
Remember me







Consecutive RIRS procedures between 2010 and 2023 were retrospectively reviewed from the RIRSearch study group database. Patients with ureteral stents prior to RIRS, patients younger than 18 years of age, patients who had a history of pelvic radiotherapy or non-ureteral pelvic surgery, and patients in whom there was no attempt to insert a ureteral access sheath (UAS) during RIRS were excluded from the study. Retrieved demographic variables were age, gender, body mass index (BMI), age-adjusted Charlson Comorbidity index (CCI), and history of previous ipsilateral ureteral intervention. Clinical data collected included side of surgery, serum creatinine level, stone density in Hounsfield units (HU), stone burden, presence of hydronephrosis, stone number and stone location. Surgical and complication data were the requirement for active ureteral dilatation (coaxial or balloon dilatators or optical dilatation using ureteroscope), the UAS size used in both successful and unsuccessful placements, JJ stent insertion at the end of the RIRS, the type of flexible ureteroscope employed, the fluoroscopy time, the hospitalization time and perioperative and early postoperative (˂30 days) complications. Perioperative and postoperative complications were evaluated according to the Modified Satava Classification (MSC) and Modified Clavien Classification (MCC) systems, respectively. Finally, surgical success or failure data were obtained from the follow-ups after RIRS procedures. Surgical failure criterion was defined as a residual stone of 4 mm or more in non-contrast computed tomography (CT) taken within 1–3 months of the RIRS procedure [5,6,7,8,9,10]. To access the upper urinary tract any additional ipsilateral intervention session after RIRS was denoted as an auxiliary procedure.
Patients included in the study who did not have a history of ipsilateral ureteral intervention were categorized as “virgin ureter”. Patients who had a history of any endoluminal/intrinsic intervention (history of antegrade or retrograde stent placement in any urological procedure such as percutaneous nephrolithotomy or pyelolitotomy, and/or history of ureteroscopy) or extrinsic surgery (ureterolithotomy, ureteroneocystostomy) for the ipsilateral ureter were categorized as “non-virgin ureter”. Those two groups were compared in terms of demographic, clinical, and RIRS outcome (surgical success and complications) before and after the case-control matching approach. In order to further evaluate the renal collecting system complexity of patients requiring second RIRS session due to residual stones, the infundibulopelvic angle (IPA) was also measured with non-contrast CT in non-virgin ureter group, as previously described [11]. This study was conducted after approval by the ethics committee of Kocaeli University School of Medicine (Approval No.: GOKAEK-2025/02/01).
Case-control matchingTo reduce the risk of bias and potential confounding factors, we adopted a case-control study design procedure of Statistical Package for the Social Sciences (SPSS) version 19.0 software (IBM Corp., Armonk, NY, USA). The non-virgin group was individually matched at a ratio of approximately 1:2 to patients with virgin ureter using an optimal matching approach based on confounders, including age (within 4 years), gender, UAS size used or attempted (≤ 10–12 Fr and 11–13 Fr≤), stone location, stone volüme (within 300 mm3), stone density, and stone number. After adjusting for confounders, the groups were compared in terms of demographic, clinical, surgical, complication, and success data.
Surgical procedureAll patients undergoing RIRS had a negative urine culture prior to the procedure. Non-contrast CT was used for the diagnosis of patients before RIRS. Consent forms were obtained from all patients prior to RIRS. RIRS procedures were performed under general anesthesia and in the lithotomy position. The surgical procedure was preceeded by cystourethroscopic examination, the insertion of a Sensor™ guide (Boston Scientific, USA) into the ureter, the demonstration of upper tract anatomy using retrograde pyelograpy, and the placement of a UAS over the sensor guidewire. The UASs employed in this study were Flexor® (Cook Urological, Spencer, IN, USA), Bi-FlexTM (Rocamed, Monaco), and Navigator® HD (Boston Scientific, Marlborough, MA, USA). Ureteral dilatation was performed using balloon (UroMax UltraTM, Boston Scientific), coaxial dilator (8–10 F, Boston Scientific) or optical dilatation with ureteroscope (8/9.8 F ureteroscope, Richard Wolf medical instruments Knittlingen, Germany; or 8–9 F, Karl Storz, Rietheim-Weilheim, Germany) before or after UAS placement, based on surgeon’s preference. Detailed ureteral dilatation approaches have been described in previously reported studies by the RIRSearch group [8, 9, 10, 12]. Despite lower ureteral dilatation if UAS could not be inserted, a flexible ureteroscope (fURS) was inserted into the upper urinary tract with a backloading approach over the guidewire. The fURSs used in RIRS procedures were Karl Storz Flex-X2 (Karl Storz, Tuttlingen, Germany), WiScope® (OTU Medical Inc.), and Uscope UE3022 (Pusen™). A Ho: YAG laser was used for laser lithotripsy. Energy pulse frequency and power were adjusted according to stone hardness and burden. Stones larger than 2–3 mm were removed from the body with a nitinol-coated basket [8, 9, 10, 12].
StatisticsCategorical variables are expressed as count/frequency (n) and percentage (%). To assess the normality hypothesis for the continuous variables, the Shapiro–Wilk test was used. Continuous variables are presented as mean ± standard deviation (SD) or median and interquartile range (IQR); analyzed with independent samples t test or Mann Whitney U test as appropriate. Categorical variables were evaluated using the Chi-square test and Fisher exact test. Univariate analysis by binary logistic regression analysis was performed to evaluate whether the risk of complications and auxiliary interventions in the non-virgin ureter group compared to the virgin ureter group after case-control matching. All statistical analyses were conducted using SPSS version 19.0 software (IBM Corp., Armonk, NY, USA). A p < 0.05 was considered statistically significant.
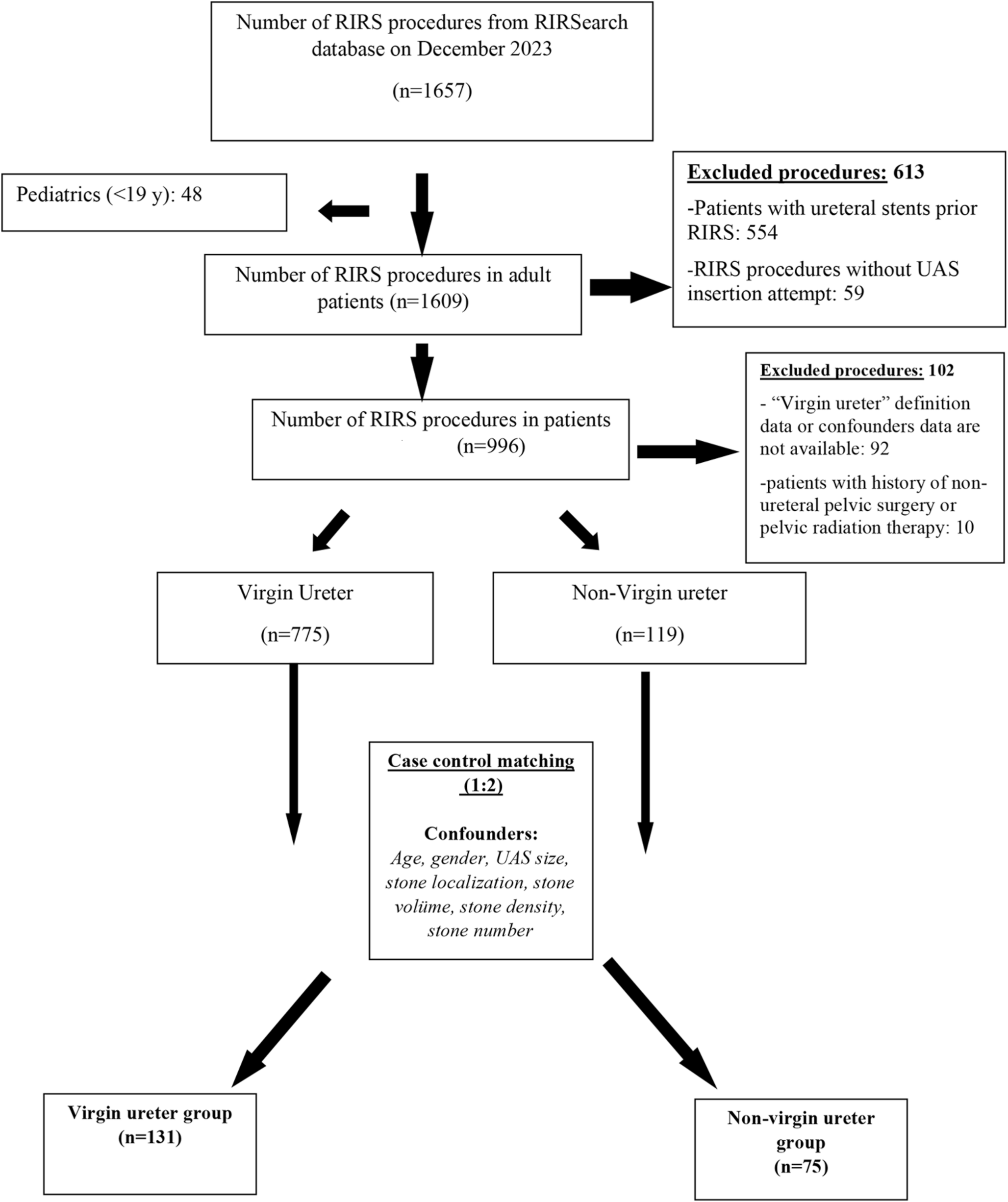
ResultsA total of 894 procedures in 819 patients that met the inclusion criteria were included in the study. The mean age of patients was 47.2 ± 13.6 years, the proportion of male patients was 61.6%, and the median CCI was 1 (0–1). RIRS procedures were performed by five different surgeons (CMY: 619, HC: 187, KT: 36, MFŞ: 17, EBS: 35). The “non-virgin ureter” group consisted of a total of 119 (13.3%) procedures (Fig. 1). Of the patients in the “non-virgin ureter” group, 84 (70.6%) had a history of only one ureteroscopy, 25 (21%) had two or more ureteroscopies, 10 (8.4%) had a history of antegrade or retrograde ureteral stenting (2 in percutaneous nephrolithotomy procedures, 3 in pyelolithotomy procedures, and 5 in retrograde DJ stenting for obstruction). There was no patients with extrinsic surgery for ipsilateral ureter based on study protocol. There was no case of failed ureteroscopy due to uncompliant or strict ureters among virgin group and non-virgin ureter group.
Fig. 1
Flowchart of the study population selection and case control matching for the virgin and non-virgin groups
Before case-control matching, mean age (50.6 ± 13.2 vs 46.6 ± 13.6 years) and the rate of patients with CCI > 1 (51.3% vs 40.4%) were significantly greater in the “non-virgin ureter” group (p < 0.05). In the “non-virgin ureter” group, the multiple stone rate (56.3% vs 35.6%), total stone volume (895.2 (284.3-2441.3) vs 503 (205.5-1049.8) mm3) and multifocal stone location rate (54.6% vs 30.7%) were significantly higher compared to the “virgin-ureter” group (p < 0.05). Moreover, the operation time (81.7 ± 36.2 vs 65.8 ± 35.6 min), hospital stay (1.74 ± 1.75 vs 1.50 ± 1.72 days), perioperative complication rates (17.6 vs 6.5%), auxiliary treatment requirement (31.1 vs 8%), and surgical failure rate (47.9% vs 20.8%) were significantly greater in the “non-virgin ureter” group (p < 0.05). There was no further statistical difference between the groups in terms of demographics, clinical, surgical, and complication data.
A hundred and thirty-one patients from the “virgin ureter” group and 75 patients from the “non-virgin ureter” group (1:2) were matched using a case-control method in terms of age, gender, total stone volume, stone location, stone density, number of stones and similar UAS use (≤ 10–12 Fr and 11–13 Fr≤). Of the 75 with non-virgin ureter, 53 (70.7%) had one and 17 (22.7%) had more than one ureteroscopy, whereas 5 (6.7%) had only undergone ureteral stenting. After matching, apart from demographic and clinic data, the UAS usage, and the UAS insertion failure rate, the lower ureteral dilatation rate, the fluoroscopy time, and the surgical time were also similar between the virgin and non-virgin ureter groups (p > 0.05). Moreover, there was no significant difference for the postoperative complication rates (17.3% for non-virgin ureter group vs. 19.8% for virgin ureter group) and the surgical failure rates (36% for non-virgin ureter group vs. 26% for virgin ureter group) (p > 0.05). However, when the perioperative complication rate (18.7% vs. 5.3%), hospital stay (1.54 ± 1.30 vs. 1.18 ± 0.98 days) and auxiliary treatment requirement rate (20% vs. 8.4%) were compared, these were significantly worse in the “non-virgin ureter” group compared to the “virgin ureter” group (Table 1).
Table 1 Comparison of demographic, clinical, operative and postoperative data of patients in the “non-virgin ureter” and “virgin ureter” groups who underwent retrograde intrarenal surgery before and after case control matchingThe details of the perioperative and the postoperative complications in non-virgin and virgin ureter groups undergoing RIRS are presented in Table 2. All of the perioperative complications in the non-virgin ureter group were an inability to reach the stone that was graded by MSC as grade 2b (14 of 75, 18.7%). All of these 14 patients were considered to have failed RIRS procedures due to residual stones that could not be reached. This complication rate was significantly lower in the virgin ureter group compared to non-virgin ureter group (4.6% vs. 18.7%, p < 0.05. There were 6 patients in the virgin ureter group who underwent the second session RIRS procedure as an auxiliary treatment because the stone could not be reached. The elapsed time to the auxiliary treatment from first RIRS procedure was 132.8 ± 216.5 days and the surgical success rate in these 6 patients was 83.3%. Moreover, 13 of these patients in non-virgin ureter group who had failure of initial RIRS and accepted auxillary treatment underwent a second RIRS session after a mean of 51.7 ± 23.2 days, and two patients from the non-virgin ureter group who had stent migration underwent stent removal using ureteroscopy under general anesthesia. Thus, the rate of auxiliary procedure (a second endoscopic session) was significantly lower in the virgin ureter compared to the non-virgin ureter group (4.6% vs. 17.3%, p < 0.05, Table 3). It was noteworthy that the stone localization of 13 patients who underwent second RIRS session was predominantly in the lower calyx and surgical success was achieved in only 6 of these procedures (46.2%). Of 13 patients, 6 was male and median age was 53 (44–59). In order to assess the complexity of lower caliceal anatomy, the IPA values were also calculated in non-virgin ureter group and median IPA level of these 13 procedures was 32 (29–39). Minor (Grades 1 and 2) and major (Grades 3-4b) postoperative complications (MCC system) were similar between the patients with virgin and non-virgin ureter (p > 0.05).
Table 2 The classifications of perioperative and postoperative complications by the modified SATAVA and the modified clavien classifications systems in patients with Virgin ureter and non-virgin ureter who underwent retrograde intrarenal surgeryTable 3 Auxiliary surgical treatments following case controllingAfter case-control matching (n = 206), the perioperative complication risk and the auxiliary treatment requirement risk were compared in the non-virgin ureter group and the virgin-ureter group in terms of detail of the history of ureteral intervention. The ureteroscopy history (n = 70), one of the endoluminal/intrinsic etiologies of non-virgin ureter gave rise to a significant increase in the perioperative complication risk (OR: 4.59, 95% CI: 1.75–12.01) and the auxiliary intervention requirement risk (OR: 3.12, 95% CI: 1.34–7.25) compared to virgin ureter (n = 131) (Fig. 2). Antegrade or retrograde ureteral stenting (n = 5) did not increase the perioperative complication risk or the auxiliary procedure requirement risk (p > 0.05).
Fig. 2
Schematic draw the virgin- and non-virgin ureteral concept (A). Intrinsic and extrinsic factors that can be associated the loss of ureteral virginity (B). Assessment the risk of Peroperative complications during Retrograde Intrarenal Surgery between patients with virgin ureter and patients with non-virgin ureter (C). Assessment the risk of auxiliary treatment requirement after Retrograde Intrarenal Surgery between patients with virgin ureter and patients with non-virgin ureter (D)
Comments (0)