This overview describes the prevalence of pediatric non-cancer chronic pain across different regions, socioeconomic contexts, and among girls [22, 23].
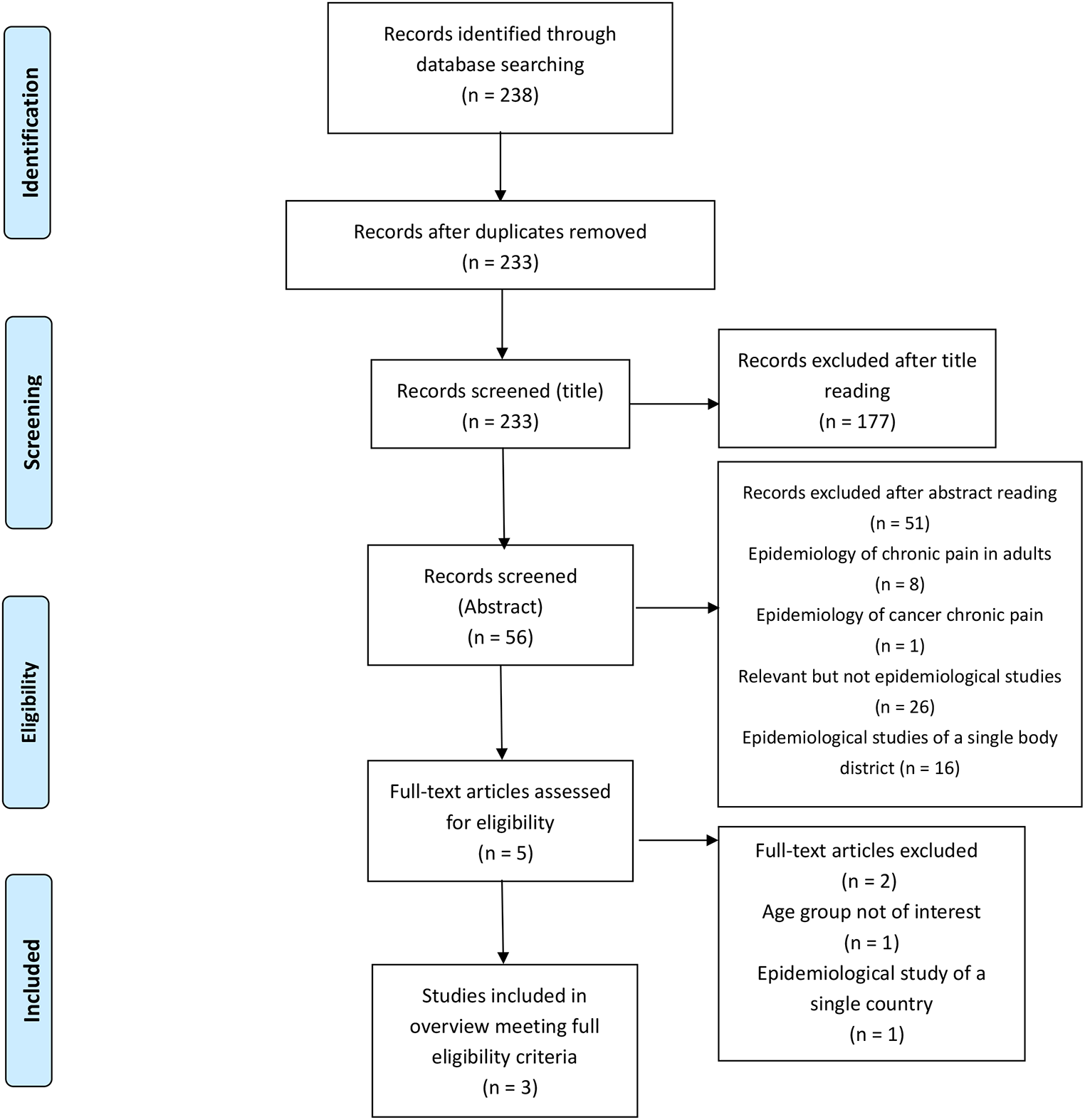
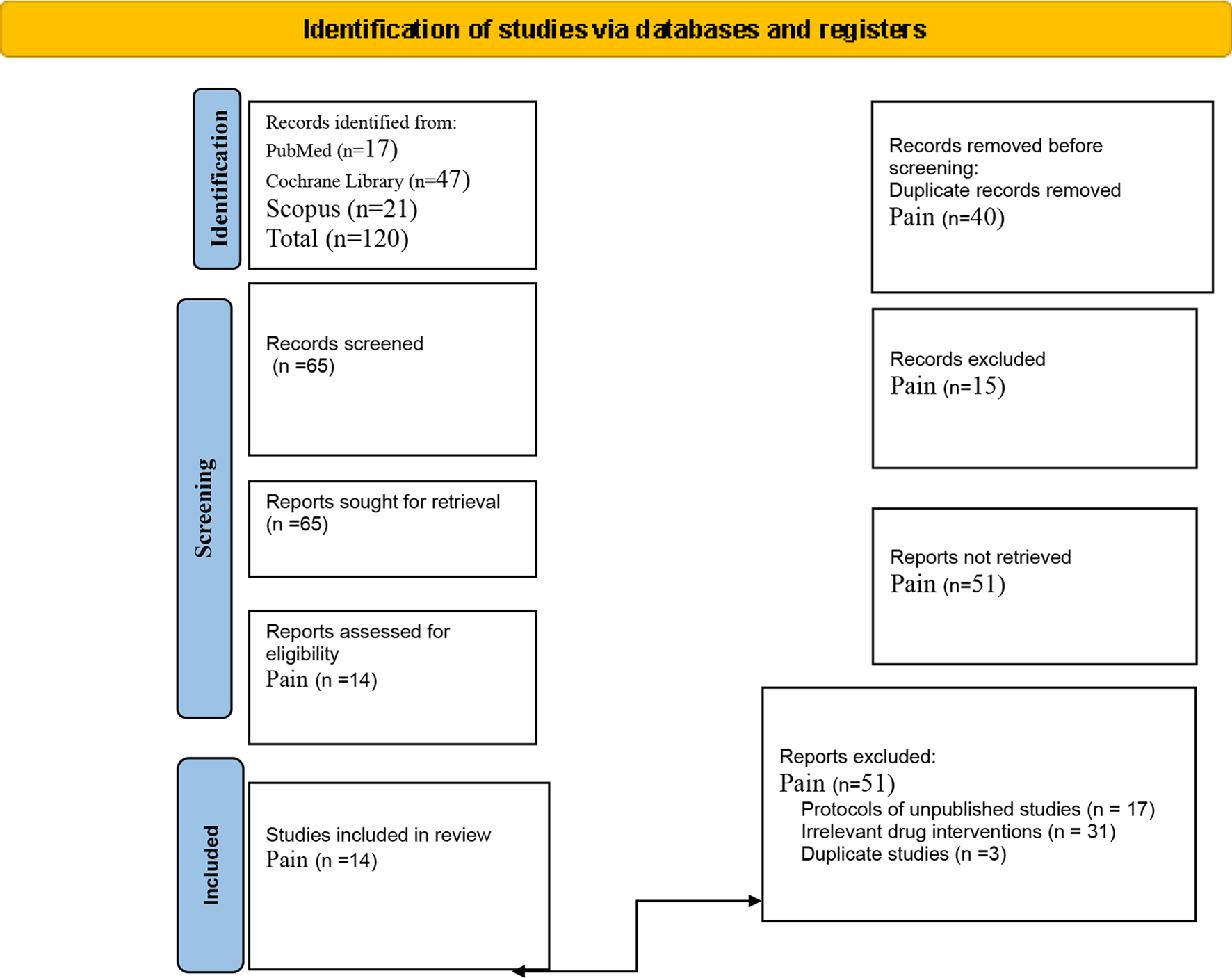
The primary objective of this overview was to synthesize the epidemiology of pediatric non-cancer chronic pain from 178 primary studies included in three systematic reviews. Understanding these prevalence rates is crucial for public health planning and for tailoring healthcare policies in different countries to provide specialized services for pain management [24]. Furthermore, reporting the clinical characteristics of pediatric patients is vital as it offers valuable feedback to pain management professionals, especially those in pain clinics within a structured network. Such data can promote advanced nursing practices and the development of specialized, globally-informed care strategies pediatric [25].
The three systematic reviews included in this overview cover studies over a broad time span from 1993 to 2023. Over the years, there has been an evolution in the international understanding and definition of chronic pain, which is reflected in the temporal spread of the included reviews. King et al. [21] employed the definition of chronic pain, as described by IASP [26]. In contrast, the more recent reviews by Liao et al. [22] and Chambers et al. [23] reflect a shift towards greater standardization, aligning with the International Classification of Diseases, 11th Revision (ICD-11), which defines chronic pain as pain persisting or recurring for at least three months [2]. Their inclusion criteria allowed for varied definitions of chronic pain, with pain duration ranging from one month to six months, or even pain experienced within the last week or year. This lack of standardization likely contributed to the wide range of prevalence rates reported in their reviews. This standardization is crucial for improving the comparability of studies and for accurately assessing the prevalence, the methodologies and interpretations of data. Our results highlight that the revision of King et al. [21] did not provide an overall prevalence rate, in contrast Liao et al. [22] reported a pooled mean prevalence of 8%, and Chambers et al. [23] reported an overall prevalence of 20.8%.
Evidence suggests that lower socioeconomic development and, in some cases, sociocultural factors, contribute to the rising incidence of chronic pain [27], contrary to findings in one of the included reviews [22]. In low- and middle-income countries (LMICs), challenges such as resource constraints, limited access to specialized care, and inadequate healthcare infrastructure are compounded by cultural beliefs and stigma that may discourage pain reporting or care-seeking behavior [28].
The public health implications are particularly concerning in LMICs. Undiagnosed or untreated chronic pain interferes with education, reduces academic achievement, and limits future socioeconomic opportunities. Additionally, it places emotional and financial stress on families, especially in resource-scarce settings [9].
Addressing chronic pain in pediatric populations is critical to improving individual health outcomes and mitigating broader societal impacts [29]. In this overview it emerges that the pediatric population studied has an age range that goes from 0 to 19 years. However, it emerges that the age phase of the pediatric population most represented has a range that is greater than 5 years. It is likely that chronic pain in such a young population (0–4 years) is low and that the adolescent population may be affected by it. Chronic pain is normally attributed and identified only to older patients. It is estimated that about 25% of pediatric patients suffer from chronic pain [30], and these findings confirm that, differently than expected, it is a common complaint in childhood and adolescence, the most affected age group represented by adolescents between 12 and 15 years of age [21]. The review also identified several gaps in the understanding of the epidemiology of chronic pain in children and adolescents, including restricted age ranges and lack of longitudinal studies. The first step to take in order to avoid any possible underestimation of the importance of properly treating pediatric pain is to use necessary and reliable tools in different clinical settings [30].
Unrealistic expectations regarding treatment outcomes can lead to dissatisfaction, emphasizing the need for healthcare professionals to set clear expectations as part of pain management strategies [29]. Managing family expectations regarding treatments and ensuring effective communication by health professionals are important for effective treatment and for supporting families’ psychosocial needs it results in a trusting relationship. Health and social care systems for children and young people’s chronic pain require modification to ensure that a more holistic approach to addressing pain in children and young people is adopted, which considers all biopsychosocial, family-centered health, and social care systems [12, 31].
In the systematic reviews by King et al. [21] and Liao et al. [22] the prevalence of headache, abdominal pain, and multi-site pain was higher in girls compared with boys, and no gender differences were observed in musculoskeletal pain [21]. In contrast, Chambers et al. [23] reported that the prevalence of all types of chronic pain localizationis more prevalent in females than in males. Differences between men and women regarding pain involve anatomical, physiological, neural, hormonal, psychological, social, and cultural factors. When examining those factors, it is found that women report pain more frequently and have a lower threshold for pain than men. They usually experience more muscle-skeletal, neuropathic, electrical shock, and temperature-related pain but respond better to opioids [32]. In terms of sex differences, prevalence of headache, abdominal pain, and multi-site pain was higher in girls compared with boys.
The quality of the included systematic reviews was assessed using the AMSTAR-2 tool. King et al. [21] was rated as having “critically low” methodological quality, as it did not satisfy three critical domains and one non-critical domain. This may limit the reliability of its findings and highlights the importance of rigorous methodological standards in systematic reviews. Chambers et al. [23] was rated as “low” quality, missing only one critical domain. Liao et al. [22] was assessed as “high” quality, indicating strong methodological rigor and increasing confidence in its findings. As shown in Table 2, the three reviews have different reporting qualities using AMSTAR-2. It is possible that the methodological rigor is more evident in the reviews published from 2016 onwards, or that the methodological rigor in place was not explicitly described. A systematic review needs to use a transparently formulated query that uses systematic and rigorous methods to recognize, collect and select, and critically appraise relevant research, and to analyze information from each of the studies that are enclosed [33]. Moreover, only two reviews [22, 23] describe their risk of bias, as their meta-analysis. The most common areas of bias across both studies were lack of national representation and non-response bias [22, 23]. Risk of bias assessment is essential to establish transparency of evidence synthesis results and findings and is a defining element of systematic reviews, often performed for each included study in the review [34].
Table 2 Items of AMSTAR 2Limits
Several limitations are inherent in this overview. The heterogeneity of the included studies, in terms of study design, definitions of chronic pain, makes direct comparisons challenging. The evolution of the definition of chronic pain over time further complicates comparisons between older and newer studies. Additionally, cultural differences in pain perception and reporting can influence prevalence rates. As a result, chronic pain in many countries is likely underestimated due to sociocultural factors of each individual nation, potentially biasing the prevalence data. In LMICs, under-diagnosis and underreporting are likely due to limited access to healthcare services and differing cultural attitudes toward pain and illness. Another limitation found is that of not being able to describe the impact that pediatric chronic pain has on parents and family members, aspects that can be addressed through qualitative clinical research techniques. Another limitation is the potential for publication bias. Studies reporting higher prevalence rates may be more likely to be published than those with lower rates, skewing the overall prevalence estimates. The quality assessment also revealed that not all systematic reviews met the highest standards of methodological rigor, which may affect the reliability of their findings.



Comments (0)