A targeted statistical interaction analysis, complemented by a case series review, highlighted challenges in detecting DDI signals during pregnancy. Initially, the application of a pregnancy identification algorithm and the omega disproportionality method helped identify potential DDIs. However, due to limitations in the available data, particularly concerning the timing of adverse events and drug exposure, these signals could not be pursued further.
4.1 Methodological Points of Attention
Signal detection of DDIs in this study is based on disproportionate reporting in VigiBase. AERSs have limitations, including potential underreporting of concomitant medications, misclassification of concurrent medication, missing data, and lack of verification against source documents. These limitations may affect the interpretation of the disproportionality analysis, especially in identifying DDIs.
4.1.1 Selecting Reports on Exposure During Pregnancy
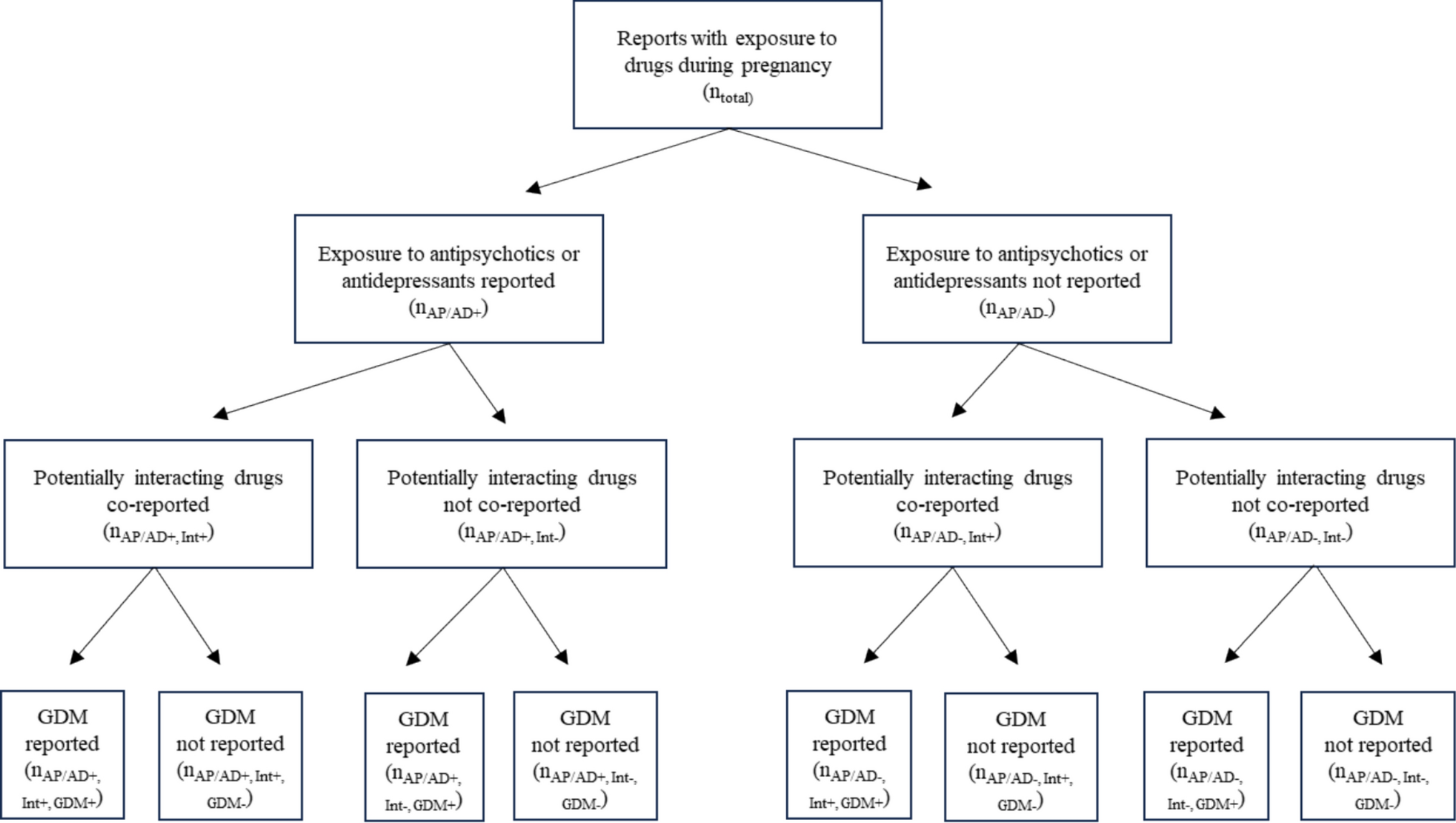
This is one of the first applied studies using VigiBase’s newly developed algorithm that enables reliable selection of pregnancy cases [25]. AERS reports related to exposure during pregnancy can be documented in two ways. A report might concern an adverse event observed in the foetus/child and mention maternal exposure to a medicinal product. Second, a report could pertain to the mother's use of the medicinal product, with the pregnant woman experiencing adverse events. It should be noted that reports of GDM are always related to the second method of reporting (the use of a medicinal product by the expectant mother) and not to reports on adverse events observed in the foetus/child. For this reason, these two types of reports will not be equally distributed over the eight cells of the matrix shown in Fig. 2. Reports related to the mother are included in cells related to the concurrent use of the two drugs of interest and in cells related to the use of either drug on its own, in the presence as well as the absence of GDM. However, reports related to the foetus/child are also included in cells related to the concurrent use of the two drugs of interest and in cells related to the use of either drug on its own, but they are not present in the cells related to the presence of GDM since this reaction is related to the mother and not to the foetus/child. It is possible that differences in the presence of both types of pregnancy-related reports could introduce a bias in the analysis.
4.1.2 Characteristics of Medication
Previous studies on DDI signal detection using VigiBase included drug pairs if the reporters listed the two drugs as ‘suspect’ or ‘interacting’ in either the reports or the case narratives [7, 26]. Strandell et al. [26] investigated the reporting pattern of unknown DDIs by requiring at least three reports for which the drugs of interest were characterised as suspected, interacting, or concomitant and at least one report in which the two drugs under study were reported as suspected or interacting. Hult et al. [7] used multiple predictors, including the omega value, possible metabolic pathways via CYP450 for the drugs of interest, and a suspicion of a DDI mentioned in the case narrative, in their predictive model for statistical signal detection of DDIs. With some exceptions, their study included reports in which the two drugs of interest were characterised as suspected or interacting. Other studies did not distinguish between assigned characteristics for the analysis of potential DDIs in AERS datasets [27,28,29,30].
In our study, no distinction was made between the assigned characteristics of the used medication as indicated by the reporter. This could help to identify potential DDIs even if the reporter did not specifically mention any interactions. However, this approach depends on the reliability of medication classification. Therefore, it may be advisable to limit statistical interaction analyses to drugs labelled as suspected or interacting until it is possible to reliably determine whether concomitant drugs were used concurrently or in the past. Strandell et al. [26] found that including concomitant medicines in interaction disproportionality analysis with the omega measure did eliminate its predictive ability for DDIs but that the mechanisms for this could only be hypothesised. Our study corroborates this finding and provides further empirical evidence (albeit in a small set of examples) that an explanation may be that many drugs listed as concomitant in fact relate to historical use.
Not distinguishing between suspected, interacting, or concomitant drugs led to the inclusion of reports where medications other than those under investigation were suspected as linked to GDM. For example, in 31 reports, quetiapine was identified as the suspected drug, whereas the two drugs of interest were listed only as concomitant. Although quetiapine was frequently suspected, no elevated Ω value indicated a DDI involving CYP450 pathways. However, this does not rule out other mechanisms, such as a pharmacodynamic interaction with ADs through additive effects on H1 or M3 receptor antagonism [31,32,33].
4.1.3 Timing and Course of Events
The occurrence of GDM is determined not only by the start date of the use of suspected or interacting medication but also by the gestational age (GDM testing is usually performed between 24 and 28 weeks of pregnancy), which makes it difficult to class a drug as suspected or interacting. It is therefore conceivable that drugs that have been used for some time, even before pregnancy, may still have played a role in the occurrence of GDM. For this reason, we considered all drugs in this study, irrespective of their characterisation in the reports.
Hult et al. [7] and Strandell et al. [26] included positive dechallenge and rechallenge for at least one of the two drugs with the adverse event as part of a composite predictor in statistical signal detection also including other information elements. Unfortunately, this positive dechallenge and rechallenge approach was not possible in our analysis since the development of GDM depends, next to gestational age, on multiple factors such as maternal age and body mass index. Therefore, it is unclear whether glucose levels would be affected immediately after a medication is stopped or re-introduced.
Two drugs used simultaneously may be flagged as a suspected DDI if there is a temporal overlap between the their use and the occurrence of the adverse event. A scoping review described the possibility for integrating variables such as simultaneous duration of suspected DDI drugs to be more effective than relying solely on disproportionality analysis [34]. In addition, Battini et al. [35] recently developed a novel method for detecting DDIs that incorporated temporal plausibility to avoid false-positive disproportionality signals in AERS.
4.1.4 Use of Standardised Drug Grouping in Detecting Signals of DDIs
Earlier studies using disproportionality analysis to investigate DDIs where potential class effects might be significant have typically conducted separate analyses for individual drugs. For instance, Strandell et al. [36] conducted a study in VigiBase on possible DDIs between azithromycin and individual statins (atorvastatin, lovastatin, and simvastatin) in rhabdomyolysis. SDG subgroups typically classify medicines based on their pharmacological effects or their metabolic pathways [18]. In our study, we considered the presence of any drug within the relevant SDG subgroup, enabling us to explore a potential underlying mechanism rather than the impact of individual drugs. Therefore, utilizing SDGs in disproportionality analysis could facilitate the examination of the pharmacological mechanisms behind ADRs or DDIs.
4.1.5 Evaluation of Reliability
Examining reliability was inherently subjective, as no established criteria existed for evaluating the quality of DDI signals during pregnancy. Although objective criteria could have supported a more consistent evaluation, such standards were not available. A key aspect of applying a statistical approach within an AERS is the need for follow-up review of the underlying case reports [37]. Therefore, the usefulness of the method was primarily evaluated based on this detailed case assessment. The subsequent case series review revealed several data quality issues (see Section 4.2).
4.2 Case Series Analysis
Disproportionality analysis should be completed by a clinical case review aimed at synthesising the characteristics of the reports with information related to causality assessment [37]. For instance, the Council for International Organizations of Medical Sciences working group VI published an overview of data elements that should generally be considered when assessing reports [38]. In this study, we focused both on data elements characterizing these reports in general and on information that was specifically needed for the assessment of potential DDIs and the quality of information on GDM and medication use.
4.2.1 Characteristics of Reports
The number of reports from North America was high (43/53), but no major differences between the three ADs highlighted were observed. In respect to the level of documentation, we noted that the median vigiGrade completeness scores were in line with the median completeness score for overall reports in VigiBase (2007–2012), which was 0.41 (interquartile range 0.26–0.63) as reported by Bergvall et al. [23].
It is possible that consideration of a possible DDI may differ between HCPs and consumers; however, unfortunately 22 reports did not include information about the reporter’s qualification. HCPs may suspect a specific drug as responsible for inducing GDM based on available literature, whereas consumers may not have access to this information or may be less aware of the risk for potential DDIs.
The quality and completeness of information in reports may differ according to the reporter's qualification and the nature of the reported drug–adverse event combination. Although the scores for the completeness of reports in this study are comparable with the average score of overall reports mentioned by Bergvall et al. [23], the scores are below 0.8, which is the cut-off value for well-documented reports in the same study. Also, the quality of case reports or the data provided differs between countries, which may limit the generalisability of interaction analysis outcomes. Nevertheless, they allow the generation of hypotheses that require validation through other methodologies, such as clinical trials and observational studies.
Although the use of multiple drugs in patients with psychiatric disorders is common, the reported number of drugs was notably high, particularly considering that this involves a pregnant population. The median number of drugs varied between 8 and 13 across the three highlighted DDIs, suggesting that certain medications used previously were reported as being taken simultaneously. Lastly, among 13 cases suggesting a potential DDI between citalopram and a CYP2D6 inhibitor, three were likely to be duplicates, despite prior screening with the vigiMatch algorithm [21]. Due to slight differences in reported drugs and distinct report IDs in the statistical analysis, they were treated as separate cases in the case series review, although they may refer to the same patient.
4.2.2 Additional Information on Medication and Possible DDIs
The possibility of a DDI was not explicitly stated in the narratives or additional comments of the investigated reports. It remains possible that additional information could be present in narratives that were not shared with VigiBase and therefore could not be considered in our study.
The analysis in this study focused on the interaction of two drugs only, but multiple concurrent drugs may be involved. As an example, for one substrate, multiple 2D6 inhibitors were found in 10 of 53 reports. Also, possible DDIs may have occurred for drug combinations or CYP450 routes other than those that were studied. For example, for the use of escitalopram and fluoxetine, we identified a statistical signal via 2D6 enzyme inhibition, but this drug pair could also interact via inhibition of 2C19 since fluoxetine is also a strong inhibitor of this enzyme.
4.2.3 Information on Timing of GDM and Medication Use
If data regarding drug use and adverse events are missing, there is a potential for information bias, which could result in misinterpretation of the DDI signal [22]. The case series review showed room for improvement in the information on medication use. Misclassification as concurrent drug use may occur in two directions. Our study indicates that unexposed patients may be mistakenly classified as exposed when drugs are incorrectly attributed to concomitant medication rather than recognized as past drug use. This may incorrectly increase the chance of signals on DDIs. Conversely, exposed patients could also be misclassified as unexposed. For instance, this might occur if a reporter omits concomitant medications while documenting a well-known ADR for the suspected drug—such as hyperglycaemia caused by olanzapine—focusing solely on this drug and overlooking other potentially interacting drugs. This scenario may reduce the ability to identify potential DDIs.
A detailed review of drug start and stop dates revealed that some drugs labelled as concomitant were no longer in use when GDM was reported, suggesting past rather than concurrent use. The drug start date occurred after GDM onset in 10 reports, and the onset date of GDM was missing from 24 reports. These findings highlight the importance of including both drug start/stop dates and the timing of event onset.
Multiple drugs from the same class were often reported as being used concurrently. For example, although SSRIs are commonly prescribed during pregnancy because of their better tolerability, co-prescribing two SSRIs is rare and discouraged because of the risk of serotonin syndrome [39]. This suggests that some drugs were likely used sequentially rather than simultaneously and should be considered part of the medication history and not as concomitantly used drugs. However, limited data on start/stop dates prevented us from distinguishing concurrent use from past use relative to GDM onset.
4.3 Mechanism of Potential Interactions Involving Antipsychotics or Antidepressants
Evaluating pharmacological plausibility is a crucial component of disproportionality analysis, as it helps to assess the validity of safety signals [37]. Consequently, pharmacological considerations of potential DDIs should be incorporated into the assessment, as they contribute to determining the likelihood of a causal relationship. The causal link between AD use and diabetes remains unclear, but differences in receptor-binding affinities suggest that the diabetes risk may vary by AD class. ADs with high H1 receptor affinity (e.g., tricyclic ADs) have been linked to an increased risk of GDM [40], whereas ADs with M3 antagonism or H1/muscarinic activity have been associated with a higher risk of type 2 diabetes mellitus [31, 33].
Our study focused on pharmacokinetic DDI mechanisms, but pharmacodynamic interactions involving H1, 5-HT2C, or M3 receptors may also contribute to DDI-related diabetes. Although the mechanisms underlying type 2 diabetes mellitus and GDM differ somewhat, receptor-level effects may be similar. The ADs studied are primarily metabolized via CYP3A4 and CYP2C19, so CYP2D6 inhibition may have limited impact unless multiple pathways are involved [41]. Studies have linked GDM to metabolic atypical APs such as clozapine, olanzapine, and quetiapine [42, 43]. However, we found no DDI signals involving these APs and CYP450-modifying drugs. Clozapine and olanzapine are mainly metabolized by CYP1A2, and quetiapine/aripiprazole by CYP3A4 [19, 44]. Although potential DDIs with CYP2D6 inhibitors have been suggested, the impact may be limited since CYP2D6 plays a minor role in metabolizing these APs [45]. Some studies have reported increased clozapine levels with SSRIs, but findings are inconsistent. Given that clozapine requires therapeutic drug monitoring, any DDI-related increase in plasma levels is typically managed through dose adjustment, limiting clinical relevance. The fact that these DDIs are known to occur may hamper reporting.
4.4 Strengths and Limitations
This work offers valuable insights into the complexities of medication use during pregnancy and highlights areas for future research and refinement of detecting signals of potential DDIs in spontaneous reporting systems. In addition, it shows the possibility for a more targeted examination of potential DDIs within this special population. Finally, the study employs a comprehensive approach by combining statistical signal detection with a detailed and structured case series review, providing a nuanced understanding of the possibility of signals of DDIs.
As this is the first study of its kind, it was not possible to define in advance criteria for the quality of the data. Information on predetermined criteria using the existing gold standards would have been welcome.
We identified several aspects that could be improved to optimise medication overview reporting, which could enhance the accuracy of analysis. As with other studies based on spontaneous data, the results should be interpreted with caution. Based on our findings, despite a statistically significant signal, no firm conclusions can be drawn on the existence of DDIs leading to an increased risk for GDM between an AP or an AD and a 2D6 inhibitor.
Lastly, apart from the influence of certain AP or AD use, the incidence of GDM has also been widely reported to be influenced by many other individual risk factors, such as genetics/family history of diabetes, maternal age, ethnicity, pre-pregnancy body mass index > 30 kg/m2, diet, sedentary lifestyle, and comorbidities such as polycystic ovary syndrome [46,47,48], which we were unable to include in our interaction analysis because of the lack of information and the relatively low number of reports.
4.5 Future Studies
It is crucial that pregnancy reports include information essential to differentiate between concurrent and prior drug use during pregnancy. Efforts should be made to optimize capturing and reporting of drug exposure timing to support a more accurate distinction between past and concurrent use, thereby enhancing the possibility of DDI signal detection in this population. Future studies may also consider developing new methods that incorporate temporal plausibility in DDI analysis during pregnancy, as shown by Battini et al. [35].


Comments (0)