Benign leiomyoma of uterus malignant spinal metastasis at initial clinical presentation
Purpose
Benign metastatic lesions from Leiomyoma of uterus to spine are very rare and it is difficult to diagnose and management is a challenge in premenopausal women as there are no guidelines.
Methods
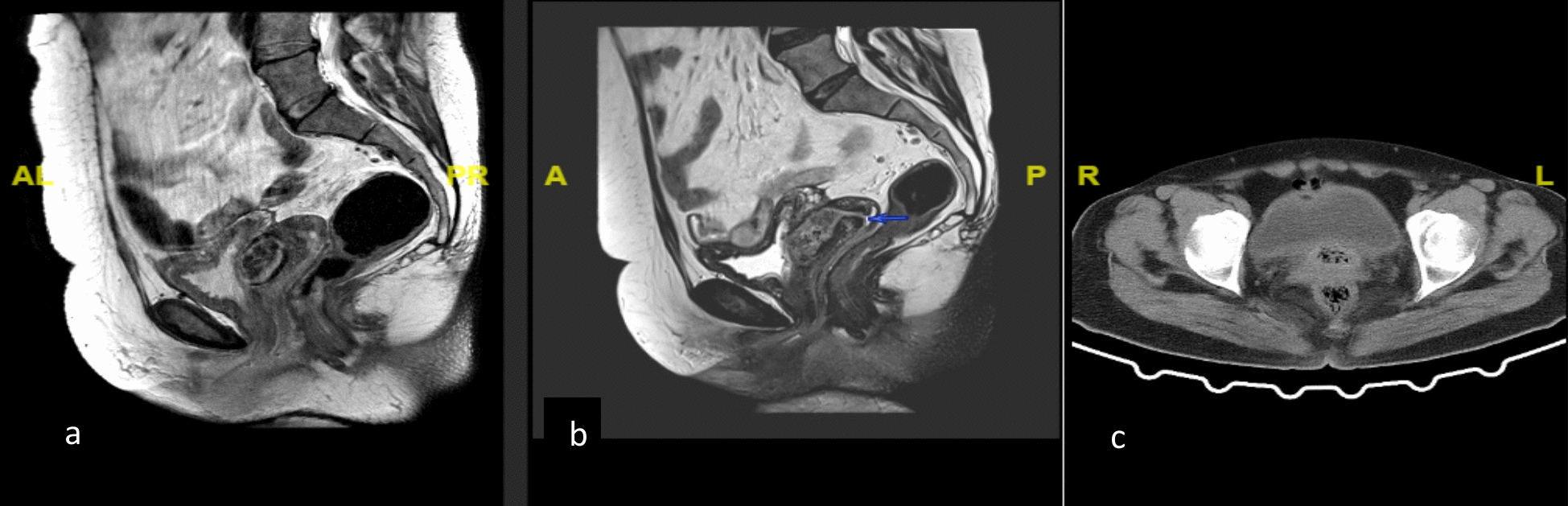
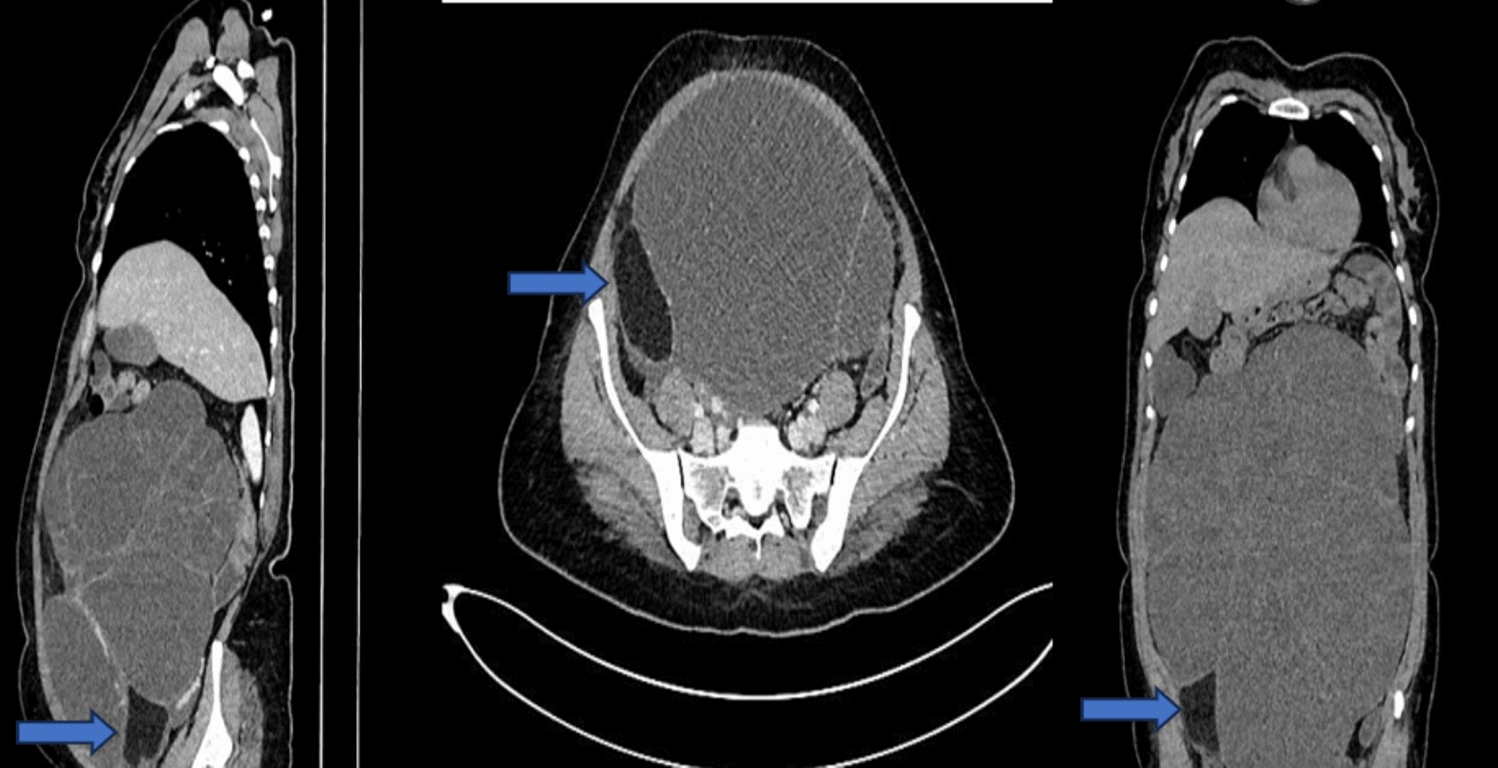
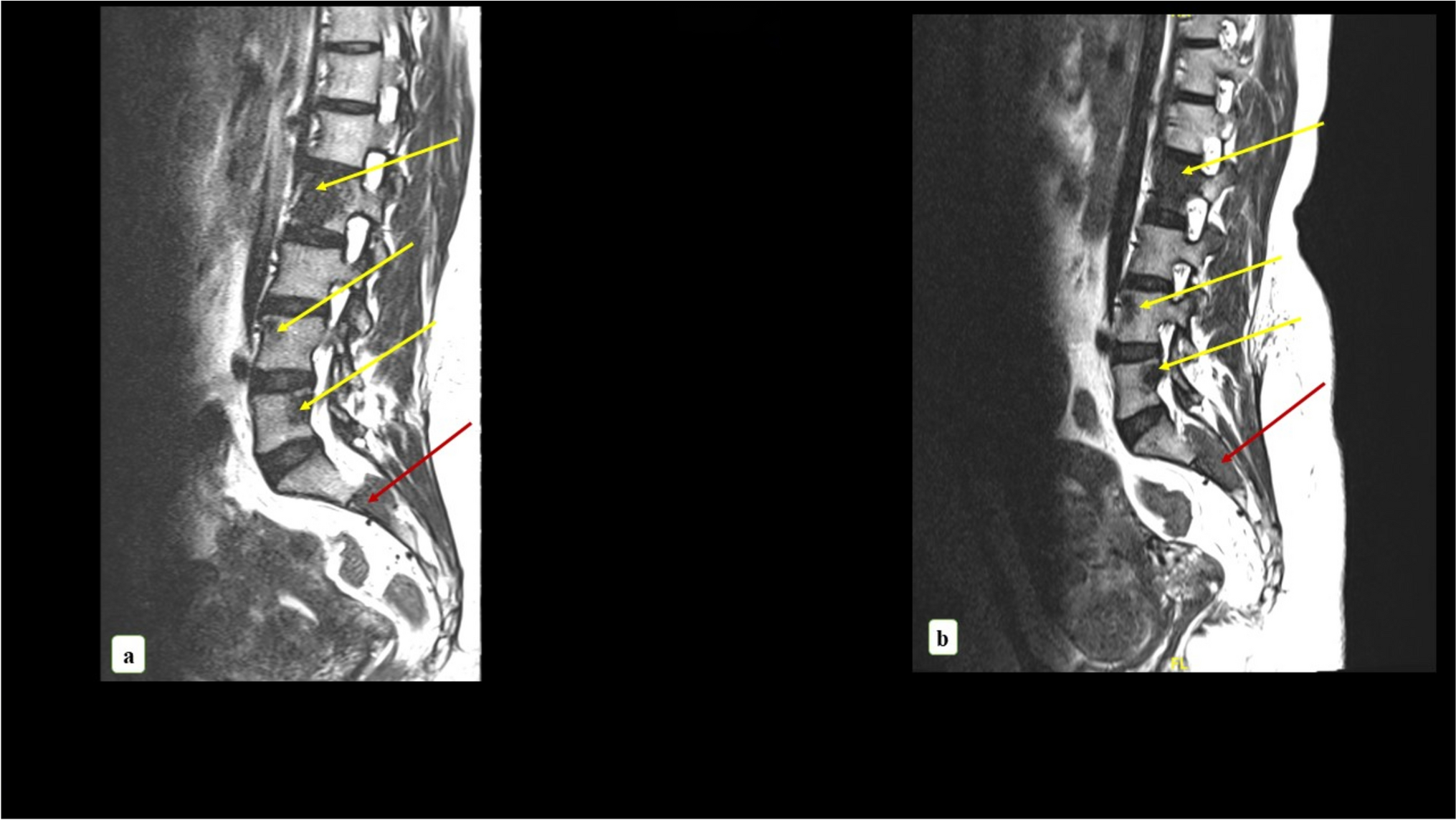
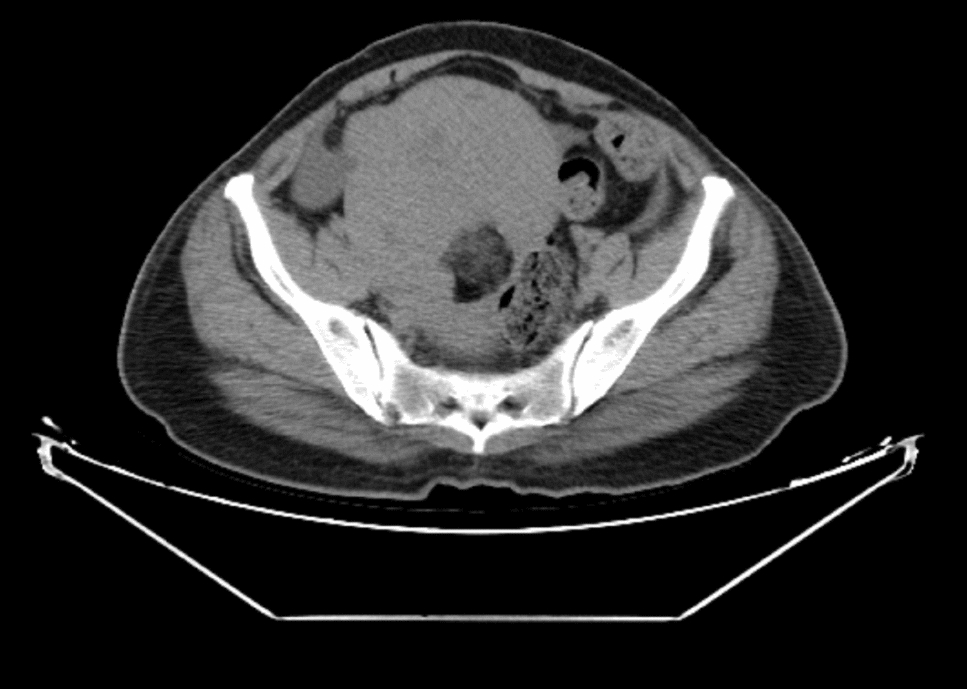
A 38-year-old multi-parous woman presented with low back pain and sciatica and neuromusculoskeletal problems and was evaluated after a year of symptomatic treatment by imaging. Three attempts of CT-guided biopsy of the sclerotic lesion of spine did not conclude the nature of the lesion except for spindle cells with minimal atypia. On further evaluation, contrast enhanced computed tomography of abdomen, pelvis and thorax showed multiple fibroids of uterus and few sub-centimetric pulmonary nodules. She was treated with three doses of GnRH analogues followed by Ulipristal acetate for three months during COVID times. Later she underwent total abdominal hysterectomy with bilateral salpingectomy and the Ovaries were retained due to young age though we had differential diagnosis of metastatic leiomyoma to spine. A repeat MRI showed an increase in the size of the S2 (second sacral vertebra) lesion causing foraminal narrowing and compression. Laminectomy and excision of the S2 lesion was undertaken. Results: The histopathology was suggestive of benign metastasizing leiomyomatosis. She received four cycles of GnRH analogues following surgery, and finally, due to intractable back pain laparotomy and bilateral oophorectomy was performed. A positron emission tomography-computed tomography scan revealed low-grade metabolically active lytic lesions and soft tissue components in the spine, lung, pleura, and diaphragm with indolent malignant aetiology. Her symptoms of intractable back pain and muscle weakness improved after anti-oestrogen therapy and spinal irradiation.
Conclusion
Multimodality therapy that creates hypo-estrogenic state is essential for achieving cure for spinal leiomyomatosis.


Comments (0)