Ethical Statement and Considerations
The study was Institutional Review Board (IRB) approved from Northern Arizona University (NAU IRB 1487466–1). Given the history of exploitative and unethical research, it was essential for researchers, including those of NA descent, to conduct the study ethically [16]. The educational intervention was culturally tailored, incorporating cultural relevance, sensitivity, and input from the community. The information provided about cancer and HPV was made pertinent to the local NA community, addressing associated health disparities while avoiding stigmatization. The focus of the intervention was on sensitive communication and empowering individuals to learn about cancer, HPV, and related recommendations through storytelling via vignettes. This method respected the traditional communication style used by NAs and aimed to avoid highlighting the negative experiences and statistics often associated with these topics. Additionally, the cultural practice of the presenter sharing a personal familial experience with cancer and identifying as a Native individual can help to establish trust, familiarity, and rapport with the participants from the beginning of the study.
The study recognized the historical mistrust surrounding medical research by being transparent from the start of the study. Participants were provided with information about study’s objectives, which included educating healthcare professionals and community workers about HPV and the vaccine. In addition, the study provided healthcare workers with the latest recommendations on HPV and their implications for NA women, as well as shared recent findings on HPV and its significance for this population. Furthermore, the study communicated how the findings could be applied in the future to enhance rates of screening and cancer prevention programs in Native communities. Importantly, there were no additional risks for participants associated with the addendum, and it was consistently emphasized that participation was voluntary.
Study Design
The educational intervention study was modeled after a previous study, that analyzed knowledge of HPV and participant attitudes [13]. Therefore, the pilot study expanded the findings as part of the requirements for a Master of Public Health internship at the University of Arizona. The study included a 45–60-min in-person and online PowerPoint presentation, along with a pre-and post-electronic survey to assess participants’ knowledge and attitudes regarding HPV, the HPV vaccine, and HPV-related diseases (such as cancers and warts). Three vignettes were also presented, each with two prompts to measure participants’ responses using a 5-point Likert scale (Supp. Table 1). Initially, two in-person presentations were scheduled for January 2020. However, due to the global COVID-19 pandemic, the in-person sessions were canceled. An IRB addendum was requested and approved to allow presentations to be delivered via Zoom®.
Study Participants
The inclusion criteria for study participants were individuals aged 18 years or older, from any racial or ethnic background, regardless of gender, and holding community roles such as college students, healthcare providers (including MD, PAs, and nurse), healthcare center staff, health educators, social workers, and community workers relevant to serving NA populations (referred to as “Other” in this study).
Recruitment Strategy
Participant recruitment involved sending emails to four local organizations: The Partnership for Native American Cancer Prevention (NACP), Northern Arizona University (NAU) Applied Indigenous Studies class, Native Americans for Community Action (NACA), and North Country HealthCare (NCHC). These organizations serve NA populations. The emails explained that the purpose of the study was to educate healthcare providers and community workers about HPV and the vaccine, considering the existing disparities in cervical cancer rates within these communities [6]. Additionally, the emails encouraged healthcare providers and other healthcare staff members to participate in the study.
Surveys
The electronic surveys were administered using Poll Everywhere®, an interactive platform that enables real-time feedback during PowerPoint presentations. Participation in the survey was optional, and responses were anonymous. No personal information, such as cellphone numbers or other digital identifiers, was collected. Participants were able to answer the survey questions using their personal devices through a provided Poll Everywhere® link or code. For those who could not use an electronic device, a paper version of the survey was available as an alternative to ensure maximum voluntary participation (n = 15). Both in-person and online presentations facilitated data collection through the survey embedded within the PowerPoint presentation. By participating, individuals consented to have their responses used in future publications and/or presentations.
Vignettes
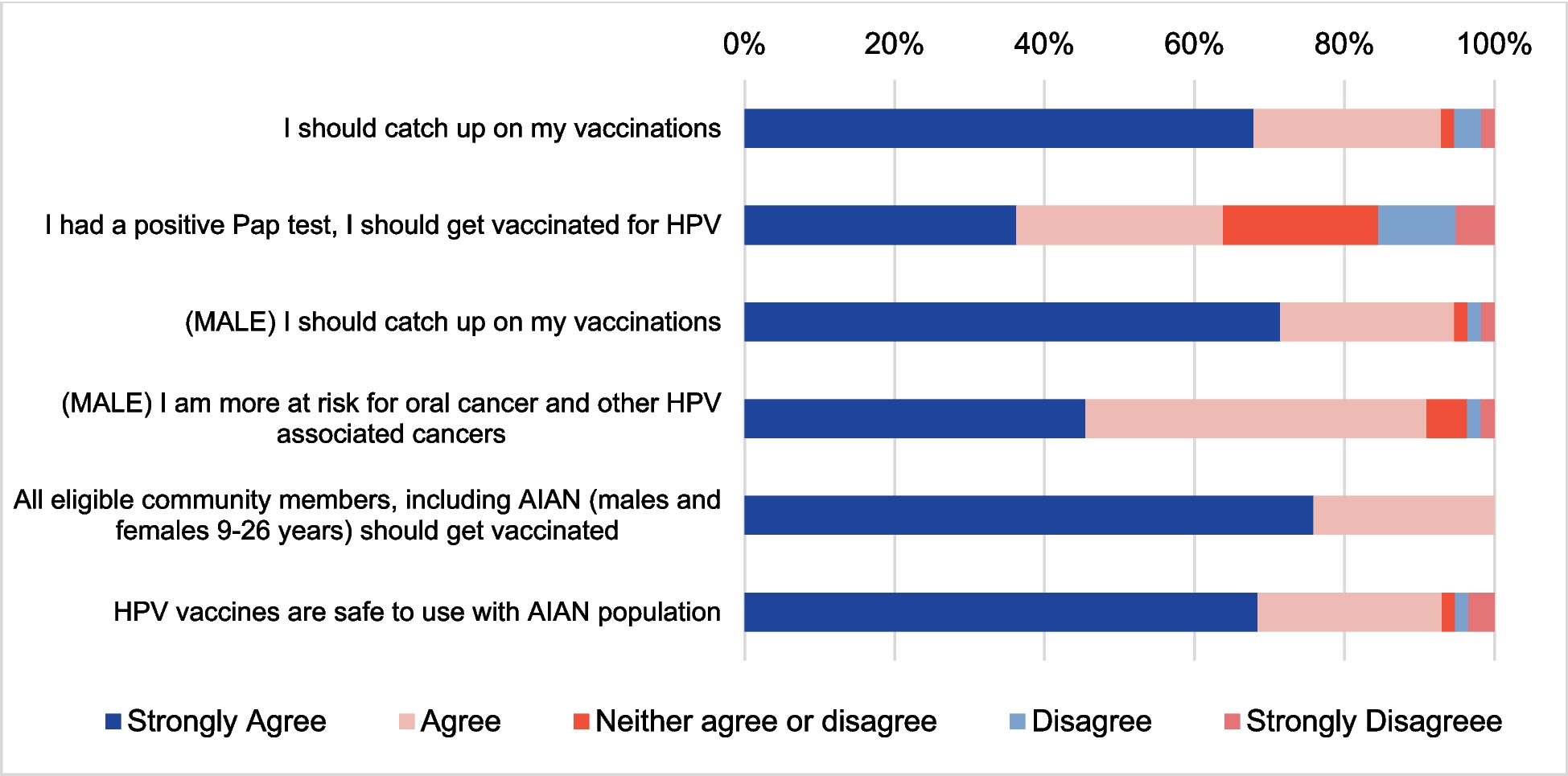
Three narrative-style vignettes, along with statements utilizing a 5-point Likert scale (strongly agree, agree, neither agree nor disagree, disagree, and strongly disagree) were used to assess participants’ attitudes toward HPV and the vaccine. These vignettes presented relatable and understandable stories, engaging participants effectively [17]. Throughout the presentation, the vignettes were accompanied by questions regarding knowledge. Vignettes provide a means to explore actions within context, clarify people’s judgments, and offer a less personal and less threatening approach to discussing the HPV vaccine. They also align with the traditional communication styles of many NA communities, using oral and visual storytelling methods that are both familiar and effective. Additionally, vignettes present a third-party perspective, which can be beneficial when discussing sensitive subjects like cancer or other difficult topics [17].
Pre-/Post-Survey Questions
The survey consisted of seven TRUE/FALSE statements designed to evaluate participants’ knowledge of HPV, the vaccine, and HPV-related diseases or infections. Participants completed both pre-and post- survey questions to measure the knowledge they gained during the presentation. Educational content was provided after the pre-survey questions to help assess learning outcomes in the post-survey.
Statistical Analysis
Data from organizations and partnerships were combined, and descriptive statistics, including frequencies and percentages, were calculated. Participant attitudes toward HPV and the HPV vaccine were visually analyzed using stacked bar charts. The percentages of TRUE and FALSE responses in the pre- and post-surveys were compared to determine which group had a higher proportion of correct responses. A greater proportion of correct responses indicated that the educational intervention had some measurable effect on knowledge gained. All data analyses were performed using MS Excel.


Comments (0)