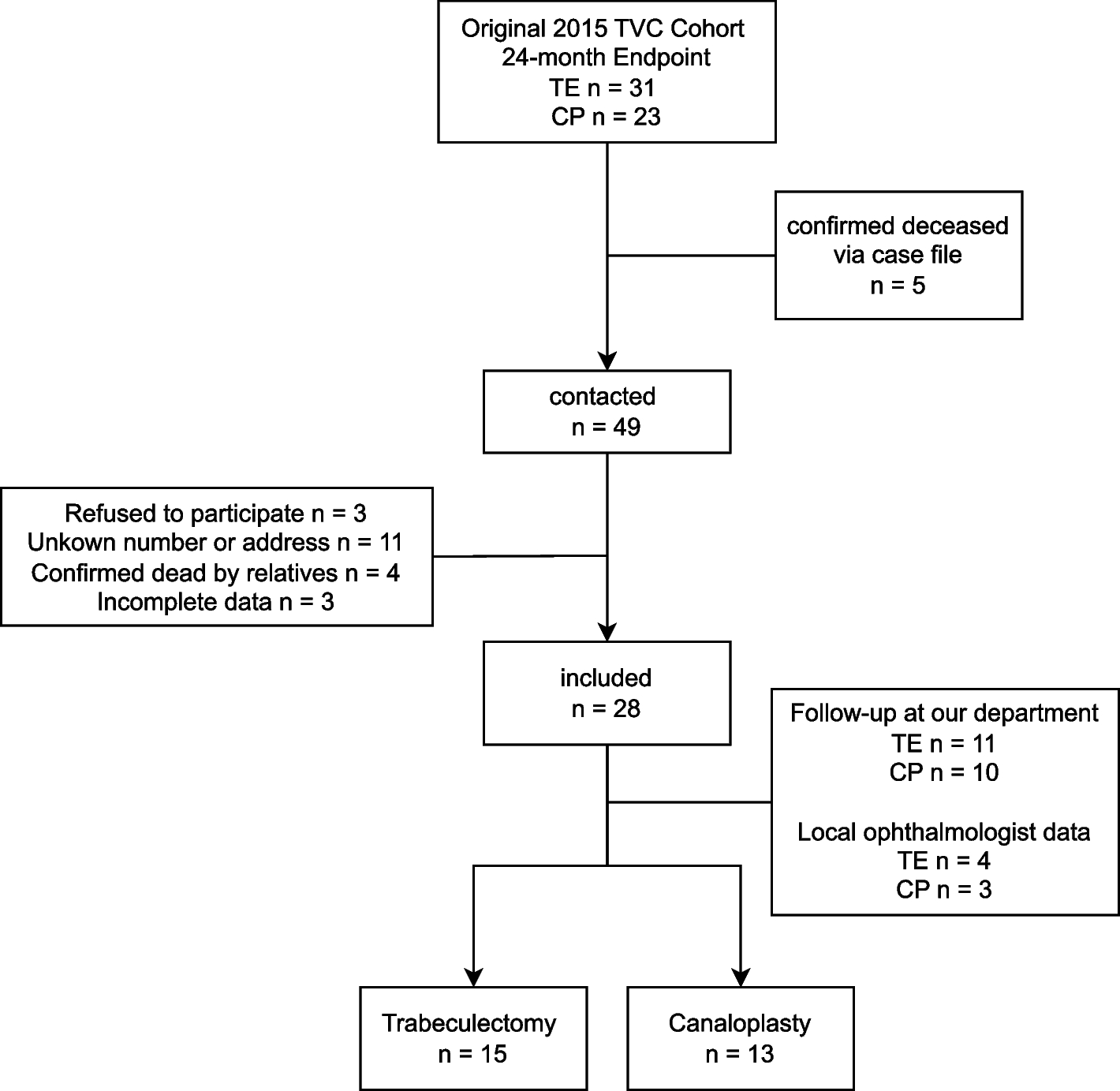
This prospective long-term follow-up evaluates the outcomes of trabeculectomy and canaloplasty in patients from the original TVC trial cohort [2].
At 11 years, TE was superior regarding IOP and cumulative complete success for Definition 1 (IOP ≤ 18 mmHg). However, there was no difference in complete success for Definition 2 (IOP ≤ 21 mmHg AND 20% IOP reduction). Qualified success did not differ between TE and CP patients for either definition.
In the original trial, trabeculectomy demonstrated superior complete success at 24 months for both definitions [2]. However, the reduced sample size in this subsequent study renders it more difficult to demonstrate substantial differences at a p-value of 0.05. Despite this limitation, the confidence intervals suggest a trend towards higher complete success rates for Definition 2 in TE.
Even after 11 years, both procedures effectively lower IOP but TE demonstrates greater efficacy in reducing medication use and achieving medication-free outcomes. Yet, this comes at the cost of an increased risk of complications, with hypotony maculopathy observed exclusively in TE. For patients with moderately low target IOPs who can tolerate some glaucoma medication use, CP remains a reliable and safer alternative.
We were able to follow up approximately 50% of the original cohort. This highlights the challenges of collecting long-term outcome data. These challenges include patient relocation, inability to visit due to declining health, or mortality. To the best of our knowledge, our study reports the longest follow-up of a randomized comparison between trabeculectomy and canaloplasty. Despite these challenges, some studies have successfully conducted long-term follow-up of patients who have undergone trabeculectomy and canaloplasty.
To our knowledge, only one study has compared modified ab externo canaloplasty with trabeculectomy over a follow-up of more than four years [7]. At a median follow-up of 4.6 years, canaloplasty patients had a mean IOP of 13.1 ± 3.3 mmHg and used 0.8 ± 1.0 compounds, while trabeculectomy achieved a lower mean IOP of 11.3 ± 3.6 mmHg and 0.1 ± 0.3 drops. Trabeculectomy also showed superior surgical success, with 66.4% complete success (IOP 5–18 mmHg without medication and revision surgery) compared to 24.3% for canaloplasty. However, the use of Mitomycin C in the modified canaloplasty limits direct comparability with conventional techniques.
Landers et al. reported that 57% of trabeculectomy patients maintained complete success (IOP ≤ 21 mmHg without medication) after 20 years, with a qualified success rate of 88% [8]. Trabeculectomy also demonstrated durability regarding the need for additional glaucoma surgeries, with Chen et al. showing a 15-year probability of 67% for further surgery. However, their definition of success differed and 77.5% (31/40) of the patients resumed glaucoma medication after 41 months [9]. To date, only one study has conducted a follow-up on trabeculectomy patients within a German cohort comparable to ours. Wagner et al. found a general success rate (IOP ≤ 18 mmHg and 20% reduction) of 75% after 5 years, with 67% complete success. At the last follow-up, mean IOP was 12.1 ± 4.3 mmHg, with 0.07 ± 0.26 compounds [10]. These results are comparable to our findings.
Long-term data for canaloplasty, particularly ab externo canaloplasty, is less extensive.
Tognetto et al. compared mid-term outcomes of ab externo canaloplasty and phacocanaloplasty in 30 eyes. At 42 months, complete success without glaucoma medication and IOP of ≤ 18 mmHg was achieved in 20% of the patients, while qualified success was reached in all patients. Mean IOP was 14.3 ± 3.0 mmHg, with an average medication count of 1.7 ± 1.7 drops [11].
Three-year results of a prospective multicenter trial by Lewis et al. show that canaloplasty and phacocanaloplasty are both efficient and safe in treating open-angle glaucoma. Mean IOP three years postoperatively was 15.2 ± 3.5 mmHg, achieved on 0.8 ± 0.9 drops [12].
In 2014, Brusini retrospectively analyzed the three-year outcome of ab externo canaloplasty in 29 patients. At 36 months, mean IOP was 17.3 ± 3.9 mmHg, and the average number of compounds was 1.3 ± 1.5. Qualified and complete success rates, defined similarly to our methods, were 58.6% and 31.0%, respectively [13].
Ennerst et al. reported a longer follow-up of 109 months in a retrospective analysis of 48 eyes, comparing canaloplasty and phacocanaloplasty with similar efficacy in IOP reduction. At 10 years, the mean IOP was 14.8 ± 2.0 mmHg, with an average medication use of 0.5 ± 0.9 compounds [14].
The IOP findings regarding the long-term efficacy of canaloplasty align with our results on long-term efficacy of canaloplasty. Similarly, the number of medications appears to be generally comparable with exceptions noted in the findings of Ennerst et al. and Stingl et al. [7, 14].
Beyond long-term IOP reduction and medication use, the occurrence of late complications is a crucial parameter. Non-penetrating procedures like canaloplasty are generally safer than trabeculectomy [15]. Transient hyphema is a common complication of canaloplasty, occurring in 21–40%, while hypotony rates are low (0.6–20%) [7, 16]. In contrast, trabeculectomy has higher complication rates (7–40%), including hypotony maculopathy (4–7%) and bleb-related complications (1.6–23%) [16,17,18]. In our cohort, hypotony maculopathy was the only long-term complication occurring in 15.4% (2/13) after trabeculectomy. These findings highlight possible detrimental consequences of excessively low IOP, reinforcing the relevance of incorporating both upper and lower IOP thresholds when defining surgical success. No bleb-related complications were observed.
Collecting long-term data remains a significant challenge, as seen in the small sample sizes of many studies and our own cohort. However, such data is vital for evaluating the long-term efficacy of glaucoma procedures. We emphasize the need for prospective long-term studies and extensive registries to generate reliable data and support individualized treatment approaches.
While we achieved sufficient power (0.8) for CP by including 13 of 23 former patients from the 24-month primary endpoint, the comparison for TE lacked power, with only 15 of 31 patients included. Achieving a power of 0.8 required at least 50% of former patients, highlighting a key study limitation. Nevertheless, the relatively small overall sample size may limit the generalizability of the findings and should be taken into consideration when interpreting the results. Another limitation is reliance on community-based practitioner data, which may introduce bias despite consistent use of Goldmann applanation tonometry. The significant difference in the visual field mean defect between TE and CP suggests more severe glaucoma in the TE group. Although the original cohort was randomized, it is unclear if this discrepancy existed at baseline. The similar rate of visual field progression suggests that both surgical procedures provided comparable long-term IOP control, which likely contributed to a similar rate of structural and functional decline. Some continued deterioration is expected given the chronic nature of glaucoma and the extended follow-up period. Additionally, the advanced age of participants at follow-up may affect visual field reliability due to factors such as fatigue, reduced concentration, or comorbidities. Nevertheless, the parallel trends in functional and structural parameters support the internal consistency of our findings.
Despite its limitations, the study’s long follow-up is a major strength, offering valuable insights into long-term outcomes of both procedures. The consistent mid-term results reinforce the reliability of the findings and highlight the importance of long-term data in clinical decision-making. Our results support evidence-based surgical recommendations, demonstrating that both procedures remain widely used after 11 years, underscoring the challenge of new alternatives and trabeculectomy’s enduring relevance in glaucoma surgery.





Comments (0)