The safety and feasibility of percutaneous endovascular techniques in the pediatric population are poorly described in the literature, in part due to the markedly lower prevalence of pediatric ESRD, compounded by the fact that dialysis serves a non-permanent role as a bridge to transplant.
The findings of this study suggest that the techniques discussed may be both safe and effective for maintaining pediatric dialysis accesses. It is notable that no complications were observed during or after any of the 67 interventions. In adults, rates of complication in angioplasty use for dialysis access have been reported to be 3% to 5% [17]. Though no complications were observed in the 67 interventions examined, great care must still be taken as these techniques are used in future management. Some of the most-observed complications of the described endovascular techniques include vascular injury (dissection, perforation, rupture), infection, and bleeding, either at the access site or due to systemic thrombolysis or anticoagulation. Congenital anomalies that contribute to ESRD, such as CAKUT, impact physiology in complex ways. Such conditions may impact the discrepancy between the technical and clinical success rates observed, as well as the gap between clinical success rates in children and adults [18]. A lack of protocol-driven decision-making may impact long-term success in unknown ways. Interventionalists might prioritize minimizing harm over efficacy, favoring lower complication risk at the cost of long-term patency—or, conversely, adopt aggressive techniques that enhance patency but increase risks like endothelial damage or hemorrhage. Additionally, incomplete understanding of pediatric ESRD pathophysiology likely contributes to the relatively low long-term patency compared to adult fistulas.
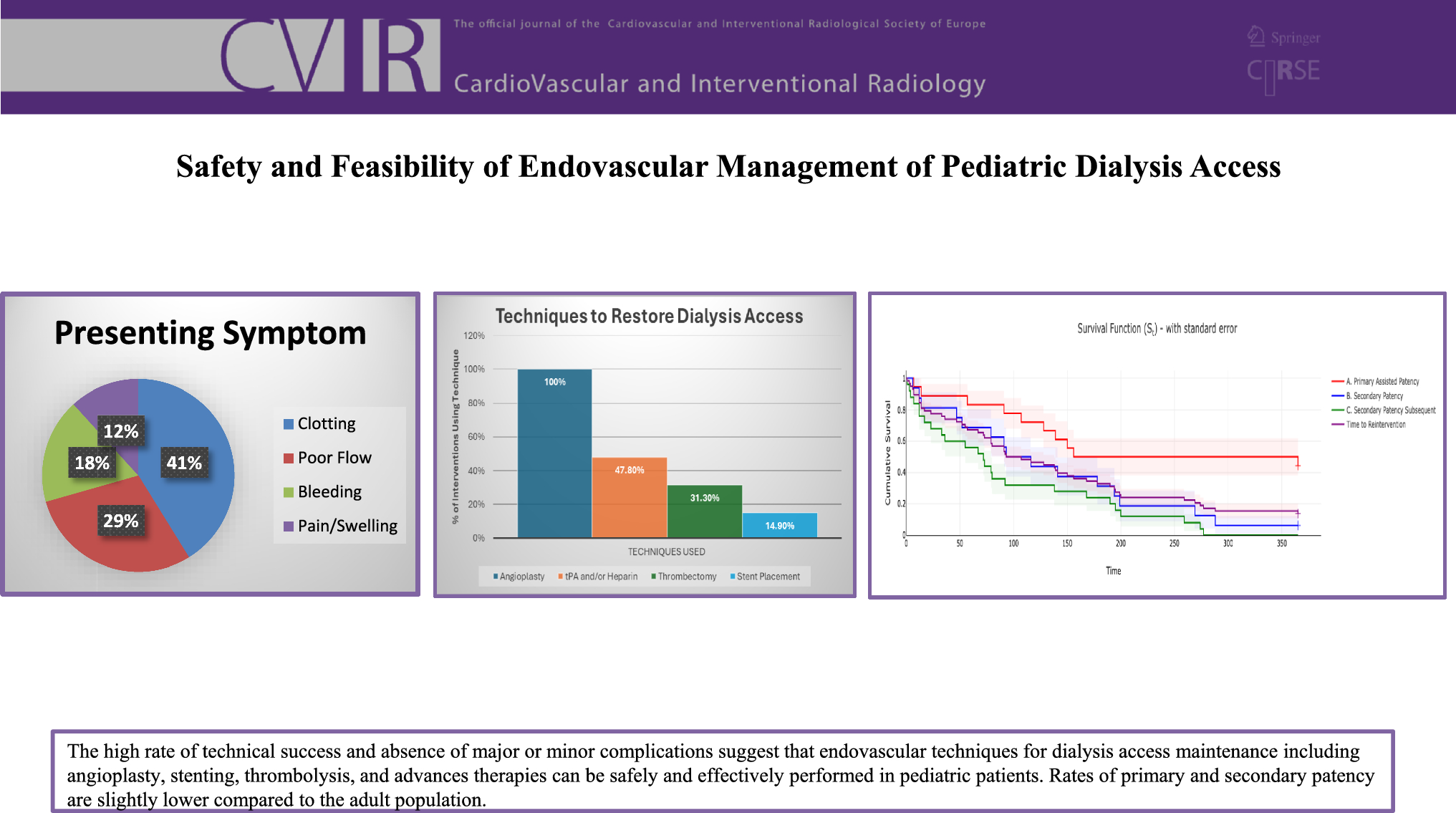
The high burden of comorbidities in these patients makes it difficult to determine whether clinical failure reflects ineffective technique or underlying disease. Pediatric vessels' growth potential, unlike in adults, must also be considered when interpreting low clinical success rates. Stent use highlights these challenges, as ongoing growth poses risks of migration and neointimal hyperplasia leading to in-stent stenosis. Angioplasty emerges as a primary option, as it was the markedly the most-employed technique. Studies have shown that in the adult population, use of angioplasty alone for dialysis access maintenance resulted in clinical success rates of 42–63% for fistulas and 27–61% for grafts [17]. The observed rate of combined 6-month primary assisted and secondary patency in this study was 41.8% across all interventions, and it would not be possible to extricate the impact on 6-month patency of angioplasty alone. However, as angioplasty was employed in every intervention, adult patency rates provide an important datapoint for comparison.
Stent placement served as a supplement in the relatively few cases where angioplasty alone was insufficient to resolve stenosis. Stents were also used to provide structural support to vasculature refractory to angioplasty to minimize the need for future reintervention. Stents were also indicated for symptomatic relief of pain and swelling in such areas unresponsive to angioplasty alone. All six patients receiving stents had undergone multiple previous procedures involving angioplasty.
Risk of vascular trauma and subsequent acute or chronic thrombosis must be acknowledged when selecting a location for stent placement and considering perioperative and long-term pharmacological management. Introduction of any stent, particularly a bare metal stent over a drug-eluting stent, can predispose to recurrent thrombus [19]. Patency rates may have been impacted by development of thrombus at stent sites, as suggested by the patients who received one or more stents and later received heparin and/or tPA.
Use of pharmacological thrombolytics and rotational thrombectomy devices was complimentary and was shown to be safe and feasible. The combined use of alteplase and percutaneous rotational thrombectomy devices was effective in clot dissolution in the setting of large or resistant thrombus. Possible adverse events especially relevant to these techniques are embolization of thrombotic debris once dislodged [20]. Ways to mitigate risk of these events occurring include thorough maceration of thrombus to the point that any debris is of insignificant size and intraprocedural placement and removal of an inferior vena cava filter.
Risks must still be addressed, even though no complications were observed. While percutaneous access is minimally invasive, wire-guided angioplasty, stenting, and thrombectomy can disrupt stenotic plaques or thrombi, leading to local vascular trauma. Pharmacologic thrombolytics also carry bleeding risks at the treatment site or systemically. These risks were minimized through careful anticoagulant and antiplatelet selection, conservative dosing, and individualized access site choice. Extensive operator experience in adults lent itself toward greater care in pediatric interventions. Additionally, pediatric vessels may be more resilient than adult vessels, which often suffer from chronic inflammation due to smoking, diabetes, or ESRD. Several limitations must be acknowledged. First, the overall sample size is low, due at least in part to the rarity of pediatric patients requiring a fistula or graft. However, the study was intended to explore safety and feasibility and for those aims the sample size does seem acceptable. The relative effectiveness of each individual technique is also difficult to discern given the variability of use in isolation or conjunction with other techniques. Finally, the use of intention to treat, necessary due to the lack of follow-up common in this patient population, like their adult correlates, limits the full capture of long-term outcomes.

Comments (0)