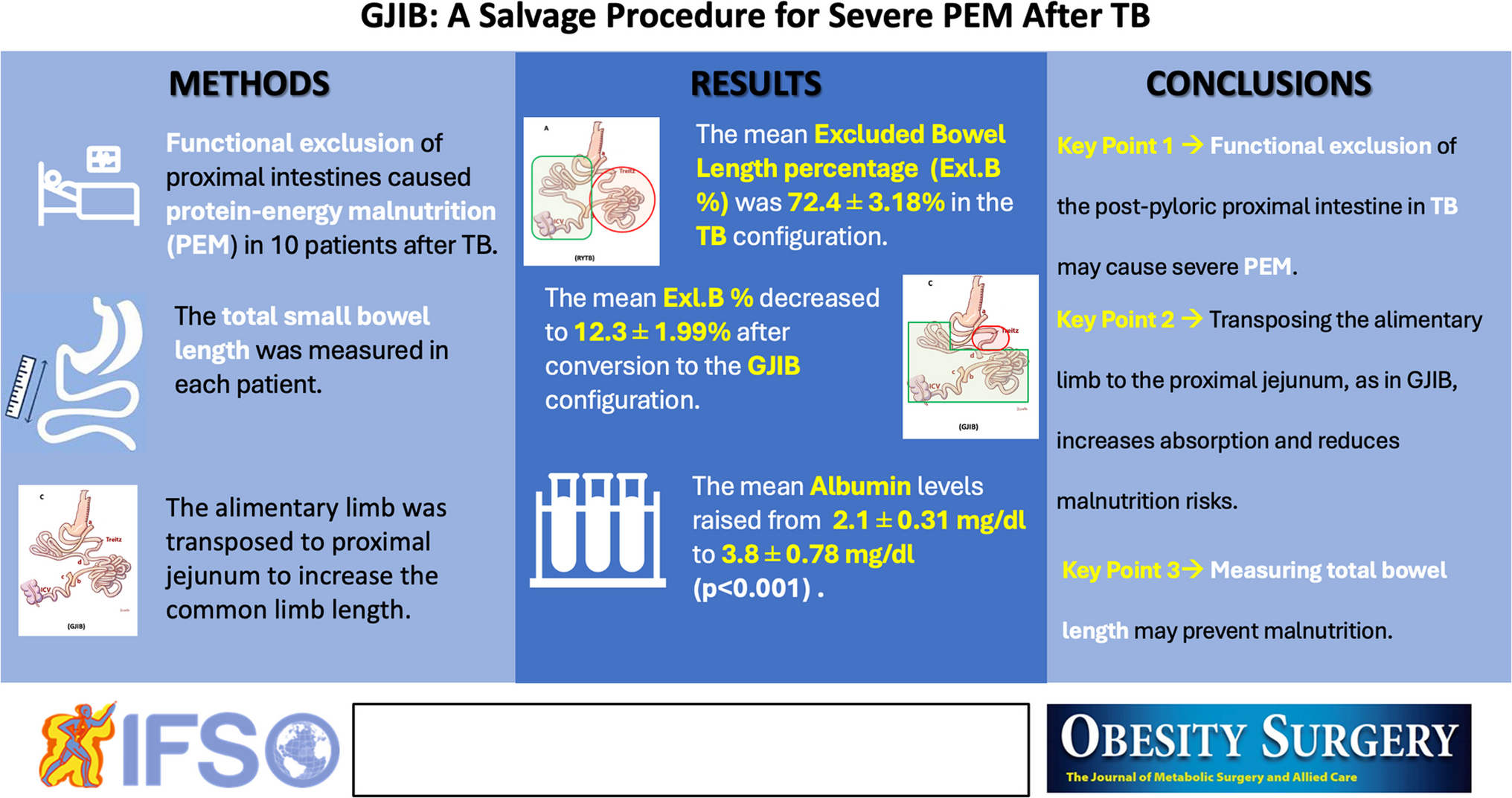
This study introduces a novel surgical technique to address protein-energy malnutrition (PEM) and intractable diarrhea following Transit Bipartition (TB). Patients experiencing persistent malnutrition, hypoalbuminemia, and excessive weight loss despite conservative management underwent conversion to Gastro-Jejunal Ileal Interposition (GJIB). This approach reintegrates functionally excluded small bowel segments while preserving the metabolic benefits of bipartition.
PEM after TB is rare but has been reported in a few cases, often associated with excess weight loss and diarrhea [3,4,5]. The etiology of these complications has been reportedly linked to excessive nutrient bypass due to a dominant new gastric outlet (wide gastroileostomy) [3, 4] or a short alimentary limb following the anastomosis [5], leading to accelerated transit and reduced absorption. While studies indicate that GIA diameters vary widely from 2.5 to 6 cm in diameter, the precise role of anastomotic size in malabsorption remains controversial [2, 7,8,9,10,11]. The details on the limb lengths, gastroileostomy anastomotic diameters, and staplers used in the other reports are summarized in Table 5 [2,3,4,5,6, 8,9,10,11,12,13,14,15,16,17,18,19].
Table 5 A summary of the operative details of previous reportsOur gastric emptying scintigraphy demonstrated that food predominantly traversed the anastomotic route in symptomatic and asymptomatic patients with similar anastomoses. This suggests that it is not the size of the gastroileostomy anastomoses that leads to PEM and diarrhea but the excessive exclusion of the unknown length of the proximal bowel in some patients.
Total bowel length (TBL) variations significantly impact outcomes following bariatric surgery, influencing weight loss and nutritional status [20]. The length of bypassed intestinal segments is crucial in determining postoperative efficacy and complications, as demonstrated in RYGBP and one anastomosis gastric bypass [21]. Stool alterations, including severe diarrhea, excessive flatulence, and foul-smelling stools, frequently occur after malabsorptive surgeries, requiring treatment or revision in cases where PEM becomes life-threatening [22, 23].
A key factor contributing to variability in surgical outcomes is the broad range of TBL among individuals, which exceeds previously assumed norms. Studies assessing anthropometric parameters and TBL have identified extreme differences, with patient TBLs ranging from 205 to 1049 cm [24, 25]. Tacchino et al. [24] found that 20% of patients had TBLs below 400 cm or above 800 cm, which could impact common limb length and influence weight loss and nutritional stability following RYGBP.
Eagleston and Nimeri [21] simulated different bariatric surgery scenarios using standard limb lengths in patients with varying TBLs of 500 cm, 700 cm, or 900 cm. Their findings demonstrated that some patients developed PEM, while others failed to meet weight loss expectations based on their TBL and procedure type. These variations highlight the necessity of individualized surgical planning to optimize patient outcomes and minimize complications.
An essential aspect in the planning of this revisional surgery is to decide whether to preserve bipartition and beneficial metabolic effects or convert to a sleeve gastrectomy. Preserving metabolic effects is important because disconnecting the ileum from the stomach eliminates early ileal stimulation, reducing hormonal benefits that enhance glucose metabolism and weight control. Converting TB to a sleeve gastrectomy reverses the anatomical changes responsible for TB’s metabolic benefits and is expected to increase the likelihood of weight regain and metabolic decline. In contrast, by restructuring proximal bowel segments, GJIB significantly enhances absorptive capacity, restoring protein and micronutrient levels without compromising metabolic control. Another advantage of GJIB is its maintenance of endoscopic access as in all bipartition techniques, unlike duodenal switch procedures that eliminate upper gastrointestinal endoscopic access.
Almahmeed, Pomp, and Gagner [26] had to revise two patients for developed significant malnutrition, who had undergone duodenal switch (DS) as the primary surgery as they had BMIs greater than 50. Both patients suffered from severe weight loss (WL), diarrhea, and PEM. The nadir BMIs of the patients prior to revision were 25 kg/m2 (representing 81 kg of WL) and 21 kg/m2 (representing 88 kg of WL), respectively. They both underwent partial common limb elongations as a first step, which did not halt further weight loss and PEM. Ultimately, both patients had ileal interpositions, one to the duodenum and the other to the proximal jejunum (30 cm from the Treitz ligament), significantly enhancing the intestine’s absorptive capacity. However, both patients regained a limited amount of excess weight while maintaining a significant portion of their weight loss, with BMIs rising to 29 kg/m2 [26].
In comparison, the average BMI of our patients increased from 22.29 to 28.16 kg/m2, preserving the metabolic and weight loss effects of the Transit Bipartition (TB) on one hand while improving PEM and hypoalbuminemia on the other.
Dapri [27] also reported a total reversal of one DS patient for intractable PEM and diarrhea, with a total weight loss of 78.5 kg and a BMI decrease from 54 to 24.5 kg/m2. He deconstructed duodenoileostomy and re-anastomosed the duodenal stump with post-pyloric duodenum, reconfiguring a normal antro-pyloro-duodenal passage, and completing with an ileo-ileostomy, re-establishing the original intestinal anatomy. This patient had retained only the sleeve component and lost the hindgut stimulation while correcting malabsorption. This is a perfect example of how the results of a sleeve-alone procedure will be markedly different from a sleeve plus ileal interposition. This patient gained 47.5 kg in 6 months, and her BMI rose to 42 kg/m2. This is significantly different from our patients’ weight regain levels. In their case, Almahmeed, Pomp, and Gagner [27] also did not experience such weight regain in which they interposed the ileal segment to the duodenum, enabling the food to traverse the whole length of the small bowel. These authors also emphasized that there wasn’t a greater weight regain despite the loose sleeve pouch [27]. Various other authors also proposed and used ileal interposition to correct severe PEM related to malabsorption [28, 29].
Our results are consistent with previous reports regarding the reversal or revision of duodenal switch surgeries for severe protein-energy malnutrition (PEM) and diarrhea related to malabsorption. Post-revision outcomes in our study support the effectiveness of transposing the ileal segment proximally as in GJIB. After surgery, the excluded bowel length decreased from 72.4 to 13.4%, reinforcing the role of bypassed intestinal length in PEM pathogenesis. Albumin levels rose from a median of 2.7 to 3.9 mg/dL, indicating a significant improvement in protein absorption. In contrast, BMI increased from 22.29 to 28.16 kg/m2, signifying effective weight stabilization while maintaining metabolic improvements.
Converting the TB to a sleeve in patients with PEM and excess weight loss corrected the malnutrition and diarrhea; however, none of the authors mentioned these patients’ metabolic and weight loss outcomes in their reports [3,4,5]. Unlike total anatomical reversal, which may cause complete metabolic regression and weight regain [27], we preferred to perform GJIB, which selectively restores absorption without negating bipartition effects, aligning with the previous experiences. This selective restoration of absorption was pivotal for achieving optimal patient outcomes.
In conclusion, though rare, the occurrence of PEM following TB highlights the importance of total bowel length and its effect on nutrient absorption. While a simple reversal to sleeve gastrectomy may seem like a straightforward solution, it comes with the risk of metabolic deterioration and possible weight regain. GJIB represents a more sophisticated approach, addressing PEM while maintaining the metabolic benefits of TB. Future studies should further assess individualized surgical strategies based on variations in total bowel length to optimize patient outcomes. However, GJIB may be a highly safe and predictable surgical intervention that prevents malabsorption while functionally excluding the foregut and stimulating the hindgut, improving insulin resistance using multiple mechanisms.
This study has significant limitations. Due to the retrospective nature of the study, we reported only our limited number of cases, gathering a small sample size. As we have significant experience with Duodenal Switch (DS) and Duodenoileal Interposition (DII) besides TB and have revised some of our DS patients to DII for PEM, we are familiar with the effect of hindgut stimulation on the control of excess weight regain and metabolic outcomes. So, we preferred to transpose the ileal segment, which was not technically demanding. However, this led to the failure to do sleeve-only revisions, and we could not have a cohort to compare. Further research is needed to refine patient selection criteria and validate these findings in larger cohorts, possibly in a multicenter study, comparing both techniques on feasibility and outcomes.


Comments (0)