
Remember me
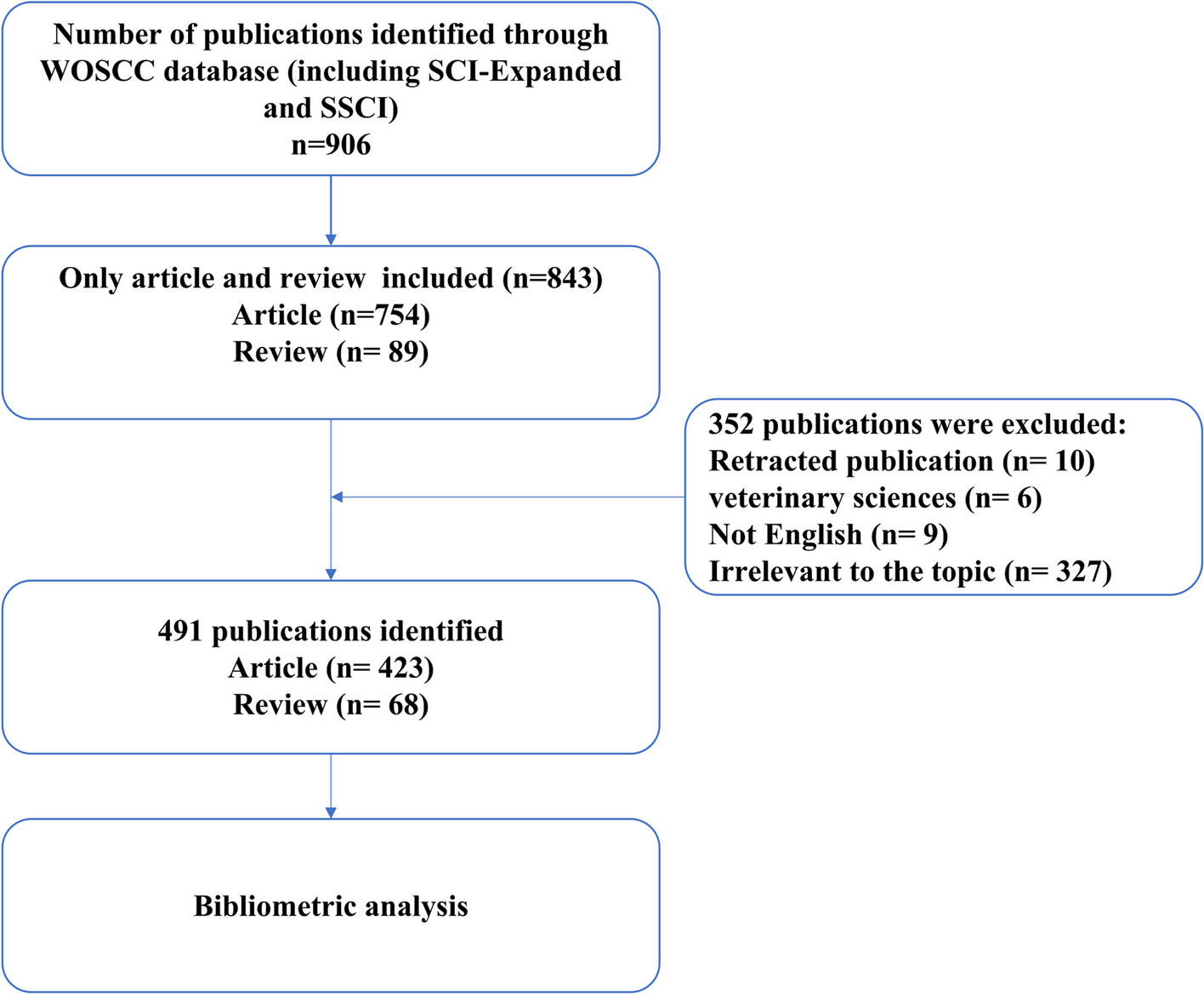
In our study, a bibliometric analysis was used to ascertain the current status of AI in anesthesiology, including publication output, leading countries, preferred journals, top institutions, and clustered keywords. In summary, 491 papers from 48 countries, 715 institutions, and 218 journals were included in this article. The rapid increase number of papers since 2018 suggests that the study of AI in anesthesiology is attracting increasing interest. In terms of co-citation of literature, a significant amount of research was observed for the prediction of hypotension, marking it as a hot frontier issue. Through the keyword co-occurrence cluster analysis, the keywords could be categorized into four distinct clusters, including machine learning for ultrasound-guided regional anesthesia, prediction model, artificial neuronal network of DoA, and close-loop control of anesthesia (Fig. 8).
Fig. 8
Application of AI in anesthesiology
Hotspots and frontiers of AI in anesthesiologyResearch on AI in ultrasound-guided regional anesthesiaAI has been shown to have advantages in image recognition. Current research focuses on the use of deep neural networks for the identification of anatomical structures and needle positioning (Yang et al. 2022) (Mwikirize et al. 2021). New type of intelligent ultrasound device, such as the ScanNav Anatomy Peripheral Nerve Block, has already been proved by US FDA to help anesthetists and other health professionals identify anatomical structures in ultrasound images in 2022 (Bowness et al. 2022). The device uses deep learning technology to create color overlays of key anatomical structures on live ultrasound images. The device was first reported by Bowness and his team in 2022. The author explored its utility, which showed that ScanNav had potential to support nonexperts in training and clinical practice and experts in teaching ultrasound-guided regional anesthesia. Furthermore, the same team published two more studies in 2023. One study compared the accuracy of key anatomical structures of 720 videos acquired with or without the device (Bowness et al. 2023a), and the other evaluated ultrasound scanning performance by nonexperts (Bowness et al. 2023b). The first study found that the false-negative rate and false-positive rate of the device were 3.0% and 3.5%, respectively, and the risk of unwanted needle trauma and block failure were also judged to be reduced. The second study showed that use of AI device was associated with improved ultrasound image acquisition and interpretation for nonexperts. Nerveblox is another AI-driven decision support solution to help anesthesiologists practice peripheral nerve block faster, which could capture the real-time images from any ultrasonography device and label key anatomical landmarks on the images (Gungor et al. 2021). However, Nerveblox has not yet been approved for use on patients in the USA. Both Nerveblox and ScanNav Anatomy Peripheral Nerve Block could support the identification of some superficial peripheral nerves: interscalene/supraclavicular/infraclavicular brachial plexus, femoral nerve, saphenous nerve, popliteal sciatic nerve, erector spinae plane, and rectus sheath. Artificial neural network and machine learning have been used to automatically identify paravertebral or epidural anatomical structures and assist needle positioning, but they have not yet been applied to clinical practice (Zhao et al. 2023) (Pesteie et al. 2018). Further studies are necessary for AI to identify anatomy related to deep block such as subgluteal sciatic nerve block and improve the ability in visualizing the needle tip when the angle of penetration is acute (Viderman, et al. 2022). AI in ultrasound-guided regional anesthesia is still in its infancy and has a long way to go before it is widely used.
Research on AI in postoperative pain managementCurrently, the assessment of pain is predominantly based on subjective descriptions or vital signs, without objective indicators, which may result in a degree of bias. AI is currently being explored to identify objective indicators of pain. During general anesthesia, the analgesia nociception index is used to assess pain levels, guiding the administration of opioids (Gonzalez-Cava et al. 2020). For the assessment of postoperative pain, researchers developed a novel analgesic index, namely spectrogram–convolutional neural network index, by combining photoplethysmogram spectrograms and a convolutional neural network (Choi et al. 2021). For the assessment of postoperative pain in children after cardiac surgery, studies had proposed using machine learning to understand pain behavioral responses based on facial expressions, body or head movements, and voice signal analysis (Pollak, et al. 2019). Preoperatively, AI was used to select patients who might benefit from preoperative pain consultation (Tighe, et al. 2012). In addition to pain assessment, AI can collect patients’ vital signs and pain data and predict the demand for analgesics after surgery through machine learning and deep learning analysis, making real-time adjustments and truly achieving dynamic, personalized preventive analgesia (Wang et al. 2020). In summary, AI may be used for pain assessment before, during, and after surgery and guiding treatment of postoperative pain. This might provide a closed loop of perioperative pain control.
Research on AI in airway managementResearch on AI in airway management primarily focus on identifying airway structures, predicting difficult airways, and predicting the size and depth of tracheal tube intubation (Kim et al. 2023). Convolutional neural networks can recognize the vocal cords and tracheal rings in real time during video laryngoscopy (Matava et al. 2020). Deep learning aids in the development of automatic navigation systems to guide nasal tracheal intubation (Deng 2023). Deep learning was used to link patient facial images to the actual difficulty of intubation to establish a model for identifying difficult intubations (Hayasaka et al. 2021; Tavolara et al. 2021; Connor and Segal 2011). The accuracy of automated Mallampati classification was improved by deep convolutional neural networks, which can help clinicians objectively and accurately classify difficult airways (Zhang et al. 2022). Currently, many models have been established, but there is still no rapid and accurate device for identifying difficult airways in clinical practice. It remains to be verified whether the same model can be applied between different races.
Research on AI in prediction modelAI was utilized in the establishment of prediction models, including the prediction of hypotension, acute kidney injury, delirium, myocardial injury, transfusion, hypoxemia, and mortality (Fritz et al. 2019; Chen et al. 2022; Bishara et al. 2022). With these advanced predictive models, healthcare professionals can identify risks more accurately, optimize treatment plans, and improve patient outcomes and quality of life. The first to be applied in the operating room was the hypotension prediction index, a machine learning algorithm that predicts hypotensive events through high-fidelity analysis of pulse-wave contours (Hatib et al. 2018). Studies have validated the hypotension prediction index and found that it could reduce intraoperative hypotension compared with standard care (Wijnberge et al. 2020). However, the algorithm of hypotension prediction index was considered as a “black box,” which cannot indicate the causes of hypotension, necessitating further standardization and improvement, which needed further standardization and improvement (Ven et al. 2021).
Research on AI in DoA monitoringWith the advancement of AI, the processing of complex electroencephalogram (EEG) signals has become easier, and the number of related studies is increasing (Chen, et al. 2022), which has injected new vitality into the monitoring of the DoA. For example, a new index for accurately predicting DoA based on EEG signals, known as EEGMAC, was proposed by combining deep learning techniques. This index was applicable to patients under volatile and intravenous anesthesia and was found to be more effective than the bispectral index (Park et al. 2020). In addition, several studies have combined AI with auditory-evoked potentials to monitor DoA (Elkfafi, et al. 1998; Lu et al. 1999; Allen and Smith 2001). However, further validation is needed to determine which indicator is more sensitive to depth of anesthesia. With the development of AI, DoA monitoring has become more diversified and popularized, which will inevitably lead to new developments in closed-loop drug infusion for anesthetics.
Research on AI in perioperative drug infusionWith the development of technology, infusion pumps have evolved from constant-rate infusion to target-controlled infusion and closed-loop infusion systems. A comprehensive closed-loop infusion system during surgery requires an accurate and comprehensive monitoring and feedback system, including the DoA (sedation, analgesia, muscle relaxation), hemodynamics (SpO2, ECG, blood pressure), respiratory dynamics, and body temperature, among others (Ghita et al. 2020). Current research on closed-loop systems is limited to smaller scopes, such as closed-loop fluid and vasoactive drug management, DoA, muscle relaxation, and blood glucose control (Coeckelenbergh, et al. 2050; Fields et al. 2008). There is still a significant journey ahead to achieve full closed-loop management throughout the entire surgical procedure. Of course, anesthesiologist continue to be the most critical role in intraoperative management. Closed-loop infusion is merely a tool, with the ultimate decision-making authority resting in the hands of the anesthesiologist.
Limitations and concerns of AIResearches on AI in the field of anesthesiology is actively ongoing, but its limitations are also becoming increasingly apparent. Firstly, AI analyzes results from existing large volumes of data, which relies on the authenticity and accuracy of the data. However, the accuracy of the data is difficult to assess, necessitating the establishment of regulatory bodies. Obtaining large datasets is relatively challenging, requiring significant human resources, financial investment, and collaboration among multiple institutions (Kelly et al. 2019). Currently, the datasets used to train AI often come from specific populations and may only be applicable to certain groups of people (Maheshwari, et al. 2023). Secondly, the algorithms of deep learning are opaque, and it is not possible to analyze the reasons leading to the results, which leads to skepticism among physicians regarding the outcomes derived from deep learning (Hashimoto et al. 2020). Additionally, there is concern that advancements in AI might lead to the deterioration of clinical doctors’ skills (Maheshwari, et al. 2023). Lastly, the issue of accountability when AI-generated conclusions adversely affect patients is a matter that needs consideration (Solanki, et al. 2021). Clinical anesthesia deals with patients who exhibit individual differences, and the formulation of medical decisions is intricate and complex, unlike chess, which has clear rules. Often, decisions must be based on a comprehensive analysis of the clinical situation. Therefore, the focus of future AI research should not be to replace the judgment or skills of clinical doctors but to optimize their methods and increase the transparency of algorithms (Hashimoto et al. 2020).
LimitationsThis study was the first to use bibliometric visualization to analyze research on AI in anesthesiology. However, this study had several limitations. First, the search was limited to the Web of Science and did not include relevant literature from other databases, which might have resulted in an incomplete search. Second, this study included only English-language literature, which might have led to biased results. Third, the use of different names for the same institution at different times can lead to inaccuracies in the number of documents. Fourth, this paper only uses two software, VOSviewer and CiteSpace, and does not use others, such as the bibliometric online platform and R software, which reduces multiple verification. Fifth, this paper gives a brief overview of the research of AI in anesthesiology, in order to understand the application of AI in specific fields (such as airway management, pain management), and more in-depth literature reading is needed.
Comments (0)