
Remember me

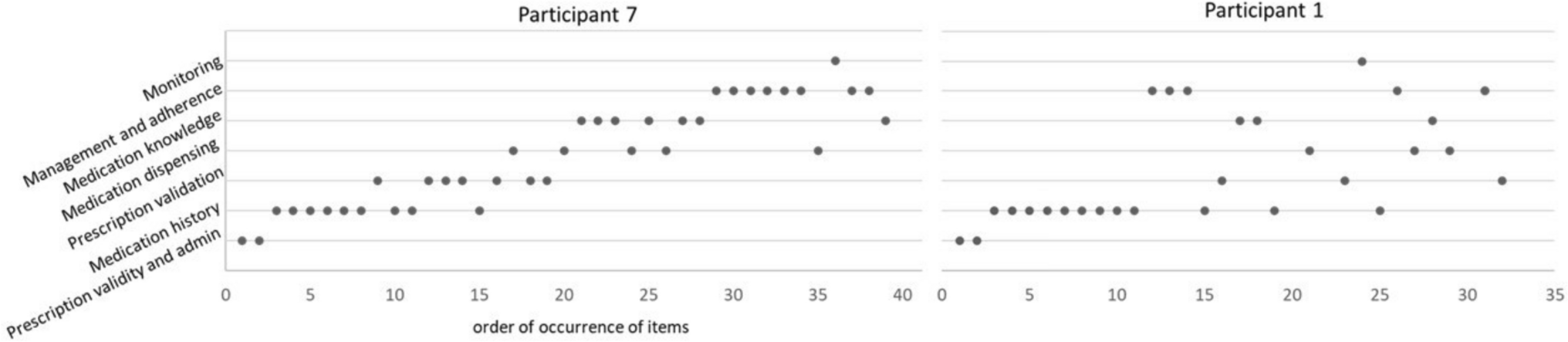
Table 1 profiles the 12 SPIs interviewed, ten of whom were qualified pharmacists. Two SPIs were pharmacy graduates. The results are presented in two parts: first, a process map of SPIs’ call-taking; second, three themes from the interviews that offer insight into how SPIs apply and develop their clinical decision-making skills.
Table 1 Interview participant characteristicsCall-taking process mapFigure 1 illustrates the SPI call-taking process. Across experience levels, SPIs described an iterative three-phase process: information gathering, risk stratification, and management decision (Supplementary Table 2). The three phases were iterative rather than linear, with SPIs moving between them fluidly during a call.
Fig. 1
Schematic map of the decision-making process used by the Specialists in Poisons information in the New South Wales Poisons Information centre
In the information-gathering phase, SPIs aimed to understand “what's actually happened here” (SPI07). They used resources such as the Australian electronic Therapeutic Guidelines, Australian Medicines Handbook, Australian National Poisons Register, MicroMedex, Monthly Index of Medical Specialities (MIMS), and Toxinz™ to assess whether the poisoning met “criteria for referral” (SPI08).
SPIs asked a mix of open and specific questions to document mandatory case note fields, such as exposure type, timing, and substance (see Supplementary Table 1). SPIs also explored social and contextual factors relevant to risk, including time of day, distance from hospital, support availability, and access to tools such as a blood pressure monitor. These factors were recorded in the open-text section of the case notes, though completeness varied.
SPIs synthesised this information with clinical experience to assess poisoning risk, working independently without decision support software. When the risk was clear, they advised home management (lower risk cases) or referred to ED (higher risk cases). For uncertain or more complex cases, they consulted colleagues or escalated to a clinical toxicologist. In some cases, they arranged follow-up calls to reassess and adjust the plan.
Although Fig. 1 presents the call-taking process in a linear format for clarity, interviews revealed that SPIs apply this process flexibly rather than following a rigid framework. They adapt their clinical decision-making in real time, tailoring their approach to each patient and situation. The following three themes, drawn from the interview data, offer deeper insight into how SPIs develop and apply these skills: balancing known and uncertain risks, maintaining decision-making flexibility under pressure, and the influence of experience and work environment.
Balancing known and uncertain risksSPIs’ decision-making centred on triaging poisonings based on risk assessment. This involved evaluating both known risks of the exposure and potential uncertain risks that could lead to deterioration without medical care.
During information gathering (Fig. 1), SPIs assessed the patient’s clinical status and checked whether a toxic dose had been exceeded, using guidelines. The presence of “red flag” substances, such as opioids, insulin, or sedatives, prompted a lower threshold for hospital referral. However, SPIs stressed that identifying known risks alone was not enough to guide management. As one SPI explained:
“it’s not like you can just look at a textbook and say OK, this is the referral dose. If they’re under, leave them at home, if they’re over send them in…there’s a nuance” SPI06
SPIs described this “nuance” as balancing known risks with the uncertain risk of deterioration. Poisonings in older adults often required a more “conservative” approach (SPI03) due to their vulnerability to adverse effects. Confidence in the patient’s ability to self-monitor influenced decisions, with social factors explaining why similar exposures could lead to different advice. Key considerations included time of day, location, available support, ability to monitor at home, and access to care, as one SPI noted:
“…realistically in an aged care setting, there’s very limited staff overnight, there's a good chance there's not a registered nurse on duty. So, in reality, who's going to be monitoring him?” SPI05
SPIs emphasised that their confidence in the reliability and completeness of the caller’s information was just as important, if not more so, than the nature of the poisoning. They considered factors such as the caller’s anxiety and English proficiency, which could affect understanding. SPIs assessed consistency by summarising and clarifying the sequence of events and later evaluated whether patients had “taken everything we’ve said on board” (SPI12) when giving advice.
These factors influenced how confident SPIs felt about a patient's ability to be safely monitored at home. If there was any doubt, they often chose to “err on the side of caution” (SPI03) and referred the patient to the ED.
Decision-making flexibility under pressureSPIs described the challenge of balancing known and uncertain risks in a “high-stakes, high-responsibility, high-speed environment” (SPI11). Making risk assessments under time pressure required flexibility, a skill that developed with experience working as a SPI. This need for adaptability was often reflected in the brevity of call documentation, a trade-off necessary to manage high call volumes.
The stress of tele-triaging was heightened during peak periods, particularly for complex cases such as calls involving older adults. One SPI recalled the pressure they felt as a newcomer:
“…seven [people] in the queue and you’re the only person there…there’s a tendency to want to wrap up the calls and move on to the next one quite quickly” SPI07
While NSW PIC SPIs no longer work solo, these same pressures still exist when multiple callers are in the queue during busy periods. Administrative tasks further intensified time pressures. Documenting call details and completing mandatory fields, such as the Poison Severity Score, were required before logging each call:
“it’s not just taking the call, and that’s it…We have to type up the call record…type in all the fields…everything they said and plus your advice…and then you have to code it as well” SPI04
SPIs described the conflict between gathering sufficient information for the current call and completing documentation, while knowing that any delay could impact patients with more severe poisonings waiting in the queue. However, they noted that this tension eased with experience. Newer SPIs tended to follow a structured, linear approach to information gathering (Fig. 1) and frequently referred to guidelines. Over time, experience translated into greater flexibility in call-taking. SPIs adapted their framework, relied more on clinical judgment, and developed an intuitive sense of “just knowing the questions to ask” (SPI05) and distinguishing between “need to know” and “want to know” (SPI02) information.
Decision-making became increasingly instinctive, with experienced SPIs describing a “hunch” (SPI03) or a “feel for what might be a risky situation and what might not…” (SPI10). With this, the flow and efficiency of calls improved, and SPIs recognised when to resist the urge to rush the call, even under high call volumes:
“If it was a simple call, I would speed it up and move through it. But if I was talking to someone confused or hard of hearing, it wouldn’t make any difference to how long I spent on that one…try and focus on the person you’ve got…even if they [other calls] have to wait, a person still needs your help.” SPI07.
The flexibility afforded to SPIs, allowing them to triage patients autonomously rather than relying on computerised decision-support algorithms, enabled more individualised risk assessments. However, balancing patient care with operational demands often led to retrospective documentation, particularly during busy shifts. One SPI illustrated this trade-off:
“on a busy shift, like I worked one the other night I was actually pretty good, I had at about 12 or 14 incompletes. One of the girls I was working with, got to a point where she had 30 calls that she had to type up…but we had been so busy….she's experienced and she'd been pumping through them…so then going back like many hours later, and looking at the brief notes you’ve typed in there and trying to remember the details and document all of that… that's part of the reason that documentation doesn't really encompass everything that we would like to.” SPI01
SPIs were also asked to record information that did not always directly influence clinical decisions and could be added later. For example, while the Phase One audit found that over half of older adults referred to hospital had a Poison Severity Score of ‘No Effect’ [25], SPIs clarified that a low score simply meant symptoms had not yet developed and did not rule out the need for intervention.
“It’s a coding thing that we put in the database, but it doesn't guide our decision” SPI04
In the context of a Poison Severity Score of ‘No Effect’ in the vignette, they acknowledged the Score’s value for research and tracking trends but emphasised that, in practice, decisions were guided more by the uncertain risks and the “expected trajectory” (SPI02) of the poisoning, particularly in complex cases involving older adults.
Decision-making experience and environmentOur findings highlight the critical role of experience and the work environment in shaping SPIs’ clinical decision-making. SPIs often “draw from… experience, what’s worked in the past” (SPI06) to decide when to conclude a call or spend more time assessing risk. While prior clinical experience as a pharmacist provided a foundation, structured training, peer review, and a supportive team environment were essential for developing tele-triage skills.
Previous pharmacy experience helped SPIs interpret key information, such as medication types, dosing, and packaging, and recognise signs of deterioration—balancing known and unknown poisoning risks. Those with hospital pharmacy experience noted that clinical exposure improved their ability to detect symptoms indicative of patient deterioration. Prior experience in interpersonal skills also helped assess whether callers were “switched on” (SPI05) or “muddled and confused” (SPI01), which could signal that “there’s something else going on” (SPI08). However, triaging acute, fast-changing cases was new for many and addressed through PIC training.
Most SPIs described the transition as a “steep learning curve” (SPI04), crediting peer support and team learning as crucial. Colleagues’ expertise was especially important when dealing with uncertainty in risk assessment, and shared case discussions helped build trust and foster system-wide learning. Peer learning was particularly valuable for newer SPIs, who felt “privileged” (SPI11) to learn from more experienced colleagues. Formal peer review (where each call record is checked by another SPI) ensured advice accuracy and supported skill development by helping new staff “understand the thought processes” (SPI06). Informal mentoring was also key, with senior SPIs offering feedback and role-playing calls to build confidence.
Experienced SPIs noted that learning was mutual, as newer colleagues contributed fresh perspectives:
“They’ve got their own clinical background that they sort of bring … I often learn a lot of stuff from new SPIs as well. So I think it goes both ways…” SPI06
Comments (0)