
Remember me


Needle tip placement is fundamental to successful epidural placements, and characteristic fluoroscopic patterns can be seen based on needle placement. Optimal placement of the epidural needle commonly follows characteristic findings on anterior-posterior (AP) and contralateral oblique (CLO) fluoroscopy. Before injection of contrast, the interlaminar space is identified on AP imaging, and appropriate depth is approximated on CLO and lateral imaging.
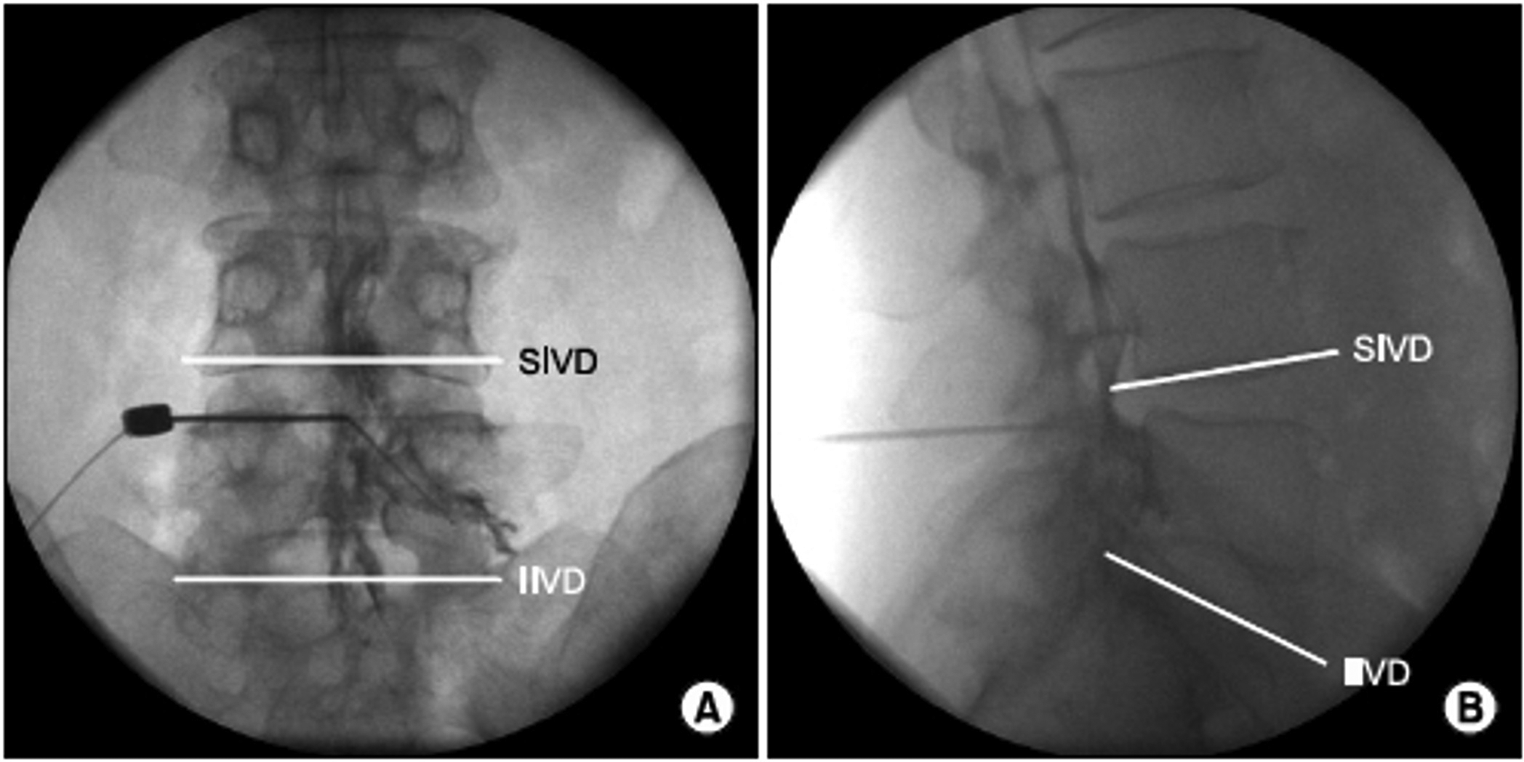
Epidural Contrast PatternsWhen contrast is correctly injected in the epidural space, asymmetric and often unilateral spread of contrast localized between the medial aspect of the pedicle and along the anteromedial aspect of the lamina can be visualized on the AP view (Fig. 1). Additionally, fat vacuolization can be in the AP view, which is a reassuring but not definitive finding seen in optimal epidural placement. On CLO imaging, contrast can be seen traveling the ventral to the lamina along the ventral inter-laminar line (VILL) in optimal epidural placement [9, 10].
Fig. 1
Anterior-posterior (A) and lateral (B) views of epidural steroid injection with contrast localized to the epidural space. (Image courtesy of Giuliano Lo Bianco, MD)
Intrathecal/Subarachnoid Contrast PatternsIntrathecal injection of contrast also follows characteristic patterns that can be visualized on AP and CLO imaging fluoroscopy. In the AP view, the contrast will often localize medially near the midline and be distributed symmetrically within the intrathecal space (Fig. 2). Additionally, in comparison to epidural contrast, the contrast will not be visualized along the medial border of the lamina as the contrast is likely confined to the intrathecal space [9]. On CLO, contrast will not be seen along the VILL, and there is a CSF-contrast fluid-fluid level with contrast located ventrally within the space [9, 10].
Fig. 2
Anterior-posterior (E) and lateral (F) fluoroscopy with an intrathecal spread of contrast. (Image courtesy of Giuliano Lo Bianco, MD)
Subdural Contrast - Localized SpreadSubdural injection of contrast classically presents along two typical patterns. If the contrast is localized to the dorsal aspect of the subdural space, on an AP view, the contrast will show a rounded mass with sharp and distinct margins where thecal layers have not cleaved and a contrast pattern that does not communicate with the medial pedicle on AP or the VILL in the CLO view (Fig. 3) [11].
Fig. 3
Anterior-posterior (A) lateral (B), and CLO (C) fluoroscopy with subdural spread of contrast with sharp margins localized to the dorsal aspect of the subdural space. (Image courtesy of Giuliano Lo Bianco, MD)
Subdural Contrast - Bilateral SpreadAdditionally, contrast injected into the subdural space may also spread with symmetric and bilateral linear patterns along the dorsal sac associated with a classic “tram track” pattern identifiable in AP view (Fig. 4) [11]. In the lateral view, the contrast can be visualized in thin linear columns traveling cephalad with contrast visible in the dorsal subdural space [9, 11].
Fig. 4
Anterior-posterior (A) and lateral (B) fluoroscopy with subdural spread of contrast with linear “tram track” pattern along the dorsal aspect of the subdural space. (Image courtesy of Giuliano Lo Bianco, MD)
Fascial SpreadThe contrast in the extradural space with fascial spread is localized with limited caudal or rostral spread and does not reach the medial pedicle, as is often readily identifiable in the AP view (Fig. 5). On the CLO view, the contrast will be dorsal to the VILL and localized to that region [9, 11].
Fig. 5
Anterior-posterior (A) and CLO (B) fluoroscopy with fascial spread of contrast localized dorsal to the VILL. (Image courtesy of Giuliano Lo Bianco, MD)
Retrodural Space of OkadaContrast spread into the retrodural space of Okada presents a very classic pattern in the AP view. The retrodural space of Okada is a potential space that communicates between the bilateral facet joins of a corresponding level and is often present with co-existing pars interarticularis defect (Fig. 6). When contrast is injected into this space, it demonstrates contrast spread at the facet joints bilaterally with communication facilitated by the retrodural space of Okada, and this finding can be readily identified on the AP view [12].
Fig. 6
Anterior-posterior (A) and lateral (B) fluoroscopy with contrast in the retrodural space of Okada with spread visualized with characteristic bilateral communication of fluid and contrast into the facet joints through the retrodural space of Okada. (Image courtesy of Giuliano Lo Bianco, MD)
Comments (0)