
Remember me
A total of 22,972 patients met inclusion criteria and were included in the final analysis (Table 1). The cohort comprised 12,061 (52.5%) male patients with a mean age of 58.7 ± 16.2 years. The majority of procedures were non-cardiac surgeries (n = 20,444, 89.0%), with cardiothoracic surgery accounting for 2528 cases (11.0%).
Table 1 Amino acid utilization by surgical departmentOverall, 899 patients (3.9%) received perioperative amino acid preparations. Among amino acid users, some patients received multiple preparation types concurrently. The distribution of amino acid preparations was: parenteral nutrition solutions containing amino acids (B05BA10, n = 723), fat emulsions containing amino acids (B05BA02, n = 145), and pure amino acid solutions (B05BA01, n = 89). The total exceeds 899 due to patients receiving multiple preparation types.
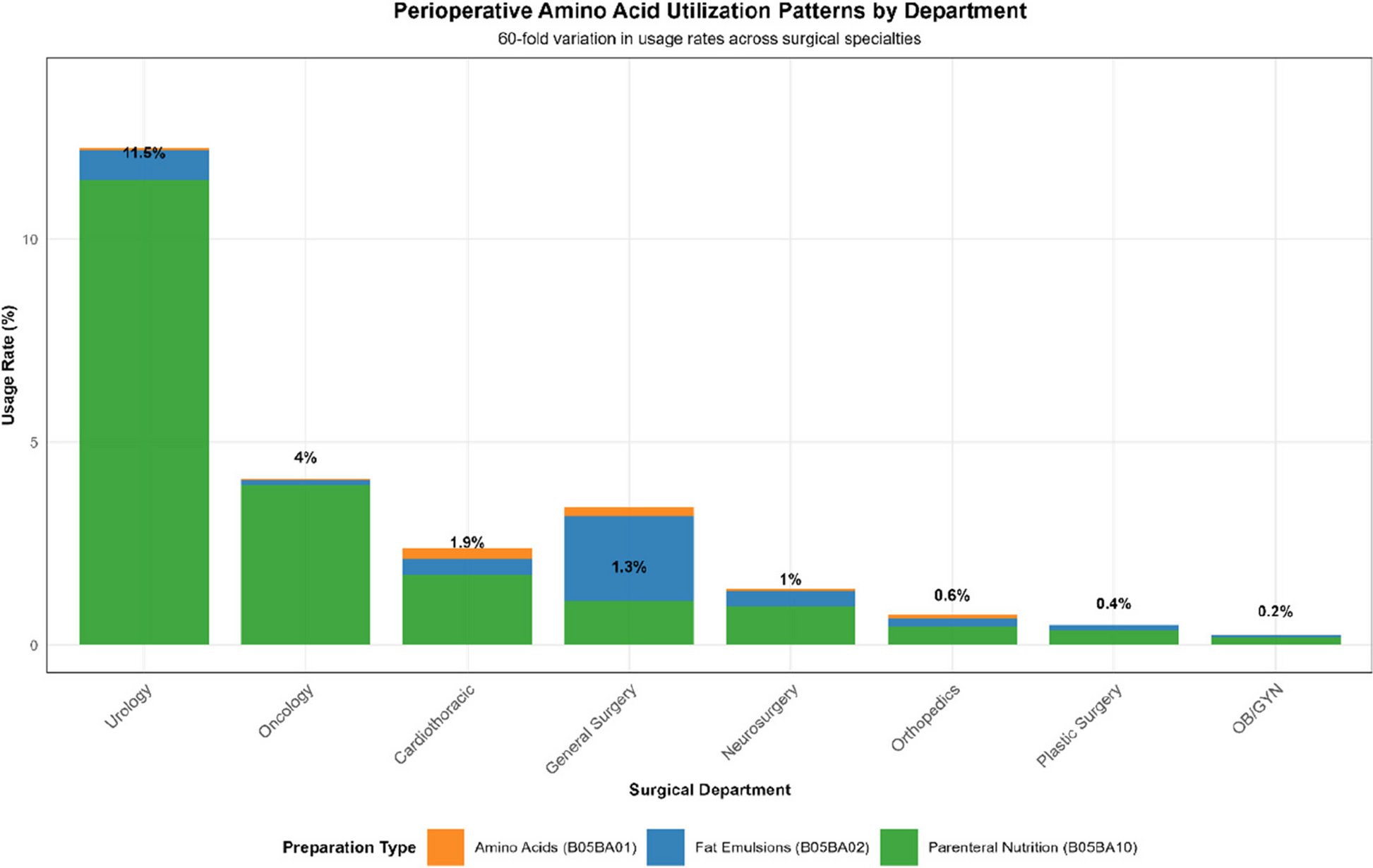
Amino acid utilization patterns across surgical departmentsAmino acid utilization demonstrated remarkable variation across surgical departments, ranging from 0.2% in obstetrics/gynecology to 11.5% in urology—a 60-fold difference (Fig. 1). The highest utilization rates were observed in urology: 11.5% (n = 885/7692), oncology: 8.2% (n = 197/2404), general surgery: 4.1% (n = 423/10,345), cardiothoracic surgery: 2.0% (n = 50/2528). The lowest utilization was found in obstetrics/gynecology: 0.2% (n = 26/12,946), plastic surgery: 0.4% (n = 21/5157).
Fig. 1
Perioperative amino acid utilization patterns by department. Stacked bar chart displaying perioperative amino acid utilization rates across eight surgical departments, demonstrating remarkable variation in practice patterns. Utilization rates range from 0.2% in obstetrics/gynecology (OB/GYN) to 11.5% in urology, representing approximately a 60-fold difference in usage patterns. Each bar shows the total utilization rate with a breakdown by preparation type: amino acids (B05BA01, orange), fat emulsions (B05BA02, blue), and parenteral nutrition (B05BA10, green). The highest utilization rates were observed in urology (11.5%), followed by oncology (4%), cardiothoracic surgery (1.9% with additional 1.3% for different preparations), general surgery (1.3%), neurosurgery (1%), orthopedics (0.6%), plastic surgery (0.4%), and obstetrics/gynecology (0.2%). Parenteral nutrition solutions (green) comprised the majority of amino acid preparations across most departments. This substantial variation likely reflects differences in patient complexity, procedure duration, departmental nutritional support protocols, and practice culture, highlighting significant opportunities for evidence-based standardization
Parenteral nutrition solutions (B05BA10) comprised the majority of amino acid use across all departments, accounting for > 80% of administrations in most specialties. This utilization pattern appeared to correlate with patient complexity, procedure duration, and departmental practices regarding nutritional support.
Primary outcomes: AKI incidenceAcross the entire cohort, 840 of 22,972 patients (3.7%) developed AKI within 72 h. AKI rates varied significantly across surgical departments: cardiothoracic surgery: 4.1% (103/2528), general surgery: 4.2% (434/10,345), urology: 3.8% (293/7692), obstetrics/gynecology: 0.8% (103/12,946), plastic surgery: 1.2% (62/5157).
In univariable analysis, amino acid administration was associated with significantly increased AKI risk (OR = 2.06, 95% CI 1.58–2.68, p < 0.001). However, this overall association masked important surgery-specific differences that emerged upon stratified analysis.
Surgery-specific analysis: the core findingThe most clinically significant finding was the striking differential association between amino acid administration and AKI risk across surgical contexts, revealing fundamentally opposite patterns between cardiac and non-cardiac surgery populations (Fig. 2).
Fig. 2
Surgery-specific patterns of amino acid use and AKI risk. Bar chart comparing acute kidney injury (AKI) incidence between amino acid users and non-users, stratified by surgical type (cardiac vs non-cardiac surgery). The chart demonstrates contrasting patterns with error bars representing 95% confidence intervals. In cardiac surgery (green bars), amino acid non-users had 4.2% AKI rate (103/2478 patients) while amino acid users had 0% AKI rate (0/50 patients, p = 0.267), suggesting a protective trend despite not reaching statistical significance. In non-cardiac surgery (red bars), the pattern reverses: non-users had 3.4% AKI rate (674/19,595 patients) while users had significantly higher AKI rates at 7.4% (63/849 patients), yielding a risk ratio of 2.16 (p < 0.001). This differential association across surgical contexts illustrates surgery-specific effects and highlights the critical importance of surgical context in amino acid administration decisions and AKI risk assessment
Cardiac surgery populationAmong 2528 cardiac surgery patients, 50 (2.0%) received perioperative amino acid preparations. Remarkably, no AKI events occurred in any amino acid recipients (0/50, 0%) compared to 103/2478 (4.2%) in non-recipients (p = 0.267, Fisher’s exact test). While statistical significance was not reached due to the small number of amino acid users and the zero-event phenomenon, this finding represents a strong protective trend entirely consistent with recent randomized controlled trials demonstrating renoprotective effects of amino acid infusion in cardiac surgery patients.
This protective pattern likely reflects the prophylactic use of amino acids in cardiac surgery, where emerging evidence supports their administration for renal protection during the high-risk perioperative period. The physiological stress of cardiopulmonary bypass, with associated renal hypoperfusion, ischemia–reperfusion injury, and systemic inflammatory response, may create an optimal pathophysiological context for amino acid-mediated renoprotection through enhanced renal blood flow and metabolic support.
Non-cardiac surgery populationIn contrast to the cardiac-surgery group, the non-cardiac cohort showed a markedly different pattern. Among 20,444 non-cardiac surgery patients, 849 (4.2%) received amino acid preparations. Amino acid use was associated with significantly higher AKI rates: 63/849 (7.4%) in users versus 674/19,595 (3.4%) in non-users, yielding a risk ratio of 2.16 (95% CI 1.68–2.77, p < 0.001).
This increased risk association in non-cardiac surgery likely reflects confounding by indication, where amino acid administration serves primarily as nutritional therapy for patients with poor baseline nutritional status, prolonged or complicated procedures, or significant comorbidities. In this context, amino acid use functions as a marker for patient severity and complexity rather than as a prophylactic intervention, explaining the observed association with increased AKI risk.
This differential pattern suggests fundamentally different clinical contexts and indications for amino acid administration between surgical populations.
Propensity-score-matched analysisTable 2 summarizes baseline characteristics before and after 1:1 propensity-score matching (caliper 0.2 SD). Following matching, all standardized mean differences were < 0.08, indicating excellent balance. Among the 799 matched pairs, AKI occurred in 54 amino-acid recipients (6.8%) versus 34 controls (4.3%), yielding an odds ratio of 1.63 (95% CI 1.05–2.52, p = 0.029).
Table 2 Baseline characteristics and AKI incidence before and after propensity-score matching (n = 799 pairs)Multivariable analysisAfter multivariable adjustment for age, sex, surgical category, and procedure duration, amino acid administration remained independently associated with increased AKI risk when analyzed across all patients (adjusted OR = 2.01, 95% CI 1.52–2.60, p < 0.001) (Fig. 3). Independent predictors of AKI included amino acid use: OR = 2.01 (95% CI 1.52–2.60, p < 0.001), male sex: OR = 1.58 (95% CI 1.37–1.83, p < 0.001), age per year: OR = 1.02 (95% CI 1.01–1.03, p < 0.001), procedure duration per hour: OR = 1.01 (95% CI 0.97–1.05, p = 0.545).
Fig. 3
Multivariable analysis of risk factors for postoperative AKI. Forest plot displaying adjusted odds ratios (OR) and 95% confidence intervals from multivariable logistic regression analysis predicting postoperative acute kidney injury. The vertical dashed red line at OR = 1.0 represents no association. Variables are ordered by statistical significance and effect magnitude. Amino acid use shows the strongest association with increased AKI risk (OR = 2.01, 95% CI 1.52–2.6, p < 0.001), followed by male sex (OR = 1.58, 95% CI 1.37–1.83, p < 0.001), baseline creatinine (OR = 1.35, 95% CI 1.15–1.58, p < 0.001), and age per year (OR = 1.02, 95% CI 1.01–1.03, p < 0.001). Surgery duration per hour showed no significant association (OR = 1.01, 95% CI 0.97–1.05, p = 0.545). The analysis demonstrates that amino acid administration remains the strongest independent predictor of AKI risk after adjustment for demographic, clinical, and procedural factors
Machine learning model performance and feature analysisAmong the four machine learning models tested, random forest achieved the highest predictive performance with an AUC-ROC of 0.782 (95% CI 0.756–0.808), followed by gradient boosting [0.775 (95% CI 0.749–0.801)], support vector machine [0.758 (95% CI 0.730–0.786)], and logistic regression [0.721 (95% CI 0.693–0.749)] (Fig. 4).
Fig. 4
Machine Learning Model Performance Comparison
Feature importance analysis across all models consistently identified amino acid administration as the most influential predictor of AKI risk. Notably, the Random Forest model revealed significant non-linear interactions between amino acid use and surgical type, confirming our stratified analysis findings through an alternative analytical approach.
Partial dependence plots demonstrated that the protective effect of amino acids was most pronounced in cardiac surgery patients, while the risk association increased progressively in non-cardiac surgery populations. This non-linear relationship supports our hypothesis that surgical context fundamentally modifies the amino acid–AKI relationship, with threshold effects that cannot be captured by traditional linear modeling.
The consistency of findings across traditional regression, machine learning, and propensity score approaches strengthens the evidence for surgery-specific amino acid effects and suggests that our observed patterns reflect genuine clinical phenomena rather than methodological artifacts.
Subgroup analysesSurgery-stratified subgroup analyses confirmed the differential patterns:
Non-cardiac surgery subgroups: age ≥ 65 years: OR = 1.90 (95% CI 1.20–3.00, p = 0.015), age < 65 years: OR = 2.30 (95% CI 1.60–3.20, p < 0.001), male sex: OR = 2.40 (95% CI 1.70–3.30, p < 0.001), female sex: OR = 1.70 (95% CI 1.10–2.70, p = 0.019).
Sensitivity analyses excluding emergency procedures, extreme age groups, and procedures lasting > 12 h yielded consistent results (OR = 2.08, 95% CI 1.55–2.78, p < 0.001 for non-cardiac surgery).
Clinical risk stratification frameworkBased on our findings, we developed a clinical risk stratification framework that enables personalized perioperative care (Fig. 5):
Fig. 5
Clinical Risk Stratification Framework Based on Surgery Type and Amino Acid Use
Risk categories:
1.Lowest risk: cardiac surgery with amino acids—0% AKI rate (n = 50)
2.Low risk: cardiac surgery without amino acids—4.2% AKI rate (n = 2478)
3.Moderate risk: non-cardiac surgery without amino acids—3.4% AKI rate (n = 19,595)
4.Highest risk: non-cardiac surgery with amino acids—7.4% AKI rate (n = 849)
This stratification framework ranges from lowest risk (0% AKI) to highest risk (7.4% AKI), representing clinically meaningful differences that can inform monitoring intensity, prophylactic interventions, and patient counseling strategies.
The identification of these distinct risk categories has immediate practical implications for perioperative care planning and resource allocation.
Comments (0)