Bariatric surgery is an effective treatment for weight loss and managing obesity-related conditions like GERD. However, its impact on esophageal function varies depending on the type of surgery performed. While weight loss generally improves GERD symptoms, the outcomes differ among surgical procedures. LRYGB is often preferred for patients with both obesity and severe GERD due to its potential to alleviate reflux symptoms. In contrast, LSG may not consistently improve GERD and could, in some cases, worsen reflux symptoms. Preoperative assessment is essential, as no single procedure suits all patients. Some surgeons consider GERD a contraindication for LSG due to the risk of exacerbating reflux [11].
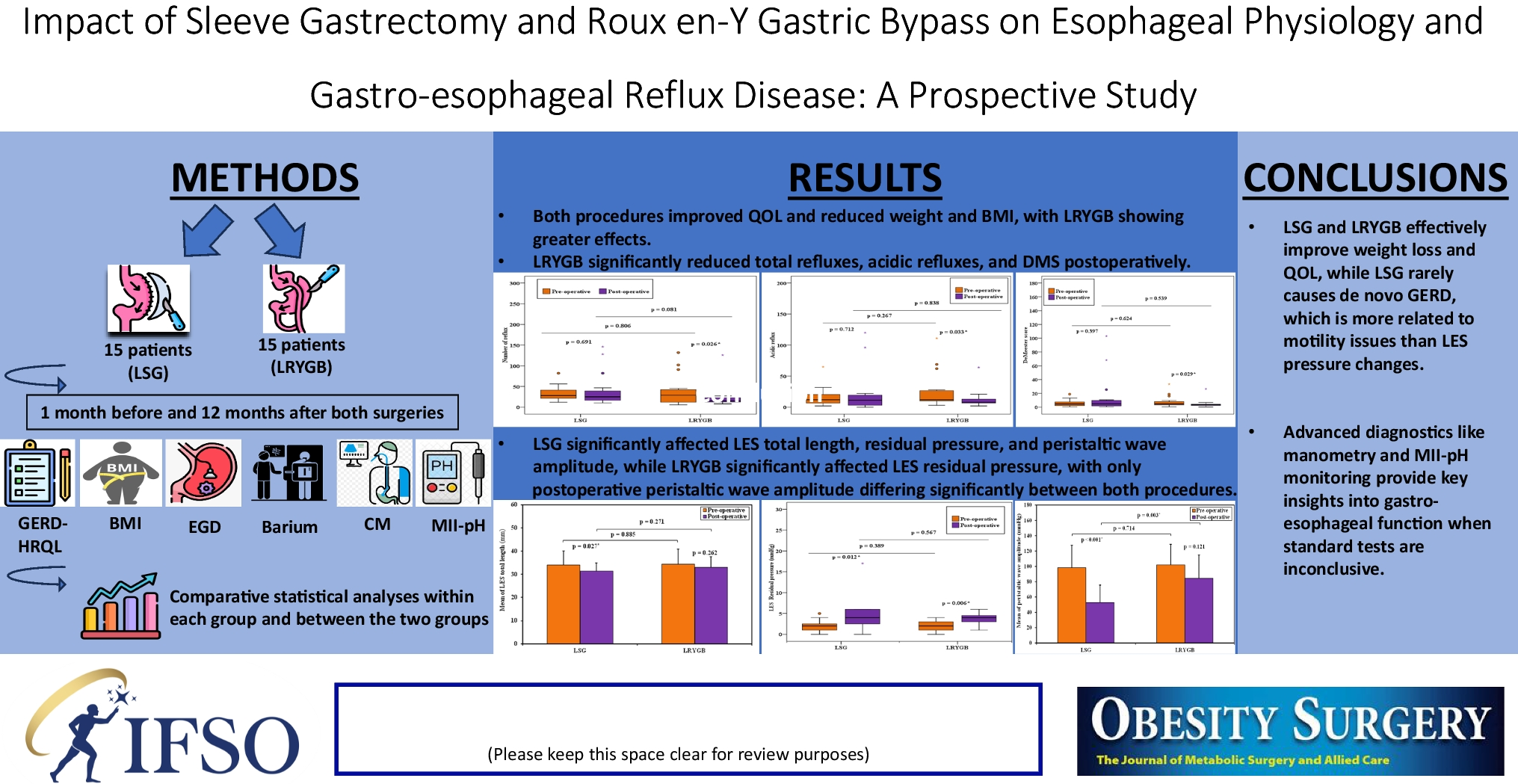
Studies examining the relationship between GERD and esophageal function following LSG and LRYGB have shown considerable variability in methodologies and outcomes, often relying on symptom questionnaires rather than objective assessments. This study aimed to address this gap by utilizing advanced diagnostic tools such as esophageal manometry and MII-pH monitoring to assess GERD and esophageal function. These technologies provide a more detailed understanding of changes in esophageal motility, pressure, and acid exposure post-surgery, offering valuable insights into the effects of LSG and LRYGB on GERD in patients with severe obesity.
The SLEEVEPASS trial [12] (240 patients) and the SMBOSS study [13] (217 patients) are the largest randomized clinical trials comparing LSG and LRYGB, with findings similar to ours. In our study, both groups showed significant postoperative reductions in weight and BMI, with the LRYGB group showing lower postoperative values. The PEWL was higher in the LRYGB group (50.48 ± 8.13%) than in the LSG group (36.21 ± 10.64%), consistent with other studies [14, 15] and a longer-term follow-up may help determine if these differences result from loss of effect of sleeve gastrectomy or from greater weight loss after gastric bypass. Both groups showed significant improvements in GERD-related symptoms and QOL, with no significant differences. The SLEEVEPASS trial also reported greater PEWL in LRYGB (57%) compared to LSG (49%) at 5 years, and both studies reported significant improvements in QOL.
Raj et al. [16] studied 77 patients and found improvements in weight-related parameters 6 months after both LSG and LRYGB, with no significant differences in GERD symptoms between the two groups. Similarly, in our study, GERD symptoms in the LSG group remained stable pre- and post-operation, aligning with Del Genio et al. [17], who found no change in reflux-related symptoms in 25 patients over a median of 13 months. Gadiot et al. [18] reported that 7% of asymptomatic patients developed de novo GERD after LSG, while 96% of those with preoperative GERD had symptom resolution after 5–8 years. In our study, four (26.7%) patients had post-surgery GERD, in whom symptoms resolved in two (50% of the affected). We also had two (13.3%) patients who continued to have GERD and two (13.3%) who developed de novo GERD.
In our LRYGB group, GERD symptoms significantly decreased. Preoperatively, eight patients (53.3%) experienced GERD, but postoperatively this number dropped to one case (6.7%), reflecting an 87.5% resolution of symptoms, with no new cases of de novo GERD. These results align with the bariatric outcomes longitudinal database (BOLD) database, where Pallati et al. [19] studied 22,830 patients, showing a 41% improvement in GERD symptoms and a 9.2% rate of de novo GERD after LSG, while for RYGB, GERD improved in 56.5% of patients. Studies also found RYGB improved GERD by > 90%, with 0–7% de novo GERD [20, 21]. Overall, no significant differences in GERD symptoms were found between the LSG and LRYGB groups pre- or post-surgery.
Clinically, both patient groups in our study reported a significant decrease in reflux symptoms post-operation, as measured by the GERD-HRQL questionnaire, with no difference between the groups. This aligns with a study of 128 patients assessing QOL after 1 year post-LSG and LRYGB using seven questionnaires, which showed similar significant improvements in scores between baseline and 12 months, except for the GerdQ score, which showed a difference between the groups [22]. Other prospective studies confirmed this improvement in scores after both procedures [5, 23]. The BOLD review showed the greatest GERD score improvement in LRYGB patients, followed by LSG [19].
Our study found that PPI usage in the LSG group decreased modestly from 40 to 26.7% postoperatively, while in the LRYGB group, PPI usage significantly dropped from 53.3 to 6.7%. Proton pump inhibitors were prescribed regardless of esophagitis detection, as GERD can occur without visible mucosal changes, which affect about 50% of GERD patients [24]. However, there were no statistically significant differences in PPI usage between the two groups.
Comparing with other studies, Himpens et al. [25] reported 75% resolution of GERD in LSG patients, but 21.8% developed new GERD cases within the first year. A French retrospective study showed over 50% of patients required PPIs during the first year after LSG [26], and Braghetto et al. [27] reported 57.2% of patients using PPIs due to reflux symptoms.
Conversely, studies on LRYGB consistently reported a reduction in PPI usage. Barr et al. [28] noted a 70% decrease 1 year after LRYGB, while Frezza et al. [29] found a reduction from 44 to 9% at 12 months in 152 patients. Parmar et al. [30] observed that 80% of patients who converted from LSG to LRYGB stopped GERD medications. However, Holmberg et al. [31] found persistent GERD in 48.8% of 2454 RYGB patients after 4.6 years, requiring acid-suppressing medications for more than 6 months in nearly half within 2 years.
In our LSG cases, EGD showed a decrease in esophagitis from 66.7 to 26.7%, with 20% having LA-A and 6.7% having LA-B esophagitis, comparable to another study reporting 26.3% with LA-A and 15.8% with LA-B; however, that study also noted a 42.1% increase in esophagitis post-sleeve gastrectomy [32]. De novo GERD signs were seen in 13.3% of cases, consistent with other studies showing new esophagitis ranging from 6.5 to 66.7% [27, 33, 34]. Sharma et al. [5] found post-LSG esophagitis in 25% of patients. In contrast, for LRYGB cases, EGD revealed a reduction in esophagitis from 53.3 to 6.7%, with no new GERD findings, aligning with other studies that showed esophagitis decreased from 42 to 4% post-LRYGB [35], with some cases persisting at 20% after 1 year (yet with 11% improved) [36]. One case (6.7%) of Barrett’s metaplasia occurred after LSG, falling between Braghetto’s 1.2% and Genco’s 17.2% [37, 38]. These differences might be due to the strict endoscopic follow-up of cases, low severity of GERD (according to LA classification), and the use of PPIs. No metaplasia cases were observed after LRYGB, similar to a study with a 3-year follow-up [23].
In our study, barium swallow studies showed a decrease in reflux signs from 33.3 to 13.3% after LSG and from 66.7 to 0% after LRYGB. A review by Howard et al. [39] found that 18% of patients had GERD signs post-LSG, with a 40% PEWL and a mean follow-up of 8 months.
Gastric morphology is another factor contributing to the progression of esophagitis after bariatric surgery. Dias da Silva et al. [40] found that 28.3% of patients with esophagitis post-LSG had abnormalities in the gastric tube, including gastric dilation, twist, neo fundus formation, and hiatal hernia. In our study, 20% and 13% of patients had hiatal hernias after both surgeries, respectively. Despite a significant reduction in hernia cases (postoperatively in both groups by 50% and 33.3%, respectively) due to weight loss, the size of the gastric tube was not measured (due to the lack of computed tomography (CT) scans done, which are more accurate than barium studies). The correlation between hiatal hernias and GERD symptoms was noted, and some studies suggest that concurrent hernia repair during bariatric surgery, especially for small hernias, might not always be beneficial and could introduce complications and that is what we believed in. Kothari et al. [41] found that many surgeons avoid hernia repair during LRYGB, while Snyder et al. [42] reported no impact on GERD symptoms from repairing small hiatal hernias (< 4 cm) with LSG. All preoperative hiatal hernias in both our groups were small (< 4 cm), which did not need definitive repair.
Accelerated gastric emptying after LSG was reported by Melissas [42], but Bernstine et al. [43] did not find the same results. Our study observed no abnormal gastro-duodenal emptying and no delayed gastrojejunal emptying after LRYGB. This aligns with Näslund et al. [44], who also did not find delayed emptying after LRYGB, except in one patient with anastomotic stenosis. Variations in results may be due to differences in surgical techniques and the lack of scintigraphy.
MII-pH monitoring has significantly enhanced the evaluation of GERD by detecting a greater number of reflux episodes compared to traditional 24-h pH monitoring. This advancement is achieved by assessing both the physical and chemical properties of the refluxate. The incidence of new-onset GERD following bariatric surgery varies, influenced by factors such as the duration of follow-up and the criteria used for diagnosis. Currently, MII-pH is regarded as the leading method for diagnosing and managing GERD, as it identifies acidic, weakly acidic, and alkaline refluxes, and differentiates between liquid, gas, and mixed refluxes, thereby offering a comprehensive characterization of the condition.
Studies on LSG’s impact on acid exposure show mixed results: some indicate a significant increase in total acid exposure after 12 months [45], while others report a decrease within the same timeframe [46]. Although LRYGB is considered the optimal treatment of GERD in patients with severe obesity [47], it may not always fully resolve GERD symptoms [25, 48]. Some studies have reported that up to 22% of patients who undergo LRYGB continue to experience GERD symptoms postoperatively [29].
Unlike previous studies reporting significant increases in AET% and DMS after LSG [49, 50], our study found only a mild, non-significant rise in these parameters, with AET% increasing from 6.7 to 46.7% and DMS from 6.7 to 20%. This result is consistent with a prior trial involving 37 patients, where no significant changes in DMS or AET% were noted, and DMS increased in 18.9% of cases [46]. Similarly, a recent study of 30 patients with a 1-year follow-up reported a non-significant rise in AET% and DMS, with QOL remaining unaffected [51]. Additionally, while there was a non-significant decrease in the total number of reflux episodes and acidic refluxes, this trend aligns with another study showing a stable DMS and a non-significant reduction in reflux episodes and acid exposure after 1 year [32]. These findings may be influenced by continued PPI use despite recommendations to discontinue them 15 days before assessment.
In our LRYGB group, there was a notable reduction in the DMS post-operation, with pathological DMS decreasing from 20 to 6.7%. However, the AET% remained largely unchanged. These findings are consistent with previous studies which also reported significant improvements in DMS after LRYGB [20, 52], with postoperative pathological DMS observed in only 9% and 12.5% of patients in other studies [16, 23]. We also observed a significant reduction in the total number of reflux episodes and acidic refluxes, which decreased from 20% preoperatively to 6.7% postoperatively. These results align with previous research showing significant improvements in various pH-based parameters, such as the percentage of time with esophageal pH < 4, the total number of reflux episodes, and the number of acidic reflux episodes [23, 53].
The study of non-acidic reflux in bariatric surgery is limited. Our research found no significant changes in the number of non-acidic reflux episodes within or between LSG and LRYGB groups, aligning with another group’s findings [16]. This lack of significance is likely because alkaline reflux is prevented by the Roux-en-Y anastomosis distal to the gastrojejunostomy.
For weakly acidic reflux, our study showed no significant changes overall, though there was a minor decrease in the LSG group and an increase in cases exceeding normal levels from 6.7 to 20%. This contrasts with Chern et al. [54], who reported a significant increase in weakly acidic reflux after LSG due to reduced gastric acidity after resection; however, our study did not observe the significant decrease in LES pressure noted by theirs.
In the LRYGB group, we saw a slight rise in weakly acidic reflux episodes, but the percentage of cases exceeding normal levels remained stable at 6.7%. This differs from Morino’s group [55], who found that 75% of patients had weakly acidic reflux and 44% developed esophagitis in their 5-year follow-up. Their results suggested that abnormal motility in the Roux limb, supported by a recent study on electrical activity and manometry, might contribute to these findings [56].
Esophageal manometry offers both quantitative and qualitative assessments of esophageal pressure and peristaltic coordination, including measurements of the LES. However, findings regarding manometric changes following bariatric surgery remain inconsistent. In our study comparing both groups, LES parameters were similar; however, alterations in impaired motility appeared to influence reflux.
Our study found no significant changes in LES basal pressure following LSG. Preoperatively, 33.3% of patients had LES pressures below the normal range, which increased slightly to 40% postoperatively. This result is consistent with Del Genio et al.’s study of 25 patients [17], which showed no significant changes in LES pressure and an increase in ineffective motility 1 year after LSG. Similarly, Rebecchi et al. [46] reported no changes in LES pressure. In contrast, Braghetto et al. [27] observed a significant decrease in LES pressure in 85% of patients 6 months post-LSG, attributed to partial sectioning of the sling fibers. Burgerhart et al. [57] also noted reduced LES pressure 3 months after LSG, despite stable peristalsis. Petersen et al. [58] suggested that higher LES pressure post-LSG might protect against GERD, potentially due to variations in surgical technique. These findings suggest that isolated LSG may not significantly impact the LES, highlighting the importance of surgical technique, especially in dissection near the gastroesophageal junction.
The LRYGB group showed no significant changes postoperatively in LES basal pressure which was below the normal range in 13.3% of patients and decreased to 6.7% after surgery. Similarly, previous studies have reported non-significant changes in LES pressure at both the same and longer follow-up periods [16, 55].
In our study, the total LES length tended to decrease after LSG and showed a non-significant shortening after LRYGB. The abdominal LES length remained unchanged after LSG and slightly increased post-LRYGB, but these changes were not statistically significant between the groups. The observed shortening of the LES following LSG might be due to increased intragastric pressure compressing the LES, similar to effacement from gastric distention. Despite significant weight loss in both groups, the abdominal LES length did not reduce. Other studies have reported conflicting results, with one showing an increase in LES length after LSG [59] and another showing an increase after LRYGB [16].
Interestingly, the median LES residual pressure nearly doubled postoperatively in both groups, with only one case (6.7%) in group A exceeding the normal range. This is contrary to other studies where LES residual pressure slightly decreased [54, 60]. The increased intragastric pressure and reduced distensibility of the sleeve might heighten tension at the gastroesophageal junction. Additionally, dissection of the phreno-esophageal membrane for stapler placement near the angle of His may disrupt the esophageal sphincter’s integrity, affecting outcomes in gastric bypass [23].
The study found a significant difference in peristaltic wave amplitude between the two groups postoperatively. In the LRYGB group, peristaltic amplitude decreased slightly but stayed within normal ranges for all patients and had no clinical significance. In contrast, the LSG group showed a more pronounced decline in esophageal contractility, with one patient (6.7%) falling below the normal range postoperatively. This decline may lead to ineffective clearance of regurgitated gastric contents and stasis, possibly as a compensatory mechanism for the weakened LES. While some studies reported no significant changes in esophageal wave amplitude post-sleeve gastrectomy [46, 49], findings from two Italian studies with 25 and 21 patients, respectively, indicated a significant increase in ineffective esophageal motility following LSG [17, 32]. Conversely, studies on Roux-en-Y gastric bypass consistently found no severe impairment in esophageal peristaltic amplitude [48, 52].
A patient from the LSG group was diagnosed with type II achalasia, as confirmed by high-resolution manometry (HRM). This diagnosis was based on a LES basal pressure of 41 mmHg, a residual pressure of 17 mmHg, failure of complete relaxation, and absent peristaltic waves, which prevented assessment of amplitude, velocity, and morphology. Such a finding is rare after LSG, as noted in the systematic review by Crafts et al. and he was scheduled for a Heller myotomy with conversion surgery [61].
Our study is prospective and integrates both subjective and objective parameters for assessment. Additionally, since no significant preoperative differences were observed between the groups, this design helps minimize potential biases. The primary limitations of this study include the relatively short follow-up period and the limited, non-randomized sample size. The study faced challenges in recruitment, as many patients declined to undergo the minimally invasive investigations. Additionally, CM was utilized instead of the more advanced HRM technology.


Comments (0)