
Remember me




Consensus statements
(a) Triaging for DED
1. Specific triaging questions based on TFOS DEWS II should be employed to facilitate the initial differential diagnosis
(b) Screening tests for DED
2. The Ocular Surface Disease Index (OSDI) or the 5-Item Dry Eye Questionnaire (DEQ-5) is recommended for evaluation of the symptoms of DED
(c) Diagnostic tests and DED severity grading
1. To confirm the diagnosis of classic DED, at least one symptomatic test (OSDI or DEQ-5) and one diagnostic test (tear break-up time [TBUT], noninvasive tear break-up time [NITBUT], or corneal fluorescein staining [CFS]) should be positive
2. A TBUT of ≤ 5 s is regarded as a positive diagnostic test result for DED
3. A NITBUT of ≤ 10 s is regarded as a positive diagnostic test result for DED
4. Either the TBUT or NITBUT followed by CFS may be used as a diagnostic test
5. If a patient presents with symptoms but no signs, they should be assessed for neuropathic pain conditions and managed appropriately
6. If a patient presents with signs but no symptoms, they should be assessed for neurogenic conditions and classified as having asymptomatic DED; they should then be managed appropriately
7. If a patient has symptoms but no signs or has signs but no symptoms, they should be assessed for a preclinical dry-eye state and managed accordingly
8. Once a diagnosis has been made, CFS can be used to determine the severity of DED
9. Severity can be determined using a grading scheme based on the level of corneal staining
➣ Level 1 indicates no corneal staining and represents mild DED
➣ Level 2 indicates < 1/3 staining of the cornea and represents moderate DED
➣ Level 3 indicates between 1/3 and 1/2 staining of the cornea and represents severe DED
➣ Level 4 indicates > 1/2 staining of the cornea and represents advanced DED
(d) Classification of DED
1. DED can be classified into various subtypes, namely evaporative dry eye (EDE), aqueous deficiency dry eye, or a mixed-type dry eye
2. The meibomian gland dysfunction (MGD) examination should be performed to classify the DED subtype
➣ One of the following tests should be positive to confirm an initial diagnosis of MGD: abnormal morphology (observed using a slit lamp), lid margin abnormalities (gland orifice morphology, gland number, patency, telangiectasia, displacement of the mucocutaneous junction, or signs of blepharitis), abnormal meibum quality, and abnormal meibomian gland expression
➣ Additional EDE examinations—such as meibography, lipid layer thickness measurement, blinking frequency, and completeness—are recommended to enable quantification
3. A positive MGD examination may be used to confirm the diagnosis of evaporative excess-type DED
4. Schirmer’s test without anesthesia is recommended to be performed to classify the DED subtype
➣ ≤ 5 mm/5 min is considered abnormal and may indicate DED
5. An abnormal Schirmer’s test without anesthesia should be used to confirm aqueous deficiency-type DED
6. A positive MGD and an abnormal Schirmer’s test indicate mixed-type DED
The definition of DED has evolved over time in conjunction with advancements in scientific and clinical knowledge. Initially, DED was primarily described as a condition characterized by insufficient or poor-quality tear production, leading to discomfort and irritation. However, our understanding of DED has since expanded to encompass a range of underlying mechanisms that are more complex than initially thought [30]. The TSCRS has considered multiple factors that contribute to the development and progression of DED, including tear film instability, inflammation, and the effect of several symptoms on the perception of ocular discomfort. These facets align with the widely accepted descriptions of DED illustrated in both the ADES and TFOS DEWS II reports [26, 31]. Thus, the TSCRS has proposed a definition for DED that incorporates the complexity and multifactorial nature of the disease, thereby facilitating a comprehensive approach to its diagnosis and management. The definition is as follows: the dry eye is a composite disease of the ocular surface and develops from instability of the tear film, where local inflammatory processes may result in the manifestation of ocular symptoms that contribute to ocular surface damage.
Triaging for DEDThe use of triaging questions assists clinicians in diagnosing DED and guides further evaluation measures and management. In the seven specific triaging questions, adapted from the TFOS DEWS II report [32], detailed inquiries are made into the symptomatic presentation of DED. These questions enable a broad differential diagnosis (Supplementary Table 1).
Screening tests for DEDScreening tools for DED are essential for initiating diagnostic procedures reliant on both the quantification of subjective symptoms and on objective examinations [12, 26, 32]. However, because of its multifactorial nature, DED is challenging to evaluate and diagnose, and this difficulty often results in inconsistencies between clinical signs, diagnostic testing, and symptomatology [5, 33, 34]. Patient screening is thus crucial because non-DED possibilities must be excluded and the diagnostic process can be streamlined, effectively improving clinical experiences and treatment outcomes [12, 26, 32, 34,35,36].
The assessment of symptoms by using questionnaires that are easily interpretable and suitable for routine clinical practice is essential in the diagnosis of DED [37]. Of the DED-specific questionnaires, the OSDI and DEQ-5 are the most widely employed [32]. These are well-established DED screening tools were found to demonstrate concurrent validity [38]. The OSDI contains 12 questions aimed at assessing the severity of ocular symptoms, visual-related function, and environmental triggers of DED [32, 39, 40]. The DEQ-5, a shortened version of the Dry Eye Questionnaire (DEQ), comprises 5 questions focused on assessing disease severity and is widely recommended for clinical use [32, 37, 41]. Both the OSDI and DEQ-5 have exhibited superior discriminative abilities with reliable sensitivity and specificity, substantiating their benefit in clinical practice [32, 42, 43]. However, when using the OSDI, environmental factors that may influence the scores should be considered. For instance, Taiwan's relatively humid climate may lead to variation in OSDI scores compared with the scores obtained in drier regions or Western countries. The OSDI is available in various translated formats, including Mandarin [44]. However, validated DEQ-5 and OSDI questionnaires in Traditional Mandarin are not currently available.Footnote 1
Diagnostic tests and severity grading of DEDInitial evaluation of DED by using validated questionnaires facilitates its preliminary identification. Subsequent confirmation is achieved using various diagnostic tests based on certain established criteria [12, 26, 32]. Currently, the ADES diagnostic criteria are commonly employed in Asia for the diagnosis of dry eye [45]. A tear-film-oriented diagnosis is used in both the ADES and Japanese Dry Eye Society [30]. This approach involves assessing ocular surface damage, tear film stability, tear secretion, tear volume, tear osmolarity, and the lipid layer as fundamental components of the DED diagnostic process [46,47,48]. Clinical evaluation of the ocular surface has revealed that an unstable tear film is the most common sign of dry eye, as determined through TBUT analysis, a popular test used to examine dry eye in clinical practice [31, 32, 49]. A short TBUT of ≤ 5 s has been identified as the primary characteristic of dry eye and is the essential criterion for diagnosing dry eye [12, 26, 32, 33, 50]. However, although TBUT is the traditional method used to evaluate DED, application of aqueous fluorescein may affect the final result. Therefore, the NITBUT can also be used in clinical practice, with a reading of ≤ 10 s being regarded as a positive clinical sign of DED [31, 32].
Given the composite nature of DED, singular pathognomonic criteria do not exist, and a combination of clinical sign examinations and symptom evaluations is necessary to establish an accurate diagnosis [51]. Diagnosing DED solely on the basis of symptomatology or clinical sign discrimination lacks specificity because numerous ocular surface diseases may present with similar subjective indications [24]. Furthermore, establishing a clear correlation between signs and symptoms is complicated because fewer than 60% of symptomatic patients present with signs of DED [52, 53]. The complex pathophysiology of DED, in conjunction with poor correlations between various clinical DED tests, results in evident discordance between the various indications [24, 54,55,56]. In light of this complexity, neurosensory abnormalities have been identified as crucial components contributing to the multifactorial etiology of DED. Symptoms appearing in the absence of signs can indicate a neuropathic or preclinical dry eye state. Similarly, signs identified in an asymptomatic state can indicate preclinical or asymptomatic DED resulting from decreased corneal sensitivity, neurogenic DED, or a predisposition to dry eye [27, 57]. According to the TSCRS expert consensus, classic DED can be diagnosed when both a symptomatic test and a diagnostic test yield positive results.
Classification of DEDPhysicians can observe ocular surface changes at a cellular level and assess tear film stability through a slit lamp examination by using corneal and conjunctival dyes, such as fluorescein, Lissamine Green, and Rose Bengal. Tear film stability is reflected by different break-up patterns indicative of various pathophysiologies, providing valuable insights into the assessment of DED severity [58, 59]. CFS is one of the methods most commonly used for grading the severity of DED and is widely regarded as a crucial and reliable tool frequently used in both clinical and research settings [32, 60, 61]. According to the TFOS DEWS II severity grading scale, severity level is determined through the objective measurement of CFS and categorized into Levels 1, 2, 3, and 4, corresponding to mild, moderate, severe, and advanced DED, respectively. In addition, the proposed assessment considers TBUT or NITBUT results and subjective measurements obtained through patient symptom assessment, all of which assist in determining the relevant severity level [14, 31, 62].
According to the TSCRS consensus, DED severity can be determined from staining results. Level 1 indicates no corneal staining, level 2 indicates < 1/3 corneal staining, level 3 indicates between 1/3 and 1/2 corneal staining, and level 4 indicates > 1/2 corneal staining. Because of variation in the grading schemes used for quantifying CFS severity, it is recommended that in cases where discrepancies may arise, the most severe level should be adopted and the appropriate corresponding treatment should be implemented [62].
Substantial scientific and clinical evidence supports the classification of DED on a continuum ranging from EDE, the most prevalent type, to aqueous deficient dry eye (ADDE), with conditions frequently overlapping [1, 31, 63]. Meibomian gland dysfunction (MGD) is the leading cause of DED and the primary contributor to the EDE subtype [31]. MGD grading involves the assessment of clinical features and gland expression through multiple methods, including morphology (slit lamp examination), meibomian gland expression, meibography, and lipid layer thickness measurement [64, 65]. Schirmer’s test is an invasive test used to examine tear volume and the rate of aqueous tear production; it is most useful in cases where ADDE is suspected [66]. Given the variability in diagnostic cutoff values, the TSCRS has determined a Schirmer’s test value of ≤ 5 mm/5 min as being indicative of DED. Patients with values between ≤ 10 and > 5 mm/5 min may be categorized as borderline DED cases, in line with the diagnostic accuracy observed in several reports [32]. The complex pathophysiology of DED can lead to a combination of EDE and ADDE presentations, and various diagnostic tools can provide further insight into the etiology in a specific case [63, 67]. Although the pathogenesis of DED involves various alterations in ocular mucins, defining a DED subtype specifically related to mucins remains challenging because of the difficulty of their evaluation. However, ophthalmologists must recognize that DED can arise from mucin abnormalities, which can be assessed through impression cytology and other relevant tests [26, 33, 68].
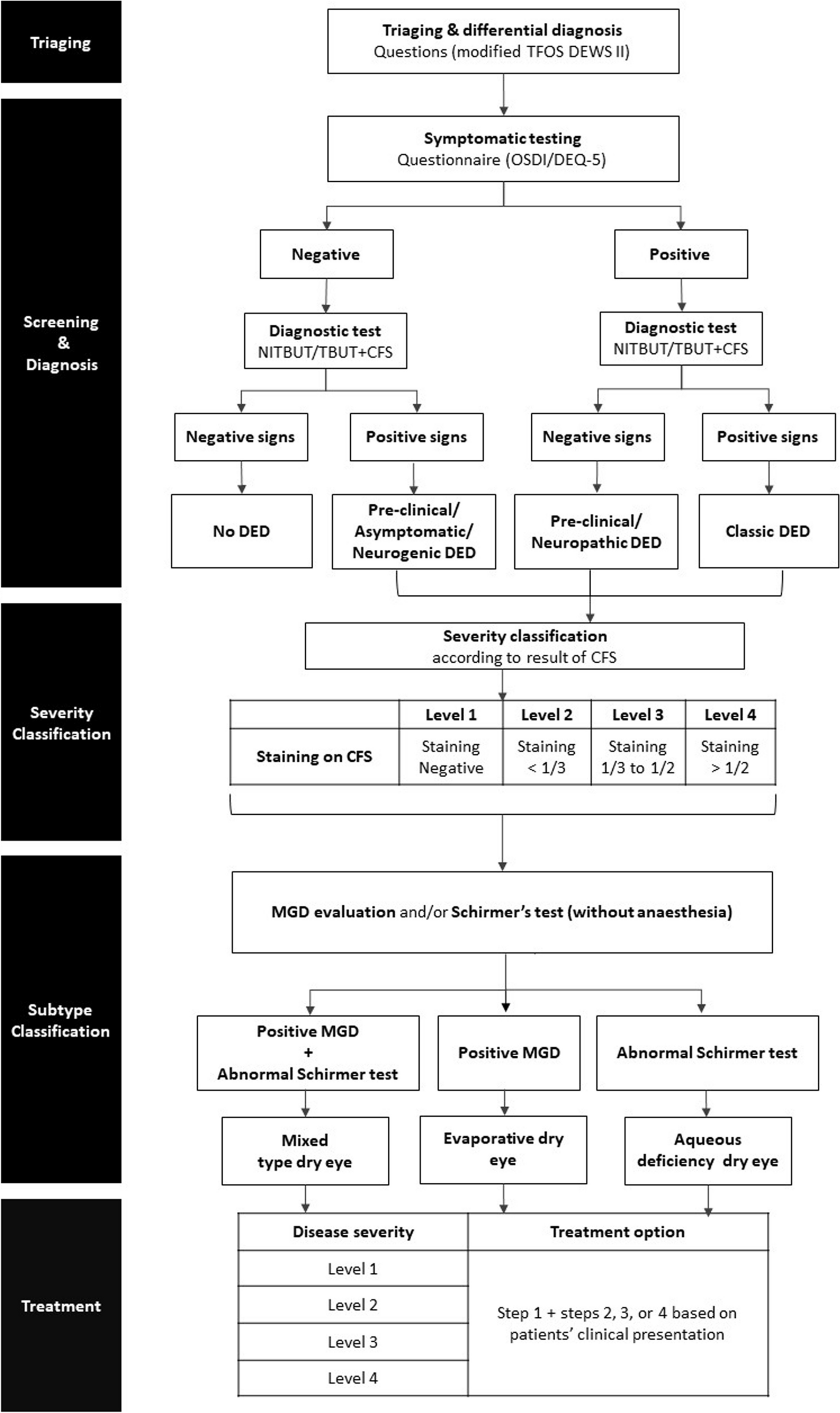
The expert panel has developed a Taiwan-specific algorithm outlining the diagnosis and classification of DED on the basis of the current scientific and clinical evidence in conjunction with expert clinical experience (Fig. 1).
Fig. 1
Algorithm for DED diagnosis and classification in the general population in Taiwan. This clinically designed algorithm outlines the diagnosis, severity classification, subtype classification, and related management procedures for DED in the general population. Abbreviations: CFS, corneal fluorescein staining; DED, dry eye disease; DEQ-5, 5-Item Dry Eye Questionnaire; MGD, meibomian gland dysfunction; NITBUT, noninvasive tear break-up time; OSDI, Ocular Surface Disease Index; TBUT, tear break-up time; TFOS DEWS II, Tear Film and Ocular Surface Society Dry Eye Workshops II. Note. In the context of the OSDI or DEQ-5, a positive result typically refers to a higher score, whereas a negative result typically refers to a lower score. However, the interpretation of the result is dependent on the attending ophthalmologist who assesses the score on the basis of the patient’s symptoms and clinical findings. A TBUT of ≤ 5 s is considered positive and a TBUT of > 5 s is considered negative. A NITBUT of ≤ 10 s is considered positive, and a NITBUT of > 10 s is considered negative. In the algorithm, the disease severity levels 1, 2, 3, and 4 correspond to mild, moderate, severe, and advanced DED, respectively. The details of treatment option steps 1 + 2, 3, or 4 in the algorithm refer to Table 1
Table 1 Recommended treatment approach for the management of DED in the general populationTreatment and managementConsensus statements
1. Individualized management of DED should be implemented in a step-wise approach
2. Treatment should be offered in 4 steps and directly correspond to the 4 disease severity levels
3. Step 1 treatment should be applied to all cases of DED in conjunction with the treatment step corresponding to the severity level diagnosed on the basis of the patient’s clinical presentation
4. Response to treatment should be measured in accordance with symptom reporting and clinical observations of the TBUT and CFS
5. Higher-stage treatment may be applied in patients who do not respond to the treatment recommended for the corresponding disease stage
6. The escalated treatment may be used in conjunction with the continued application of the previous treatment step
Comprehensive and individualized treatment approaches are vital to successfully restoring homeostasis of the ocular surface. These approaches include various therapeutic interventions that are typically determined by the clinical presentation, accurate diagnosis, disease severity level, and DED classification [14, 69].
The treatment progression for DED follows a step-wise intervention approach, adapted from the protocol of the TFOS DEWS II report, and is presented in Fig. 1. Additional details are provided Table 1 [12,13,14, 70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94]. The process begins with step 1, which emphasizes education, lifestyle modifications, and the use of lubricating eye drops. It then advances to step 2, which involves both nonpharmacological and mild pharmacological management, including use of a nonpreserved ocular lubricant and specific prescription medications. If these initial treatment steps are inadequate, more intensive pharmacological management can be implemented in step 3, with further progression to surgical interventions combined with aggressive pharmacological prescriptions in step 4 [14, 79, 90, 95]. The severity level of DED may be used to determine the corresponding treatment step (Table 2). If a patient responds positively to the initial treatment, the treatment may be de-escalated to the corresponding disease severity level.
Comments (0)