionally, the pharmacist used a standardised form in our study, while physicians and medical interns used individual forms. Standardisation may positively impact quality according to literature [31, 41,42,43]. Although this constitutes a source of bias in favour of the intervention, we tried to minimize it by only including medicines and medicinal products in the analyses and by providing the pharmacist with the same information sources as the physicians (i. e., patient documents in the EMR). We believe that the earlier timing of the telephone interviews is the most important factor due to potentially fewer interruptions, which are generally common in admission interviews [4]. A previous study associated this with high completion rates of medication histories, because patients had easier access to their medicines at home [22], which corresponds with the results of our patient survey: Approximately 42% of patients found it easier to list their medicines from home. In other studies, the telephone approach provided accurate medication histories and was faster than face-to-face interviews with values between 5.8 and 8.25 min [23, 25], which is comparable to our results (6.3 min). However, to provide robust evidence on the individual impact of the aforementioned aspects, they would need to be studied separately or in a factorial study design. This was infeasible in our setting.
Based on the time measured, the staff survey and EMR data, pharmacist-acquired histories by telephone were more time-consuming than in-person interviews by physicians. Conversely, according to our primary endpoint, the telephone interviews were of better quality. This phenomenon is known as the efficiency-thoroughness-trade-off [44] and suggests that better quality might require (and potentially justify) a more time. However, due to the limited comparability regarding time expenditure (see Limitations) and the uncertain clinical relevance of the difference between the groups, a formal cost-effectiveness analysis was not undertaken. Apart from potential time savings and reduced admission-day workload for physicians, telephone histories might streamline subsequent processes (e.g., medication orders) and could, thereby, positively impact cost-effectiveness.
While the telephone approach was well accepted by patients, more than half of the survey participants rejected medication history taking via video-call, despite > 80% owning a suitable electronic device. Although our survey questionnaires do not enable qualitative content analysis due to the close-ended question format, individual comments of the participants suggested that video-calls may be considered too cumbersome. Online platforms were favoured, indicating a general receptiveness for digital formats in this population. However, for their implementation, factors such as age, digital and health literacy and general trust need to be considered [19].
Limitations
The major limitation of this study is the uncertainty of our quality parameter. The BPMH phase was performed on small sample size of six patients and cannot be considered a full validation. Accordingly, all p-values must be interpreted exploratively. Next, our quality parameter will be validated against the BPMH or medication discrepancies.
About 90% of patients assigned to the intervention completed the telephone histories. Even though telephone interviews were feasible for them, we managed to obtain written consent from only 56%. Patients not answering the phone were excluded, which could have biased the study, as telephone calls may be infeasible or undesirable for them.
We relied on estimates and data from the EMR for the time spent on medication histories in the control group. This might introduce bias, as interruptions cannot be accounted for, but reflects the reality of clinical practice. Physicians should have been monitored closely to obtain reliable data on time expenditure, however, this would have introduced observer bias.
Lastly, the questionnaires were not formally validated. Additionally, only four physicians participated in the survey on staff satisfaction. This small sample size reflected the staffing levels at the study sites with only two physicians on duty per ward. Due to high workload, the willingness to participate in this non-mandatory survey was low. Naturally, the results of the staff survey are exploratory and the low response rate limits their generalizability.


Comments (0)