Exuberant Vulval Vestibular Papillomatosis (VVP): A Rare Enigma Treated with the Help of the “Workhorse” of Vulva Reconstruction—the V–Y Advancement Flap
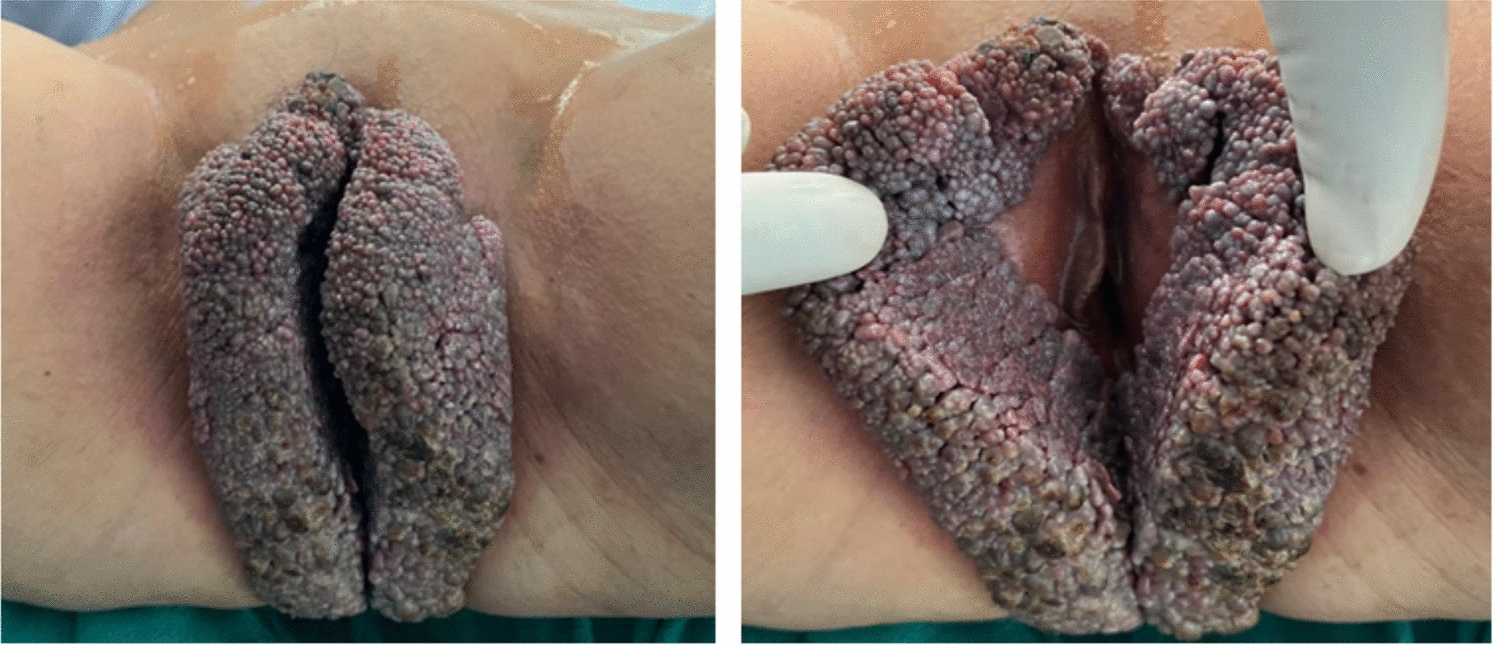
Vulval vestibular papillomatosis (VVP) is a rare entity described in the literature. Due to the diagnostic dilemma, they were also named as pseudocondylomata, hirsuties papillaris vulvae, hirsutoid papillomas of vulva, vestibular microwarts, micropapillomatosis and vulval squamous papillomatosis. [2] They are usually symmetrically distributed often as small [1–2 mm], shiny linear array of papules, are soft and have the same color as skin or the adjacent mucosa. Unlike warts, individual projection bases remain separate and they characteristically do not show acetowhite areas on the application of 5% acetic acid, unlike warts. [3].
A common misconception of VVP is that human papillomavirus (HPV) is a causative factor. While The incidence of HPV was shown to range from 12 to 77% in earlier studies [3, 4] however this has been refuted in multiple studies by the HPV polymerase chain reaction or in situ hybridization test. [5, 6] A common source of discrepancy in this regard is attributed to the finding of vacuolated cells resembling koilocytes in histology slides. This can be explained by the fact that heavily glycogenated epithelial cells on processing get vacuolated and resemble koilocytes. [1, 7].
When planning for resection of large vulval lesions be it benign or malignant the possibility of need for vulval reconstruction should always be borne in mind. The primary aim of vulval reconstruction is to achieve tension-free closure and decrease the amount of scarring both in the donor and receipt sites. The secondary objectives include the preservation of sensation and sexual functioning. [8] The various methods to achieve vulval reconstruction include the use of skin grafts, local flaps or myocutaneous flaps based on gracilis, tensor fascia lata or rectus abdominis. The advantage of fasciocutaneous flaps over myocutaneous flaps is the former flaps are less bulky and thereby cause less of a ghastly scar on the donor site.
In the late 1990s, numerous fasciocutaneous flaps were introduced due to the more detailed knowledge about the perineal blood supply from the internal pudendal artery. The V–Y advancement flap either from the medial thigh or gluteal fold gained widespread popularity and is based on the suprafascial vascular plexus from superficial and deep femoral arteries and the superficial perineal artery Viz. the terminal branch of the internal pudendal artery. [9] Moreover these flaps are thin, reliable, similar skin quality and colour as the vulval skin, can be sufficiently advanced to achieve tension-free repair, are well hidden by the gluteal fold and are covered by undergarments making them an ideal choice. The flaps also maintain sensation by the posterior cutaneous nerve of the thigh and the pudendal nerve. Another advantage of V–Y flaps is that they can be raised bilaterally and are reliable even in post-radiotherapy cases as they depend on a network of blood vessels rather than a single perforator artery. This translates to a decreased incidence of full flap necrosis(< 5%) and the need for additional surgery for scar correction or flap debulking. These advantages have been proved in studies done by Zhang et al. and Tock et al(10, 11).
The novelty of the case report lies in the rare reporting of VVP and repair of the large vulval defect by a bilateral V–Y flap. Clinicians should be aware of this benign condition and need to keep this differential diagnosis in mind when dealing with atypical presentations of warts to correctly treat patients.


Comments (0)