
Remember me




Surgical complications are widely documented to occur more commonly in older persons (Table 1). This is accompanied by higher mortality rate, longer postoperative stays and a higher chance of being discharged to a facility other than their normal residence [7]. Complications could also be higher than what is reported in studies given emergency appointments with primary care or nursing home doctor may not be tracked in their hospital records at the time of study reporting [8]. In a review of complications post radical cystectomy (RC) in elderly patients, Froehner et al., reported that the difference in rates between age groups is even higher when comparing 30 days to 90 days [9]. In a more recent study addressing mortality rates post RC, 90-day mortality increased > 80 years (odds ratio [OR] 3.42, 95% confidence interval [CI] 1.62–7.22). Most urological studies focus on 30-day outcomes for reporting adverse events, while in this age group it is arguably important to extend this to 90 days to give greater insight. In a study of patients aged ≥ 85 years undergoing ureteroscopy for kidney stones, 41% suffered a complication of some kind within 90 days [10].
Table 1 Key themes and summarised findingsPredicting Life ExpectancyA core element in decision making in surgery for the elderly is their expected life expectancy, particularly over the next 10 years. The latter is for example, a common decision factor when considered radical prostatectomy (RP) for localised prostate cancer. A number of studies have consistently found that both doctors and nurses are poor at estimating 10-year survival and predominantly underestimate it [11, 12]. Accuracy for this particular dichotomous outcome is far more accurate on a short-term basis but the horizon effect occurs as increasing imprecision of predictions is observed as the time frame extends further into the future [12].
More objective tools include statistical models based on registry cohorts of populations with a particular disease such as the model described by Zhou et al. for predicting risk of death post radical prostatectomy using the Surveillance, Epidemiology, and End Results (SEER) database [13]. Another option for clinicians is use of actuarial predicted survival data sourced from national statistics and these are the most commonly used by institutions such as National Institute for Health and Care Excellence (NICE) when making recommendations for treatment considerations. A previous review evaluating all these different methods found that these tools are superior to clinican predicted life expectancy but still lack accuracy [12]. Using purely age cut offs when deciding suitability for treatment is discouraged, and is increasingly considered to constitute “ageism” [14]. Rather, individual patient characterics should should be weighed up while appreciating their wishes and projected life expectancy.
Geriatric Assessment MethodsA number of tools are available to aid the evaluation of health status and that can provide more information beyond just age and performance status alone. Their regular clinical application receives a strong recommendation from the European Association of Urology (EAU) Prostate cancer guidelines [15]. The Geriatric 8 (G-8) screening tool is specifically highlighted. Developed by Ballera et al., it can be used to identify cancer patients who would benefit most from a comprehensive geriatric assessment (CGA) [16]. It includes seven items from the Mini Nutritional Assessment (MNA) questionnaire that cover nutrition, mobility, cognitive status, polypharmacy with the final component being the patient´s age. It is freely available in an online calculator format also. Possible scores range from 0 to 17 with lower values indicating poorer health status and the guidelines advise full assessment for < 15. The tool can be useful to identify potentially reversible conditions that can be improved before a final decision is made on the feasibility of surgery.
An alternative to the G-8, is the Erlangen Index (EI) that covers five areas of geriatric assessment including mobility, dependence status, frailty, American Society of Anesthesiologists (ASA) physical status and the Charlson Comorbidity Index (CCI) [17]. Designed for assessing elderly patients undergoing major uro-oncological surgery, Graf et al., recently validated this tool and determined it as a reliable method for identifying elderly patients not only at high risk of mortality but also persistent functional impairment [18].
Other tools to consider incorporating are those for specific aspects such as for frailty (e.g., Clinical Frailty Score (CFS)) and cognitive function (e.g., Mini-Cog). Sun et al. found that CFS scores ≥ 5 were associated with a more than 10-fold increase in the risk of major complications after uro-oncological surgery and over a 20-fold increase in the risk of functional decline at 90 days [19]. Eredics et al. found that frailty was the biggest predictor for one year mortality for nonagerians admitted acute to urology wards [20]. Yajima et al. reported that a Mini-Cog score of < 3 was a clear precictor (OR = 9.5; p < 0.001) for delirium after urological surgery [21]. Of note, however, a recent survey highlighted that less than 15% of urologists use geriatric assessment tools in their clinical practice [22]. Why this is so, is likely multifactorial. It may be partly attributable to lack of awareness. Practical challenges may also be a contributor too. More extensive geriatric assessments such as the GCA are time consuming and can represent a resource that is not available. The GCA itself, refers for several assessments made by wider members of the multidisplinary team and is a process rather than a single evaluation in time [23]. In a systematic review by Partridge et al., the authors found that implementation of GCA improves post-operative outcomes the elderly [24]. However, there is such heterogeneity in how they are performed, that the authors concluded that it remains unanswered which part of GCA actually contributes the most, the so called ¨blackbox effect´.
Clinical InterventionsBraude et al., initiated a Proactive care of Older People undergoing Surgery (POPS) intervention for elderly inpatients in urology [25]. Through implememntation of regular multidiscipinlary meetings and ward round involvement from a geriatrician, the length of stay was decreased by 19% as well as fewer complications and re-admissions. This method of POPS has been previously applied across a range of specialities with good effect [26]. Hospital at home (HaH) is another initiative that has been promoted across several countries. It facilitates a step down from the ward setting where patient can still receive much of the care that is traditionally only deliverable in secondary care such as intravenous medication and monitoring. In a Spanish cohort study of 325 patients undergoing major surgeries including RC, it allowed for shorter length of stay and re-admission rate of 7% [27].
Decision Making – Adopting a Conservative ApproachThe maxim “Good surgeons know how to operate; better ones know when to operate; and the best know when not to " is well-established in surgical tradition—yet it is perhaps even more relevant when treating patients in this age group. While numerous studies do report acceptable outcomes in elderly patients, caution is warranted when attempting to generalise these findings. Due to the retrospective nature of these studies, there is an inherent selection bias: patients with significant comorbidities who underwent surgery were typically deemed suitable by experienced clinicians at tertiary centres, based on clinical judgments that may not be fully captured or reproducible within the study data [10, 28]. While it is still absolutely positive to have reports from tertiary centres that support the feasibility of such surgeries, what would be even more valuable would be for the follow up outcomes to be attained for those who were deemed inoperable.
There are a lack of studies exploring patient perspectives when facing the decision of surgery in the elderly. However, in a study by Lavery et al., older age was identified as significant predictor for decisional regret associated with RP [29]. García-Rodelas et al., reported findings from a qualitative study of elderly men who had undergone RP and reported consistently poor experiences among the participants [30]. Ensuring that patients are clearly informed about their alternatives, including the discussion around ‘What if we do nothing?‘, is a key aspect of the Scottish approach known as ‘Realistic Medicine’ [31]. This aligns closely with the principles of ‘Choosing Wisely’ in the United States [32]. It is therefore important for clinicians to ensure information has been communicated in an appropriate way and to make adjustments as necessaey including regarding health literacy [33].
Treatment SuccessIn this age group, treatment success should arguably be defined more broadly. For example, in a young patient with renal stones, success may not be considered to have been achieved if follow up imaging does not show a 100% fragment free status [34]. However, in an elderly patient, dealing with the culprit stone is arguably the priority and the threshold to accept residual fragments can be higher. Residual fragments should not therefore constitute unsuccessful treatment. When performing bladder outflow surgery for an extremely elderly male with a long-term catheter, their predicted life expectancy may be limited. However, even one or two years living potentially catheter free may have such a positive impact on their quality-of-life treatment, that surgery should be considered even if the estimated life expectancy is relatively short.
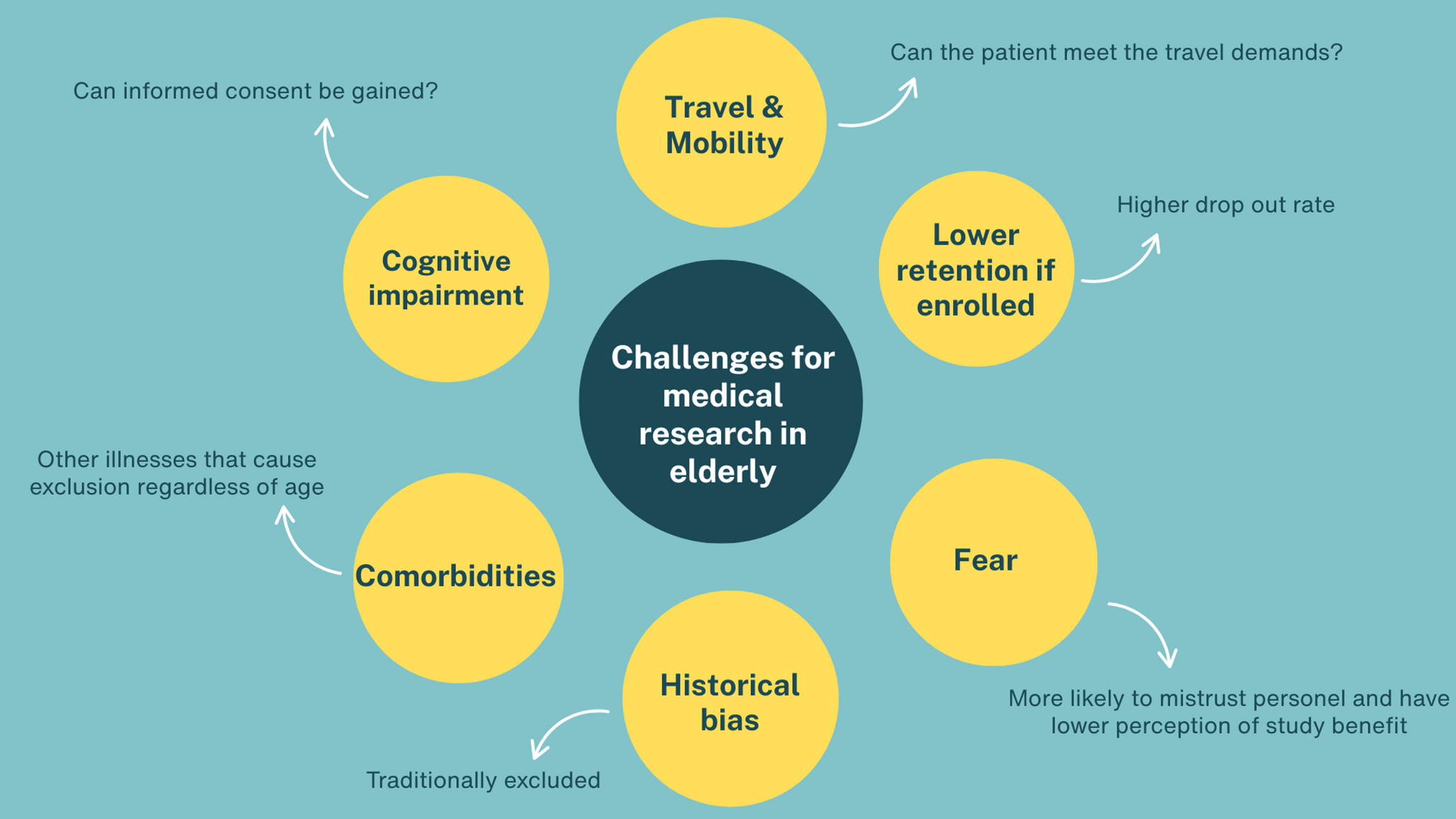
Challenges in Undertaking Research Studies in the ElderlyThere are many possible reasons why older persons are poorly represented in surgical research (Fig. 1). Firstly, the majority of clinical trials and prospective studies typically exclude elderly patients [35]. Even if eligible on age, they are more likely to have a comorbidity that is a separate exclusion criterion. Additional demands of a trial may be deemed too burdensome such as travel or additional follow up visits. Provencher et al., performed a systematic review evaluating challenges faced by the elderly in trials and cited lack of perceived benefit and distrust of research staff as commonly reported factors [36]. The higher likelihood of cognitive impairment can also raise ethical concerns regarding participation. While it is possible to gain consent for such a patient group, it is a more complex and time intensive process. From a practical perspective, the historical trend has often been to not include older persons in surgical trials as is reflected in the literature [37].
Fig. 1
Summary of challenges for performing medical research in the elderly
Future Research NeedsIn addition to more research on urological surgery in the elderly, these should consider incorporating outcomes that are often not routine in the index patient. While mortality and complication burden are important, there are other elements that are of great relevance for quality of life that should not be overlooked. This includes impact on functional status including mobility and home status (e.g., Did the surgery result in the patient being permanently relocated on a permanent basis to a nursing home? ). Use of patient reported outcome measures (PROMs) are encouraged as these have been used to a lesser extent in elderly study samples [38].
Comments (0)