While the feasibility of high-quality 161Tb SPECT imaging has been demonstrated [15, 16], more detailed descriptions of the response in γ-camera imaging is lacking. In this study, we evaluated sensitivity, septal penetration, and count rate behavior for two different energy windows (48 keV ± 20% and 75 keV ± 10%) and two collimators (LEHR and MELP) using a Siemens Symbia Intevo SPECT system. These investigations are particularly relevant as the system is currently used in two clinical trials involving 161Tb-based radiopharmaceuticals (BETA PLUS; NCT05359146 and PROGNOSTICS; NCT06343038) [7, 10]. As future study phases will involve increased administered activities of 161Tb, we aimed to investigate dead-time effects in anticipation of potential limitations.
Sensitivity and penetration
The primary imageable emissions of 161Tb are relatively low in energy, making them more susceptible to in-patient attenuation. Even so, the sensitivity for 161Tb remains reasonable. In this study, the planar in-air sensitivity was determined to 15.7 and 18.5 cps/MBq for LEHR and MELP, exceeding values reported for similar systems using 208 keV 177Lu with a medium-energy collimator (e.g., 9.36 and 10.1 cps/MBq) [17, 18], likely due to the higher detection efficiency of NaI(Tl) at lower photon energies. When attenuation is present, the count rate per unit activity in the 161Tb 75 keV window (~ 6 cps/MBq, see Fig. 4) appears roughly comparable to that of the 208 keV window for 177Lu (~ 7 cps/MBq [17], deduced from tabular data).
At 48 keV, sensitivity is even higher than at 75 keV, partly, as this window includes not only the 49 keV γ-peak but also several intense X-rays (e.g., 45.2 keV, 6.28%; 46.0 keV, 11.2%) [11]. While quantification at this energy presents additional challenges—such as reduced recovery [16] and down-scatter contributions from the 75 keV peak—sensitivity remains favorable, making this window a potential asset at late-time point imaging. Overall, 161Tb demonstrates good potential for clinical imaging with reliable counting statistics.
For the 75 keV window, the in-air sensitivity (i.e., as measured at 10 cm) was similar for both collimators, yet slightly higher for MELP. However, at larger distances—where scatter and penetration are minimized—the MELP sensitivity remained higher than for LEHR (18.1 vs. 13.3 cps/MBq, Suppl. Table 1), highlighting that the primary count rate is indeed higher with medium-energy collimation.
A more notable difference between the collimators was noted for the 48 keV window (e.g., Fig. 4). At 10 cm, the planar sensitivity at 48 keV was 3.7 times higher than at 75 keV for MELP, whereas for LEHR, the increase was only 2.8-fold. This difference can, in part, be attributed to penetration effects; the contribution from down-scattered photons is higher for LEHR at 75 keV, which leads to a lower 48 keV-to-75 keV sensitivity ratio. At the maximum source-to-collimator distance—where the scatter contribution is minimized—the relationship between the two windows becomes more similar (see Suppl. Table 1), supporting the argument above. However, even at 40 cm, the 48 keV-to-75 keV sensitivity ratio remains slightly higher for MELP compared to LEHR (3.2 and 3.6, respectively, see Table 1, Suppl). One possible explanation is that the use of the MELP collimator increases the production of characteristic X-rays, which contribute more to the 48 keV window. This hypothesis remains to be verified.
Regarding septal penetration, the greatest degradation was observed for LEHR with the 75-keV window, reaching a peak PF of 22% at a 1-cm source-to-collimator distance in the planar Petri dish measurements (see Fig. 2). The effects of penetration were also evident in the SPECT measurements. At 75 keV, the count rate for projections acquired at the closest source-to-collimator distance was 34% higher than those at the farthest (5.06 vs. 6.78 cps/MBq), while for MELP, the increase was 25% (5.53 vs. 6.91 cps/MBq), see Fig. 4. Penetration poses challenges both qualitatively and quantitatively; visually, it can introduce streak artifacts and reduce image contrast, while quantitatively, it leads to unwanted contributions within the photopeak window, affecting measurement accuracy. Although methods of scatter correction, e.g., the triple-energy window (TEW) method, can mitigate these effects to some extent, minimizing penetration at the acquisition stage remains the preferable approach for ensuring reliable quantification.
The impact of penetration was evident when examining the energy spectra acquired (see Fig. 5). For LEHR, penetrating peaks are noticeable at, e.g., 292 and 550 keV. Although the yields of these emissions are low (0.058% and 0.036%, respectively) [11], they—along with other low-yield higher-energy emissions—still contribute significantly. For LEHR, 51.6% of all counts are recorded above the highest energy window, whereas for MELP the corresponding fraction is only 12.2%. This highlights how penetration is linked to dead time; penetration and scatter will result in unwanted counts, elevating the wide-spectrum count rate, thus, promoting dead time. Specifically, the wide-spectrum count rate was 51.8–75.0 cps/MBq for LEHR and 42.2–54.2 cps/MBq for MELP. Assuming dead-time losses are directly proportional to the wide-spectrum count rate, using MELP would increase the system’s measurement capability by 23–38%.
Dead time
In this study, dead-time was estimated intrinsically using a set of 161Tb point sources, measured at two separate occasions; a methodology similar to that described by Hjellström et al. [19]. This approach offers a quick and practical way of estimating the dead time, as opposed to extrinsic phantom measurements, which require more time and higher activity.
We assume that the measured dead time is applicable in a clinical setting, where collimators and scattering material will alter the energy distribution of detected photons. It is generally accepted that dead time is primarily dictated by the total count rate across the entire spectrum, which is what we have considered. Other authors have suggested that, when considering only the total count rate, dead time should be relatively independent of photon energy and nuclide [20, 21]. Also, the fractional dead-time loss within a selected photopeak window should be close to proportionate to that of the entire spectrum, unless pulse pile-up effects are severe [22].
This said, primary photon energy appears to have some influence on dead time. However, no exact relationship between dead time and energy has been described in the literature. Desy et al. and Frezza et al. measured dead time on the same Siemens Symbia T6 camera (a model similar to the device used in this work) using 177Lu and 99mTc, respectively, and reported values of 0.55 µs and 0.49 µs [17, 21]. In this study, we obtain 0.42 µs, suggesting a trend of increasing dead time with higher photon energy. This would be reasonable, as higher energy results in higher pulse amplitudes, potentially increasing the demand on the pulse height analyzer (PHA). Other components within the γ-camera could also impose limitations, but we do not have detailed insight into which components set the constraints or how they influence dead time.
Measurement geometry has also been shown to affect dead time. Heemskerk and Defrise conducted a comprehensive study of dead time using 99mTc [23]. They observed a reduction in the wide-spectrum dead time when a collimator was applied: 1.25–1.30 µs intrinsically with point sources, 0.99–1.07 µs extrinsically with point sources, and 0.87–0.94 µs extrinsically with a phantom including scatter. One possible explanation is, once again, that the collimator and scattering material reduce the average photon energy, making pulses easier to process by the PHA, thus, lowering the dead time. This suggests that the actual dead time for 161Tb in a clinical SPECT/CT setting—including collimators and patient scatter—could be lower than the intrinsic value estimated here. However, these results apply to 99mTc, which has a single primary energy of 140 keV. For 161Tb, with its broader energy distribution, the effect is expected to be less pronounced. Still, this highlights a limitation of our approach: the dead-time constant obtained from intrinsic measurements may overestimate the dead time experienced during clinical imaging with a collimated setup. These potential discrepancies should be kept in mind when applying the threshold estimates reported here to real-world imaging.
McIntosh et al. determined the 161Tb SPECT sensitivity in reconstructed images (corrected for attenuation and scatter) to be 14.2 cps/MBq for the 75 keV window with a LEHR collimator, based on measurements in the 250–2000 MBq range, using a similar system [15]. This aligns well with our planar sensitivity of 15.7 cps/MBq for LEHR. While the methodologies are not directly comparable—McIntosh et al. used dual-head acquisition with full correction, while we report single-head planar sensitivity—the agreement is consistent with the theoretical expectation that properly corrected reconstructed sensitivity should approximate planar sensitivity. Moreover, McIntosh et al. measured the sensitivity across a broader activity range (70–4990 MBq) using a NEMA IEC Body Phantom and a LEHR collimator, and reported that uncorrected dead-time effects became apparent above 2 GBq. However, they also observed an activity-dependent variation in sensitivity across the entire examined range, attributing the higher sensitivity at low activities to reconstruction-related issues. At 5 GBq, they estimated dead-time losses of approximately 20%. The discrepancy between their findings and ours could be due to camera-specific differences or variations in measurement geometry. Nonetheless, their results support our predicted critical activity levels, reinforcing that dead-time effects occur at significantly lower activities for 161Tb compared to 177Lu.
It is worth noting that Siemens systems generally appear to perform well in terms of dead time. Desy et al. measured a dead time of 0.49 µs for 99mTc with a Siemens camera, whereas two GE cameras using the same method showed considerably higher values, 1.74 µs [21]; hence, the critical activity levels predicted in this work could be significantly lower with a different system.
One important factor to consider is the dead-time saturation threshold. While other modern systems have been shown to follow a more purely paralyzable behavior [19, 21], the system examined in this study exhibits a gradual reduction in count rate—well described by the Sorenson model—followed by a sharp drop. This occurred at distinctly different levels for the two detector heads (384 and 546 kcps, respectively), a phenomenon also observed by others [21]. Desy et al. also reported significant differences in saturation levels depending on which detector heads were active, with saturation thresholds of 480 and 290 kcps for dual-detector acquisition, while in single-detector mode, they measured 700 and 475 kcps [21]. A similar pattern was confirmed in another study using the same camera model [18]. While dead-time behavior below the saturation threshold appears independent of detector activation, this has important implications for our study: since our measurements were performed in single-head acquisition mode, the predicted critical saturation activities may be significantly lower.
Clinical implications
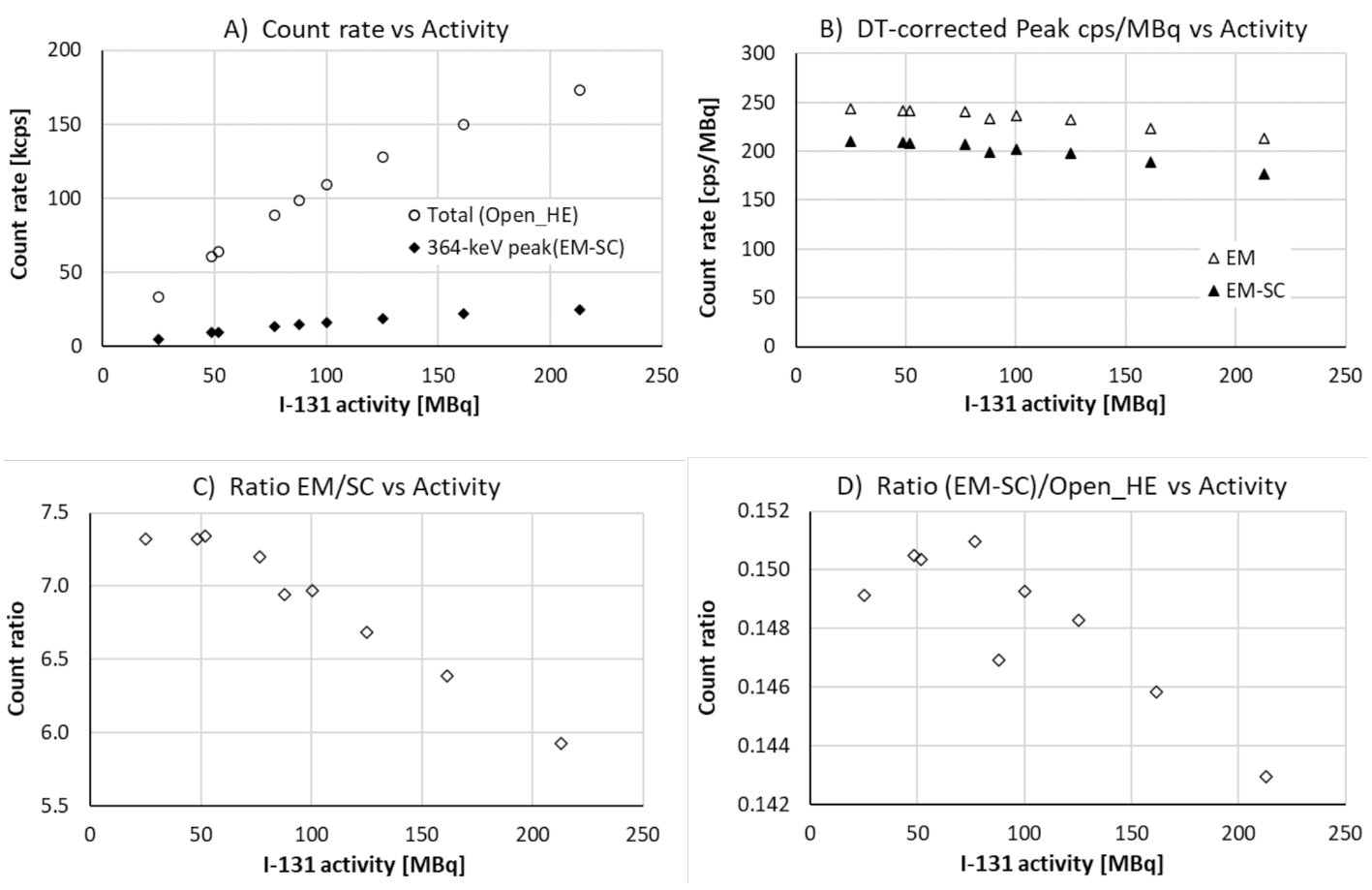
Concerning dead time, the patient count rates observed for 1 GBq of [161Tb]Tb-DOTA-LM3 were well below the range where dead-time effects are expected (Suppl. Table 2), with an estimated median whole-spectrum count rate of ~ 20 kcps at 3 h p.i. However, at therapeutic activity levels, dead-time effects could become significant. Assuming a linear relationship between count rate and activity, an administered activity of 7.4 GBq would correspond to a median count rate of approximately 150 kcps and a maximum of around 300 kcps at 3 h p.i., leading to estimated dead-time losses of 6.5% and 13.6%, respectively. For comparison, Uribe et al. reported typical whole-spectrum count rates of 50–70 kcps for patients treated with 7.4 GBq of 177Lu at 4 h p.i., which is about one third of the values observed in our study [21].
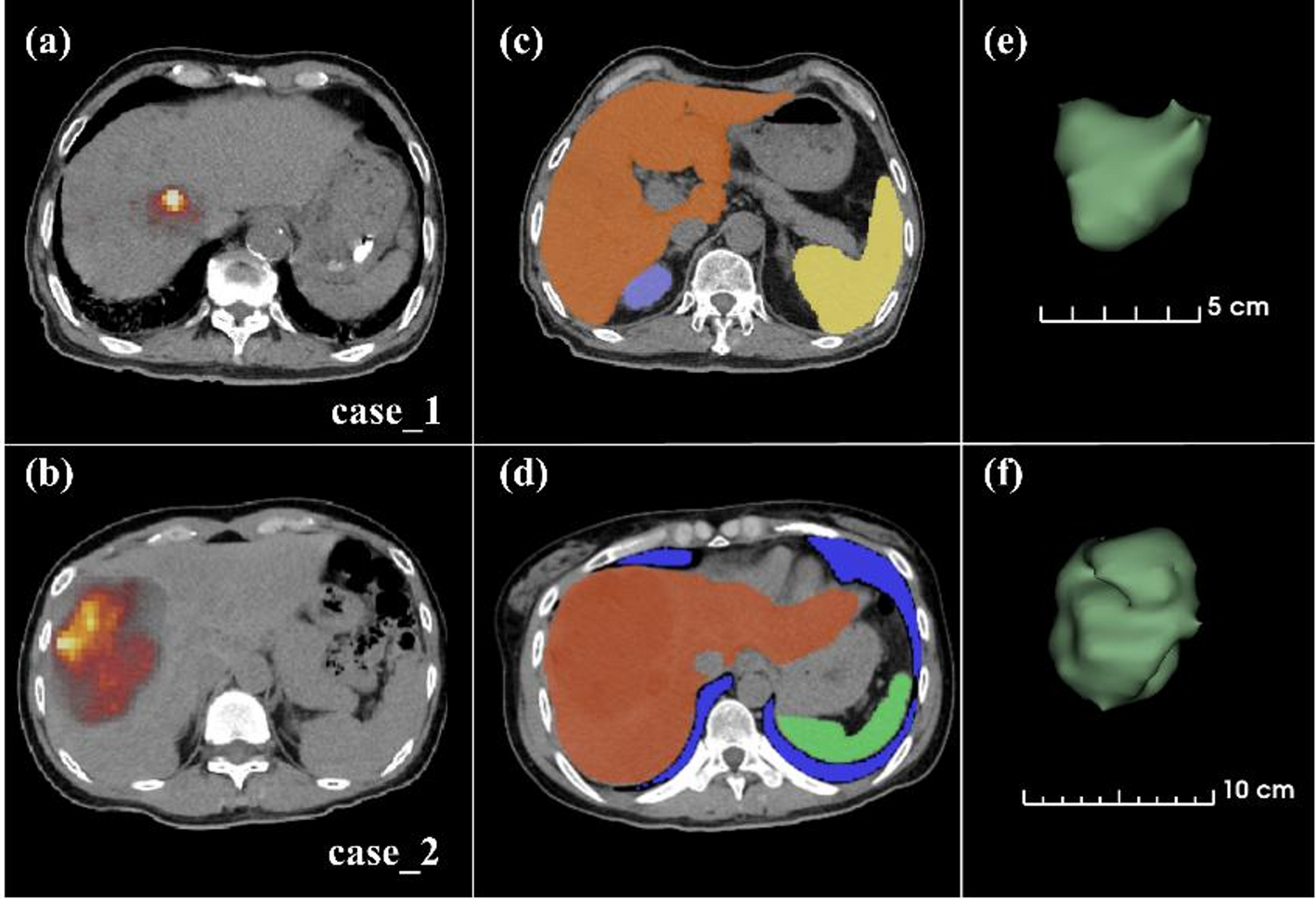
It should be noted that our dead-time estimates are based on measurements with a cylindrical SPECT phantom. In a clinical setting, patient-wide spectrum count rates may be even higher due to increased scattering. Additionally, patient positioning plays a crucial role. For the patients in this study, high-activity regions (e.g., liver, kidneys, and spleen) were distributed across two FOVs. A single FOV centered on the abdomen would result in even higher count rates and increased dead time. Moreover, while we assume a linear relationship between administered activity and count rate, nonlinear effects in biodistribution and kinetics at higher activity levels cannot be excluded and may influence the actual count rate.
In terms of recommended settings for clinical imaging, the findings in this study suggest that medium-energy collimation combined with a 75 keV ± 10% energy window offers more robust prerequisites for quantification, as it reduces degradation from septal penetration and dead time. This contrasts with current literature, which supports the use of low-energy collimation [15, 16]. That said, centers with access to advanced reconstruction methods and the ability to measure and correct for dead-time losses may achieve sufficient accuracy even with low-energy collimation, benefiting from improved spatial resolution. Ultimately, optimal imaging parameters—including collimator type and energy window—may need to be adapted based on the specific system and reconstruction capabilities available at each center. Regardless, for early time-point imaging with 161Tb at clinical activity levels, dead-time effects should be closely monitored and possibly accounted for.
In a clinical setting, the 48 keV energy window may offer advantages for delayed acquisitions due to its higher sensitivity. However, this window is more susceptible to scatter degradation—including 75 keV down-scatter, characteristic X-rays, and increased coherent scattering—which can vary significantly between patients. Obtaining good quantitative accuracy would therefore likely require more a robust scatter correction, ideally Monte Carlo-based.
Based on our preliminary experience, a practical strategy could be to reconstruct both energy windows separately with individually optimized parameters. If agreement between the two windows is observed at earlier time points, the 48 keV window could be used to replace or complement the 75 keV estimate at later time points, when count rates are low. Defining a count threshold within the VOI below which the 75 keV window becomes unreliable may offer a practical trigger for switching to the 48 keV window.
It should also be noted that dead-time effects may be more pronounced at 48 keV at high activities, due to pulse pile-up. Additionally, the attenuation correction at this energy is likely more sensitive to spatial misalignments, e.g., misregistration between SPECT and CT due to patient movements, which could introduce larger errors compared to the 75 keV window.




Comments (0)