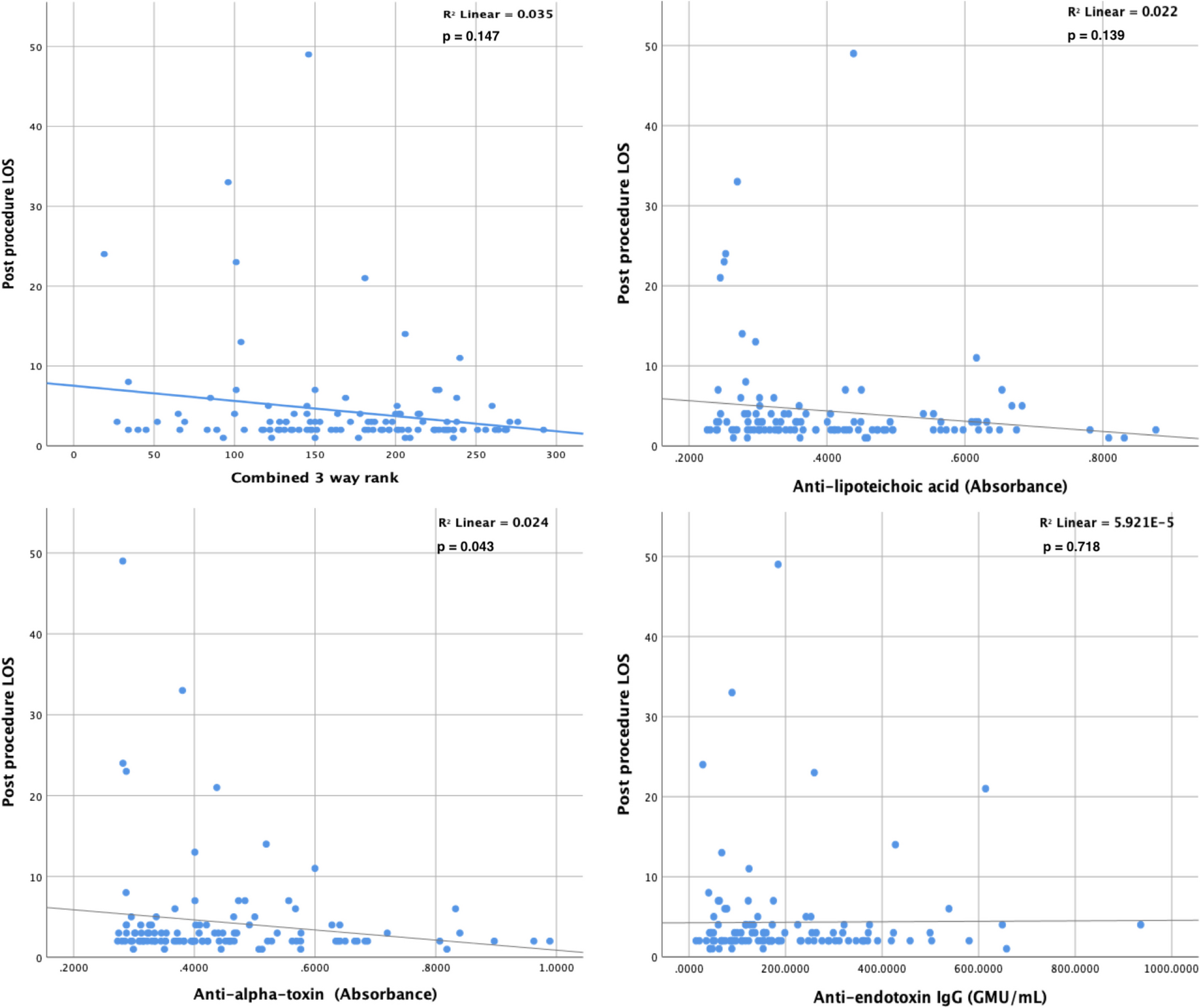
The results from this study indicate that there is little association between post-procedural length of stay in hospital following TAVI and pre-procedural antibody levels to endotoxin or staphylococcus.
Furthermore, when a composite measure of antibody level using a combined ranked score for antibody levels is used, as described in previous work (Horan et al. 2008), there is no significant correlation between antibody levels and length of stay following TAVI.
The likelihood of developing a post-procedural infection did not appear to be correlated with antibody levels to endotoxin or staphylococcus, in contrast to the findings in patients undergoing open surgical aortic valve replacement (Horan et al. 2008).
Examination of the quartiled results, as described in previous studies on patients undergoing open cardiac surgery (Granstrom et al. 1983; Hamilton-Davies et al. 1997; Horan et al. 2008), indicates no differences in the median length of stay between all four quartiles, for any of the antibody assays or for the combined rank sum grouping.
The median length of stay of the Q4 group is lower than that for the Q1 group when analysed for staphylococcal antibodies; however, only the teichoic acid component reaches statistical significance. Patients divided into quartiles according to anti-endotoxin antibody titre have no differences in length of stay.
Any potential difference between Q1 and Q4 for the rank sum group appears to be driven by the antibodies directed at gram-positive epitopes (alpha-toxin and teichoic acid).
We have previously described the relationship being specific to the antigenic threat (Horan et al. 2008), and it would be reasonable to consider that the exposure to endotoxin during the TAVI procedure would be markedly reduced when compared to the exposure during cardiopulmonary bypass in open cardiac surgery. This idea is supported by the lack of association of outcome with pre-operative EndoCAb levels. The difference in endotoxin levels measured in patients undergoing open surgery and TAVI has been described by Adrie et al. (Scully et al. 2020).
The reduced association of length of stay with staphylococcal antibodies supports the reduced risk of staphylococcal exposure afforded to patients undergoing TAVI when compared to the large incision of a sternotomy from a surgical AVR. Importantly, those with an impaired ability to mount an adequate immune response may be avoiding the important antigenic challenges of endotoxaemia and staphylococcal antibody exposure. Any association between staphylococcal antibody titre levels is likely due to some, albeit limited, exposure to organisms during skin punctures for catheter placement.
Patients undergoing TAVI are generally older with a relatively high ‘surgical risk’ yet do not seem to suffer the same level of infective complications as those patients undergoing open surgical AVR.
Recent work by Kimura et al. has demonstrated the lower levels of inflammatory cytokines released following TAVI when compared to surgical AVR (Sharabiani et al. 2016). It has also been demonstrated that the circulating levels of endotoxin, peptidoglycans, and proinflammatory cytokines were lower in TAVI patients when compared to those having undergone standard surgical AVR (Scully et al. 2020).
Our results are consistent with these findings of a reduced inflammatory and immunological response in those undergoing percutaneous approach to AVR. There is significantly less tissue trauma with the percutaneous approach with much smaller incisions. It is intuitive that the exposure to staphylococcus would be less in the percutaneous approach. The avoidance of CPB results in less haemodynamic disturbance with less gastro-intestinal hypo-perfusion and subsequent endotoxin leak into the circulation. Less exposure to staphylococcal or endotoxin antigen results in a lesser challenge to the immune system.
Unlike those undergoing surgical aortic valve replacement, patients with diminished pre-operative immune status (low pre-existing antibody levels) undergoing TAVI appear to be at a lower risk of increased length of stay or post-procedure infection.
This raises a number of considerations. Based on previous work, those subjects with low levels of antibody may be expected to have a prolonged stay if they had undergone surgery rather than TAVI. We presume this to be in some way related to the ability to mount an adequate immune response to the particular antigenic challenge encountered. Low antibody levels to an antigen imply either the absence of recent exposure to that antigen or failure to mount an adequate immune response; the population with low antibody levels are likely to contain a proportion of subjects with inadequate immune responsiveness. Currently, there is no simple test available to identify this proportion.
If those people referred for AVR who have coexistent immune impairment can be identified, then TAVI may offer a lower risk option than a surgical approach.
In addition to the problems relating to endotoxin and gram-negative organisms, staphylococcal wound infection complicates approximately 3–4% of cardiac procedures (Smith et al. 2018). A large study carried out in the United States on over 8000 patients undergoing cardiopulmonary bypass surgery found an overall mortality rate of 4% compared with over 17% for those developing post-operative methicillin-resistantStaphylococcus aureus(MRSA) (Soderquist et al. 1993). The economic implications of cardiac surgical patients developing staphylococcal bacteraemia is great with a demonstrated threefold increase in cost for the group developing infectious complications (Auensen et al. 2017; Swank et al. 1996).
The protective effect of antibodies to these antigenic challenges may not be surprising, yet the underlying immunity of the pre-operative patient is not routinely explored and is not incorporated in standard risk assessment algorithms.
The large breach in the skin integrity necessitated by open cardiac surgical procedures, often involving cardiopulmonary bypass, will leave the patients at a significant risk of staphylococcal exposure. Patients with impaired immune function, as evidenced by low antibody levels, may be less capable of withstanding this stress and, therefore, be more prone to perioperative complications.

Comments (0)