
Remember me
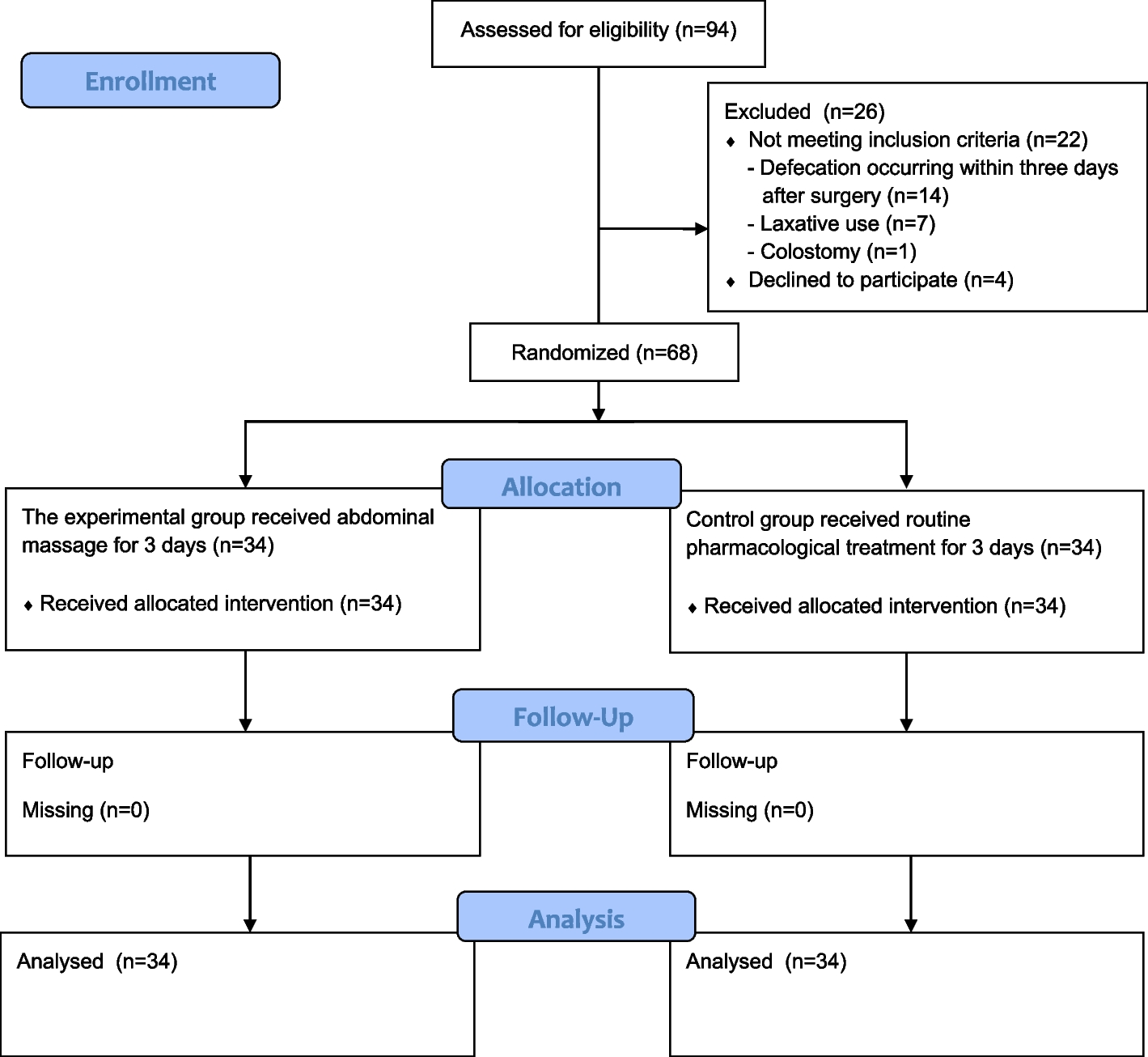
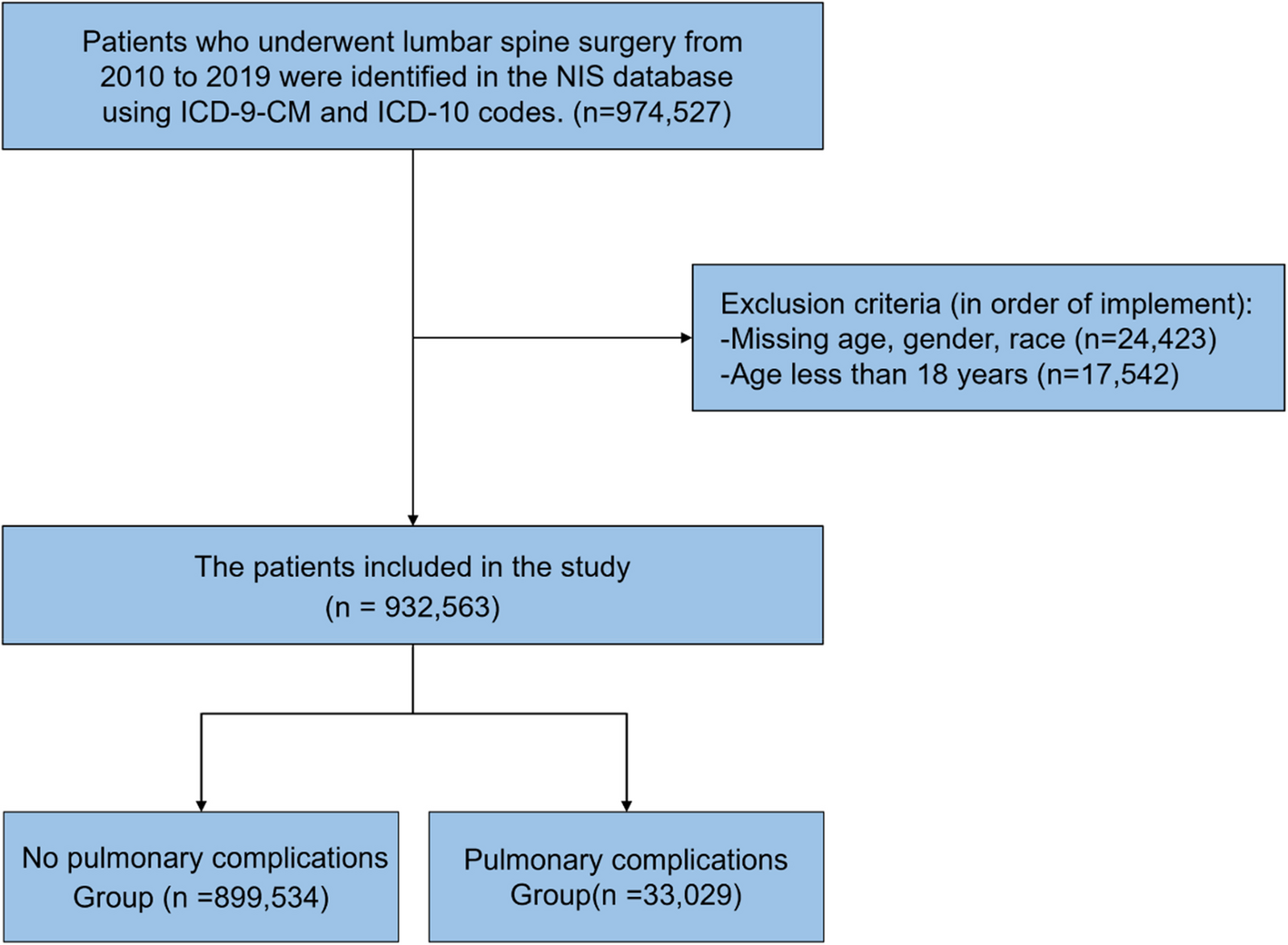
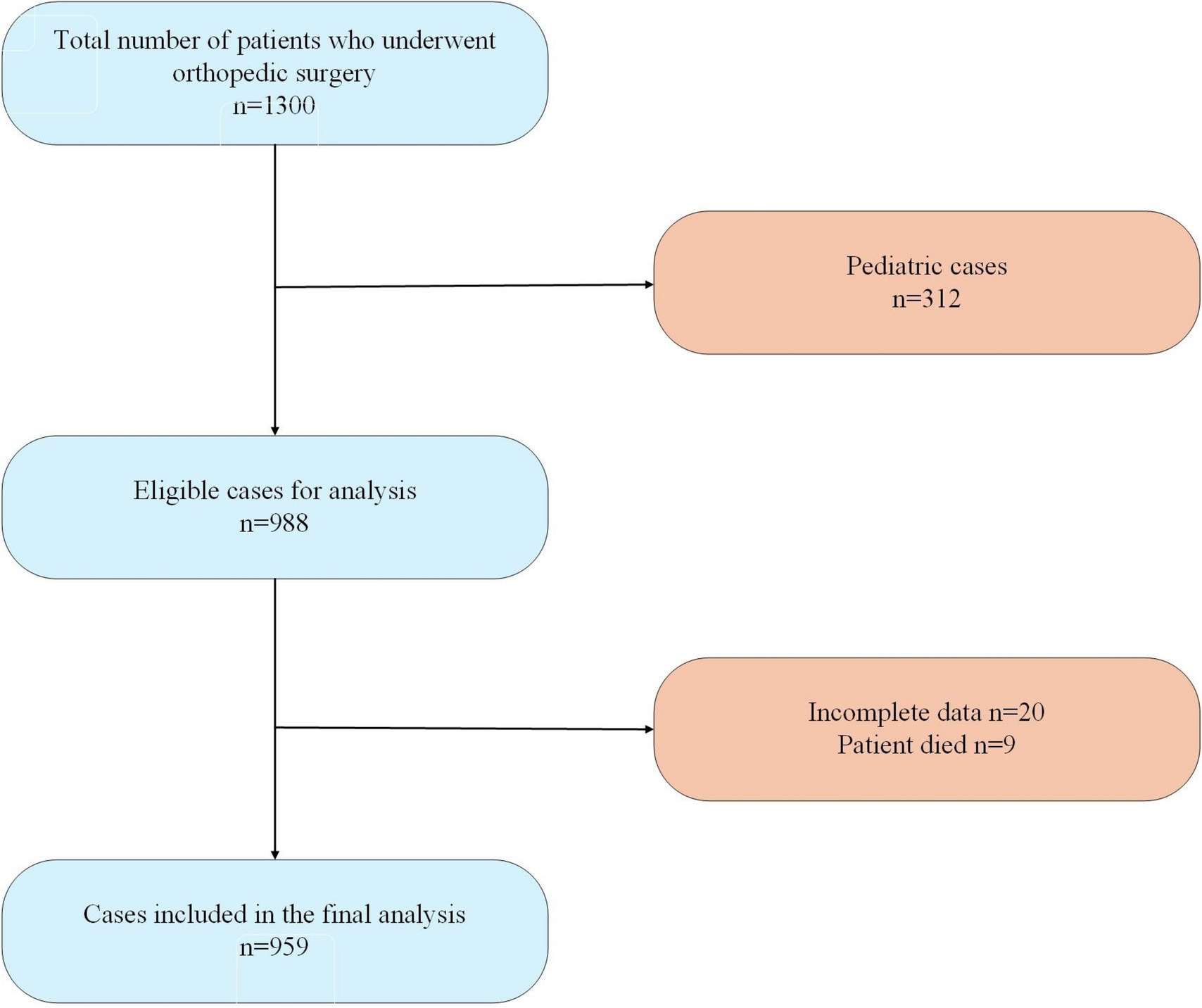
The randomized controlled experimental study was registered at https://clinicaltrials.gov/ and conducted by CONSORT guidelines (Schulz et al. 2010) (Fig. 1).
Fig. 1
CONSORT flow diagram for this trial
Study population and sampleThe study population consisted of patients hospitalized in the orthopedics and traumatology clinic of a university hospital in the province of Istanbul between September 2022 and September 2023. The study sample consisted of 68 patients: 34 in the experimental group and 34 in the control group, as determined by power analysis (G*Power 3.0.10), with an effect size of f = 0.20, 90% power, and a 5% margin of error. The primary outcome for the power calculation was the Gastrointestinal Symptom Rating Scale (GSRS) score. The effect size was calculated based on a mean difference of 0.60 points in GSRS total scores between groups, with an assumed standard deviation of 0.80, derived from findings in previous studies with similar populations (Aydinli and Karadağ 2023; Turan and Aştı 2016; Mutlu et al. 2024). This sample size was sufficient to detect significant differences between the experimental and control groups.
The inclusion criteria were as follows: the patient was 18 years of age or older, was conscious and coherent, had typical vital signs after the surgical intervention, did not defecate within the first 3 days after the surgical intervention, and continued inpatient care and treatment in the orthopedics and traumatology clinic of the hospital for at least 6 days.
RandomizationPatients to be sampled were assigned to the experimental and control groups by computerized (https://www.random.org/) randomization. The study was completed with 68 patients. A researcher who was not involved in the central randomization, assessment, and intervention processes generated the randomization list and assigned participants to the interventions. Owing to the nature of the study, blinding could not be performed because the researcher and the participant were aware of the intervention.
Research procedure and dataData collectionData were collected via the Patient Information Form, Functional Independence Measure (FIM), Bristol Stool Scale, Gastrointestinal Symptom Rating Scale (GSRS), and General Comfort Scale (GCS).
Patient Information FormThis form, created based on the literature (Turan et al. 2017; Turan and Aştı 2016; Nouhi et al. 2022), included questions about the patient’s characteristics and disease characteristics, the time of first gas and stool production, initiation of oral intake, bowel sounds, and mobilization status.
Functional Independence Measure (FIM)The FIM was developed by Granger and colleagues in 1986. It evaluates the individual’s function in two main areas: motor function (13 activities) and cognitive function (5 activities). The scale consists of a total of 18 activities, and each activity is divided into 7 levels. Level 1 indicates full assistance; level 7 indicates complete independence. A score of 36 and below is considered high disability, 37–72 points moderate disability, and 73 and above low disability (Küçükdeveci et al. 2001). In the Turkish validity and reliability study conducted by Küçükdeveci and colleagues in 2001, the Cronbach’s alpha value was greater than 0.70 and considered significant (Küçükdeveci et al. 2001; Yavuzer 1996).
Bristol Stool ScaleThis is developed by Lewis and Heaton at the University of Bristol, UK (Lewis and Heaton 1997). In the seven-type stool classification, types 1 and 2 represent constipation, 3 and 4 represent normal stool, and 5, 6, and 7 represent diarrhea (Bristol stool chart 2024).
Gastrointestinal Symptom Rating Scale (GSRS)Developed by Revicki et al. in 1998 (Revicki et al. 1998). The scale consists of 15 items, each scored on a 7-point Likert-type scale ranging from “no discomfort” to “very severe discomfort.” Based on factor analysis, the 15 items of the GSRS are divided into five subscales: reflux, abdominal pain, indigestion, diarrhea, and constipation. Higher scores on the scale indicate more severe symptoms. The Turkish validity and reliability study of the scale was conducted by Turan, Aştı, and Kaya in 2017, and the Cronbach’s alpha value was found to be 0.82 (Turan et al. 2017). In this study, the Cronbach’s alpha value was 0.71.
General Comfort Scale (GCS)Comfort theory, developed by Kolcaba in 1992, is based on a taxonomic structure with three levels and four dimensions. The scale subdimensions are relief (17 items), ease (16 items), and transcendence (15 items). In addition, it is related to the dimensions of physical comfort (12 items), environmental comfort (13 items), sociocultural comfort (10 items), and psychospiritual comfort (13 items). There are 48 items in the GCS, which are evaluated with a 4-point Likert scale. The higher the score obtained from the scale, the higher the comfort level perceived by the patient (Comfort 2003; Kuğuoğlu and Karabacak 2008). The Turkish validity and reliability studies of the scale were conducted by Kuğuoğlu and Karabacak in 2008, and the Cronbach’s alpha value was 0.83 (Kuğuoğlu and Karabacak 2008). In this study, the Cronbach’s alpha value was 0.83.
ProcedureThe investigators informed volunteer patients who could not defecate for 3 days after surgical intervention and met the other sampling criteria concerning the study’s purpose, content, and method. Written and verbal consent was obtained from the patients assigned to the experimental and control groups by randomization.
The Patient Information Form, Functional Independence Measure, Gastrointestinal Symptom Rating Scale, and General Comfort Scale were applied to the patients in the experimental group at the first encounter (after surgery on the fourth day). No pharmacologic agent was administered to the patients in the experimental group, and abdominal massage was performed twice a day for 15 min each in the morning and evening for 3 days starting from the morning of the first day. The Abdominal Massage Practice Guidelines developed by Uysal, Eşer, and Akpınar in 2012 were used during abdominal massage (Uysal et al. 2012). The four main techniques used in the massage application were as follows: superficial effleurage, deep effleurage, petrissage, and vibration. Abdominal massage is applied in the natural flow direction of the intestine, that is, clockwise.
To ensure standardization, the same researcher trained in the guideline-based technique administered all abdominal massage sessions. Each session was delivered under the same environmental conditions (e.g., time of day, room privacy, post-meal timing), and the duration and method of application were kept consistent across all patients. In addition, to ensure that the patients were sufficiently relaxed during the abdominal massage, care was taken to ensure that the relatives were not present in the room; the curtain/screen on the bed was closed; there was no need for urinary excretion; the room was calm, at an appropriate temperature and dim light according to preference; and it was applied 30 min after meals.
After each massage application (twice a day in the morning and evening for 3 days), the researcher used a stethoscope to record bowel sounds/movements in each quadrant. The investigator evaluated and recorded the patients’ defecation during this period via the Bristol Stool Scale. At the end of the 3-day follow-up, the investigator administered the Gastrointestinal Symptom Rating Scale and General Comfort Scale to both groups (after surgery on the 6th day) (Fig. 2).
Fig. 2
At the first encounter, patients in the control group were administered the patient information form, Functional Independence Measure, Gastrointestinal Symptom Rating Scale, and General Comfort Scale (after surgery on the 4th day). Patients in the control group received pharmacological treatment such as enema and laxatives according to the physician’s instructions, starting from the morning of the first day, when necessary, and following the clinical routine. During the 3-day follow-up period, bowel sounds/movements in each quadrant were auscultated and recorded by the researcher via a stethoscope twice daily in the morning and evening. The defecation of the patients who defecated during this period was evaluated and recorded by the investigator via the Bristol Stool Scale (Fig. 2). At the end of the 3-day follow-up, the Gastrointestinal Symptom Rating Scale and General Comfort Scale were administered to the experimental and control groups (after surgery on the 6th day) (Fig. 2).
Several precautions were taken to minimize the risk of observer bias since the same researcher performed both the intervention and data collection. Before the study, the researcher was trained in the abdominal massage technique and standardized data collection procedures. To ensure fidelity and consistency, all massage sessions were guided by a structured checklist based on the abdominal massage guideline. Furthermore, data analysis was conducted by an independent statistician blinded to group allocation.
Statistical analysisThe SPSS (IBM SPSS Statistics 27) package was used for statistical data analysis. Descriptive statistical methods (frequency, percentage, mean, and standard deviation) were applied. Parametric methods were used to measure values suitable for a normal distribution, the independent sample t-test was used to compare the measurement values of two independent groups, and the paired sample test method was used to compare two dependent groups. For nonnormally distributed measurement values, the Mann‒Whitney U-test was used to compare the measurement values of two independent groups, the Wilcoxon test was used to compare two dependent groups, the Pearson chi-square test was used to compare qualitative data, and the Spearman correlation coefficient was used to examine the relationships between two normally distributed quantitative variables. The findings were evaluated at the 95% confidence interval and 5% significance level.
Comments (0)