Pathogenically, these tumors enmate from neuroendocrine cells within intestinal-type epithelium of mature cystic teratoma [1]. The insular/mucinous types and trabecular/strumal carcinoid are midgut and foregut or hindgut derivatives, respectively.
On gross, these tumors are usually unilateral and small (average size: 3.4 cm). Larger tumors (> 7 cm) are often associated with carcinoid syndrome and usually do not arise in the background of cystic teratoma [1]. The tumor is typically solid and rarely cystic. They can also form a nodule within a dermoid cyst. On cut section they are homogeneous yellow to tan, and may have glistening mucinous areas [1,2,3,4,5,6]. In the present case, however, the maximum tumor dimension was 12 cm and was seen associated with areas of mature cystic teratoma and was not associated with carcinoid syndrome.
Metastatic carcinoid in contrast to primary ovarian carcinoid, have larger size (mean 10.2 cm), usually bilateral, multinodular in appearance and not associated with teratomatous elements [10].
Approximately 57% cases are associated with cystic teratoma [11]. The most common histological variant include insular carcinoid (~ 50%) followed by strumal carcinoid (~ 40%). However, study by Kong S. et. al. on 56 cases of primary ovarian carcinoid showed strumal carcinoid to be most common (~ 66%) [6]. Rare cases of trabecular carcinoid and mucinous carcinoid have been reported. Insular carcinoid is more frequently associated with carcinoid syndrome [1,2,3,4,5,6,7].
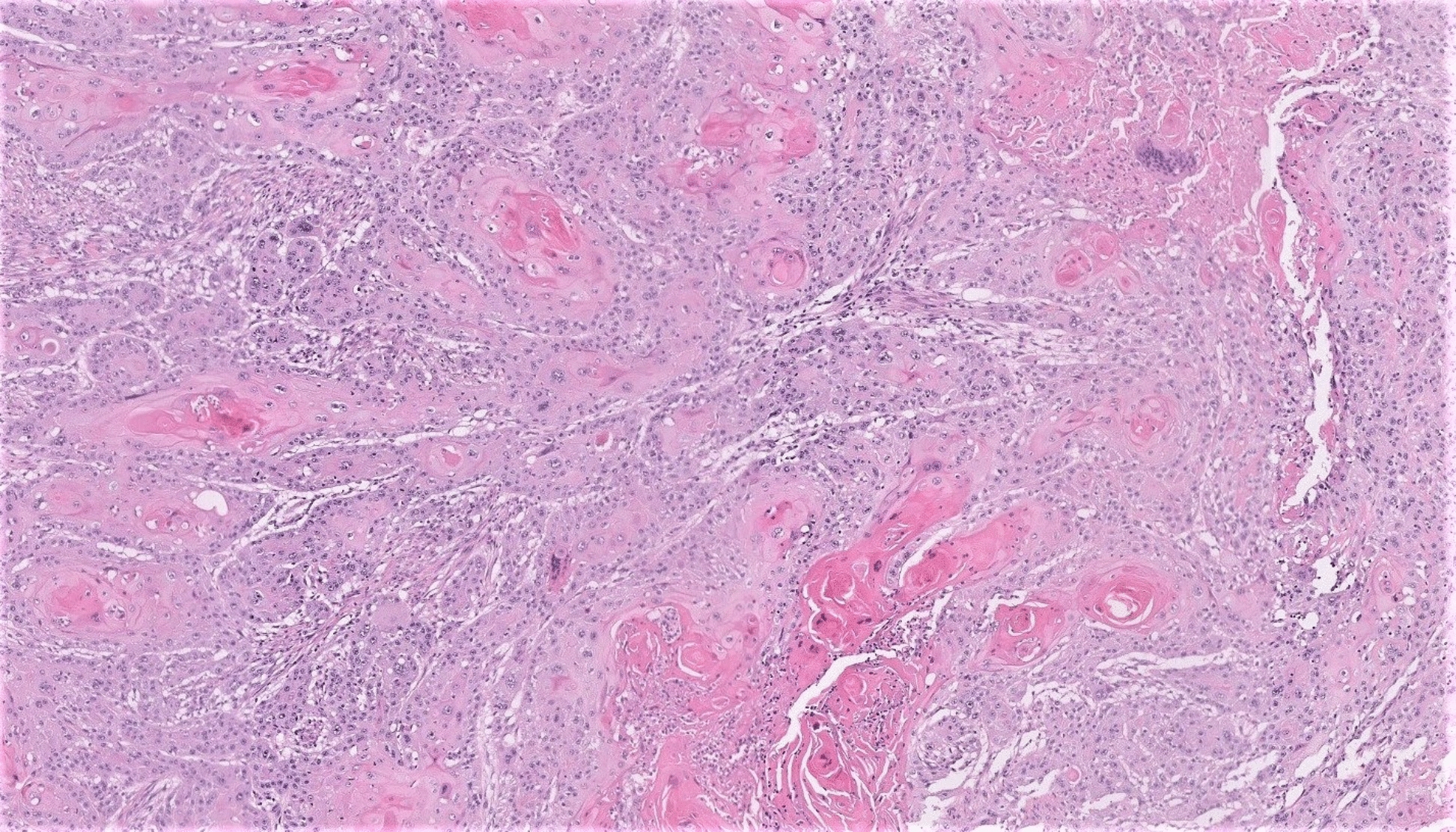
On microscopy, insular carcinoid is arranged in solid nests, acini, glands or tubules, whereas trabecular carcinoids are arranged in ribbons, cords, or trabeculae. Cells are uniform and have round to oval centrally located nuclei with salt-and-pepper chromatin and with eosinophilic cytoplasm. Reddish-brown argentaffin granules may be seen at the base. Strumal carcinoid in addition shows thyroid follicles. Gastrointestinal-type mucinous glands are seen in about 40% of cases. Well-differentiated mucinous carcinoid shows small glands/acini floating in pools of mucin, lined by goblet cells with compressed nuclei admixed with columnar cells, some showing neuroendocrine granules. Atypical carcinoid shows confluent growth, cribriform areas, and crowded glands. Carcinoma arising in mucinous carcinoid shows solid growth, single or signet-ring cells, severe cytological atypia, brisk mitotic activity, and mucin depletion. Teratomatous elements and fibromatous stroma may be seen in the ipsilateral or contralateral ovary [1,2,3,4,5,6,7]. The morphological differential diagnosis are discussed in Table 1.
Table 1 Possible morphological differential diagnosisOn immunohistochemistry, carcinoids are variably positive for neuroendocrine markers and CDX2 and are typically CK7 + and negative for CK20. Mucinous carcinoids are typically CK20 + . A study indicated CDX2 showed diffuse/focal expression in 90% metastastic carcinoid from gastrointestinal tract while weak positivity in 18.8% of primary ovarian carcinoids. Strumal variant will also be positive for TTF-1. Moreover, primary ovarian carcinoid have lower median Ki-67 index than metastatic carcinoids ( 2.3% versus 9.7%) [1,2,3,4,5,6,7]. The present case also showed a predominant insular pattern which is described as the most common variant by most of the authors. Ki-67 proliferation index was on a higher side 8–10% despite being a primary carcinoid.


Comments (0)