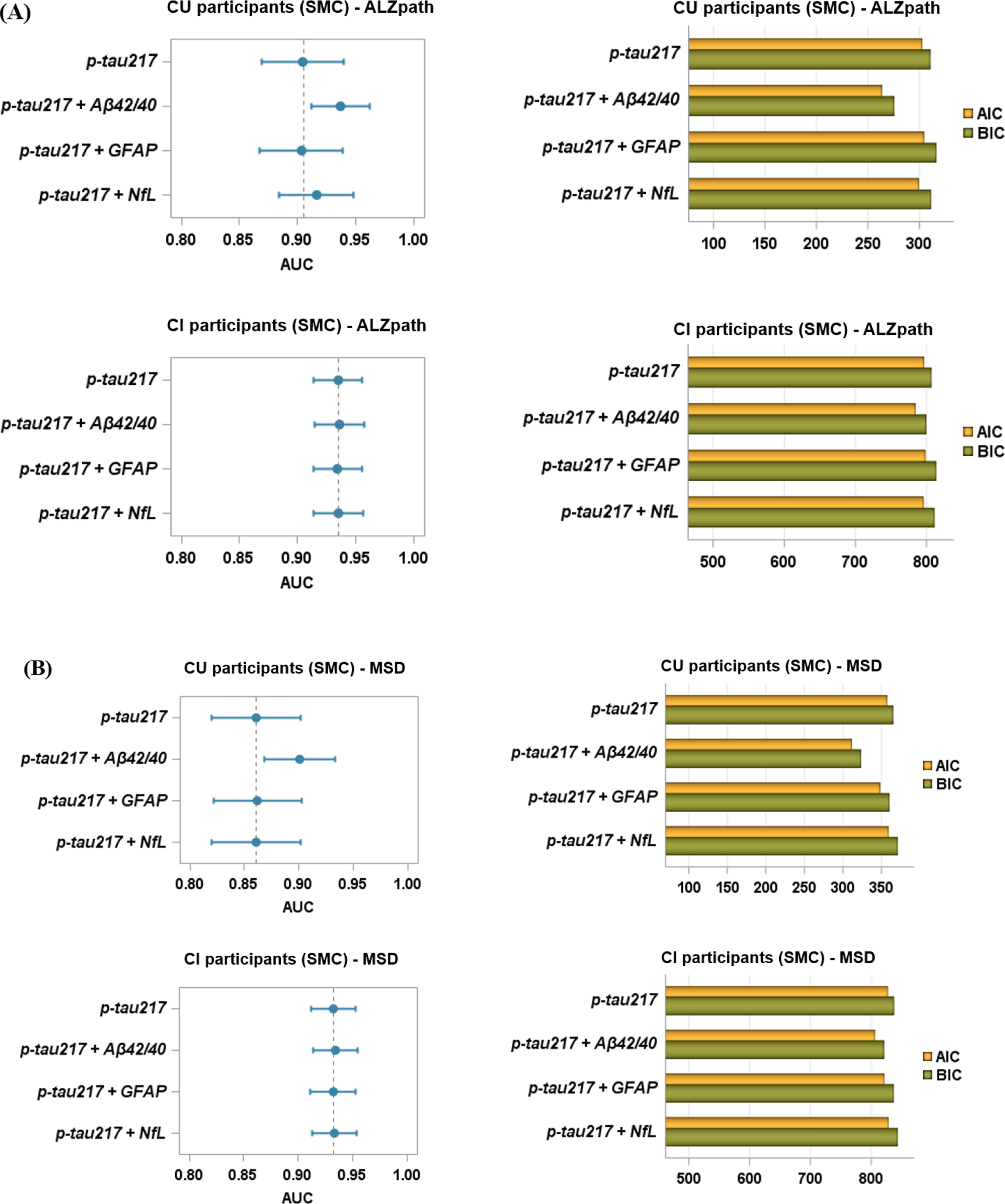
We assessed the diagnostic performance and model fit of plasma biomarkers in CU and CI individuals using SIMOA and MSD assays, with model development at SMC and validation in an independent cohort. Our major findings were as follows. First, in CU individuals, the combined plasma p-tau217 and Aβ42/40 model significantly improved diagnostic accuracy and model fit compared to p-tau217 alone, whereas in CI, it provided only modest model fit improvements without enhancing AUC. These findings were consistent across both the SIMOA and MSD assays, and the amyloid probability score was validated in an independent cohort, supporting its robustness and cross-site applicability. In contrast, adding GFAP or NfL did not improve diagnostic performance or model fit in either group. Finally, within CU subgroups stratified by age, sex, APOE4 status, and obesity, the combined model enhanced diagnostic performance in older individuals, females, and APOE4 non-carriers. These findings were observed in both obese and non-obese participants and were consistent across both the SIMOA and MSD assays. Taken together, these findings suggest that the combined plasma p-tau217 and Aβ42/40 model improves predictive performance in specific CU subgroups, while offering only modest benefits in CI individuals. These results underscore the clinical potential of integrated plasma biomarker strategies for enhancing early diagnosis and individualized risk assessment of AD.
Our primary finding was that in CU individuals, the combined plasma p-tau217 and Aβ42/40 model significantly improved diagnostic accuracy and model fit compared to p-tau217 alone, whereas in CI individuals it provided only modest improvements in model fit without enhancing AUC. This difference in effectiveness likely stems from the distinct pathological profiles of these groups. Specifically, CI individuals exhibit a greater enrichment of tau pathology than CU individuals. Although p-tau217 is associated with both Aβ and tau, its relationship in CU individuals is predominantly with amyloid, whereas in CI individuals—where tau pathology is more enriched—it is more closely linked to tau uptake. Consequently, in CI individuals, p-tau217 alone is highly accurate in identifying amyloid-positive cases, rendering the added value of Aβ42/40 minimal. In contrast, in CU individuals the sensitivity of p-tau217 for detecting early Aβ accumulation may be limited; since Aβ42/40 reflects soluble Aβ species that decline prior to Aβ PET positivity, incorporating it into the model likely enhances early Aβ detection.
We identified the optimal AP cutoffs were higher in CI than CU individuals, which aligns with our prior findings showing that p-tau217 levels are influenced predominantly by amyloid pathology in CU, and by both amyloid and tau pathology in CI [45]. This highlights the potential need for subgroup-specific thresholds in clinical applications.
Indeed, previous studies have indicated that the effectiveness of the p-tau217 and Aβ42/40 combination model is greater in CU individuals than in CI individuals. In studies focused solely on CI individuals, the APS2—derived from the %p-tau217 and Aβ42/40 combination—primarily enhanced model fit relative to the %p-tau217-only model, with minimal impact on AUC [28]. Conversely, in studies of CU individuals, models incorporating both %p-tau217 and Aβ42/40 demonstrated improved adjusted R² and overall model fit compared to models based exclusively on %p-tau217 [29, 31, 46]. Furthermore, in a study that separately analyzed CU and MCI groups, although direct comparisons were not performed, the combined model appeared to be more effective in the CU group [30]. Similar findings were also observed in another study employing the Fujirebio platform, reinforcing the notion that the added value of Aβ42/40 is particularly pronounced in the early, cognitively unimpaired stage [47]. These findings underscore the stage-dependent diagnostic value of plasma biomarkers in AD. Specifically, the enhanced performance of the combined model in CU individuals suggests its potential utility for early detection and patient stratification, which is crucial for timely intervention.
Conversely, GFAP and NfL, which primarily reflect neuroinflammation and neurodegeneration, did not substantially improve Aβ detection in either group. While these markers have been associated with AD pathology and have shown potential for tracking disease progression [26, 48,49,50], their role in early Aβ accumulation appears to be limited. In our study, although GFAP and NfL contributed modestly to model fit improvements, their impact was not as pronounced as that of Aβ42/40, particularly in CU individuals. This suggests that while GFAP and NfL may provide additional insights into neurodegenerative processes, they do not directly enhance the ability to detect Aβ pathology in its earliest stages.
Our final major finding was that in CU individuals, the combined model significantly improved diagnostic performance in specific subgroups, particularly older individuals, females, and APOE4 non-carriers, regardless of obesity status, with consistent enhancements in AUC and model fit across both the SIMOA and MSD assays. These findings suggest that integrating p-tau217 and Aβ42/40 may enhance individualized risk assessment in CU. In contrast, while younger individuals, males, and APOE4 carriers showed a trend toward improved AUC and model fit, these changes did not reach statistical significance. Interestingly, in CI individuals, the combination model did not significantly improve AUC across most subgroups, except in males, where a modest but significant increase was observed. The reason for this sex-specific effect remains unclear, highlighting the need for further investigation. These results underscore the potential of plasma biomarker combinations for refining individualized risk assessment and early detection strategies in AD. Further large-scale studies are needed to determine how demographic and genetic factors modulate their effectiveness.
Our study has several strengths. It utilized a large, well-characterized cohort with both plasma biomarker and Aβ PET data, enabling development of diagnostic models and assessment of their generalizability across clinical and demographic strata. The cut-off–based amyloid probability score was further validated in an independent subset from other centers, supporting its applicability across different recruitment sites. However, several limitations should be acknowledged. First, although our overall sample size was large, some subgroups defined by age, sex, BMI, and APOE ε4 status, especially within the CU group, had relatively small sample sizes. Therefore, caution is warranted when interpreting subgroup-specific model improvements, and these findings should be validated in larger, independent cohorts. Second, although findings were consistent across both SIMOA and MSD assays, potential platform-specific variability in plasma biomarker measurements cannot be entirely excluded. Also, although logistic regression was used in this study, future work may explore clinically implementable alternatives such as decision trees or point-based scoring systems. Finally, the use of Aβ PET positivity as the reference standard may not fully capture the complexity of AD pathology, particularly in early stages where tau accumulation and neurodegeneration also play critical roles. Despite these limitations, our study provides important evidence supporting the complementary role of p-tau217 and Aβ42/40 in detecting early Aβ pathology, particularly in CU individuals. These findings underscore the potential of integrated plasma biomarker strategies to improve the accuracy and efficiency of AD diagnostics in preclinical stages.
In summary, our study demonstrates that combining p-tau217 with Aβ42/40 significantly enhances Aβ detection in CU individuals, improving both diagnostic accuracy and model fit, whereas its impact in CI individuals is limited to modest model fit improvements. These findings highlight the complementary role of Aβ42/40 in capturing early Aβ pathology and suggest that plasma biomarker combinations may offer a more sensitive approach for detecting preclinical AD.
This work may serve as a foundation for future research aimed at developing clinically practical approaches for biomarker-based risk assessment.
Table 2 Validation performance of the amyloid probability score in other centers

Comments (0)