Design
This population-based cohort study included all adults with a recorded obesity diagnosis in any of the four Nordic countries Denmark, Finland, Norway, or Sweden (alphabetic order). The overall study period was from January 1, 1989, until December 31, 2020, but differed between the participating countries (July 1, 1996, until December 31, 2019, in Denmark; January 1, 1989, until December 31, 2019, in Finland; January 1, 2007, until December 31, 2020, in Norway; and January 1, 1989, until December 31, 2020, in Sweden). Denmark started follow-up with the introduction of operation codes for bariatric surgery, which became available in 1996. Finland and Sweden started follow-up with the introduction of ICD- 9. Finally, the follow-up in Norway started with the introduction of the patient registry in 2007. The study was approved by the appropriate ethical review boards, data inspectorates, and governmental agencies in the participating countries [13].
Obesity Cohort
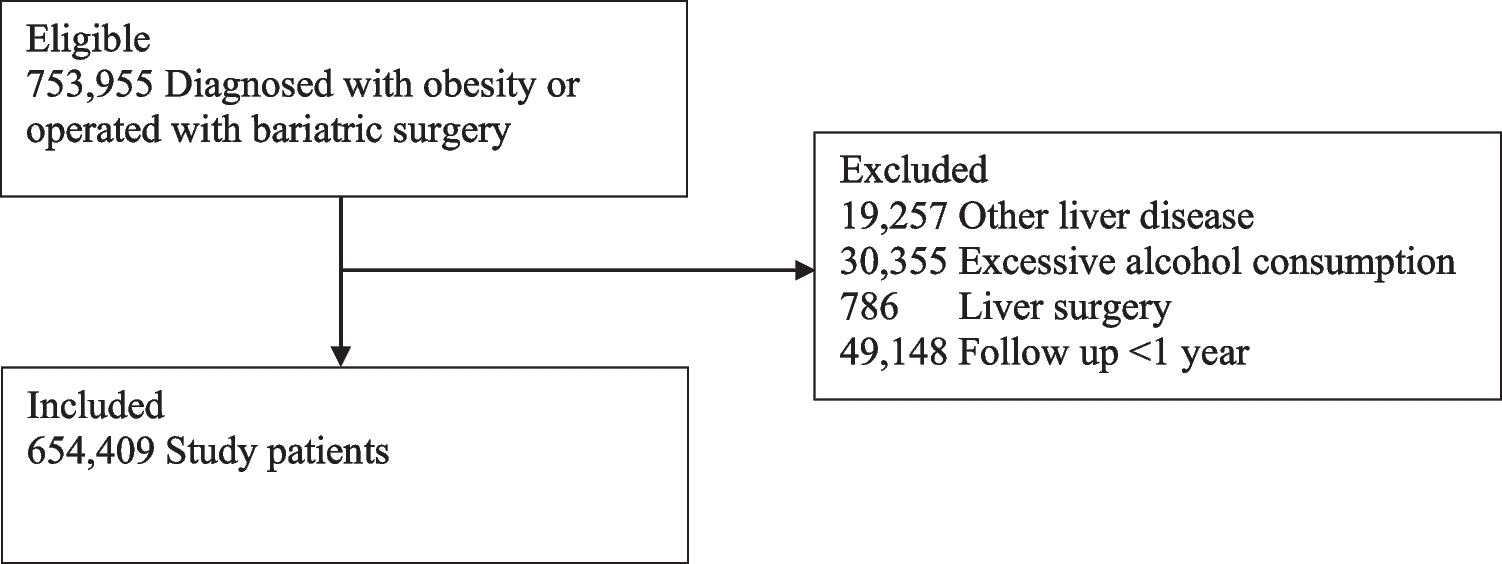
The study cohort was an updated version of the Nordic Obesity Surgery Cohort (NordOSCo), which has been described in detail elsewhere [13, 14]. NordOSCo includes all patients with an obesity diagnosis or bariatric surgery in any of the national patient registries of Denmark, Finland, Norway, or Sweden. The patient registries in all participating countries record individual-level data on all hospital-based healthcare, including patient information, diagnoses, and procedures, and have a similar structure and quality, thus allowing for harmonization of data in large databases such as NordOSCo. In brief, the cohort of the present study consisted of all adult (≥ 18 years) individuals with an obesity diagnosis (ICD-codes are provided in Supplementary Table 1) according to any of the nationwide patient registries in the participating countries. The obesity diagnosis was made by at least one physician and registered in one of the participating countries’ patient registries. Data on all diagnoses and surgical procedures, cancer, and mortality came from nationwide complete, well-maintained, and well-validated registries [13]. Excluded were patients with a history of excessive alcohol consumption, any liver disease other than steatotic liver disease, or liver surgery (Supplementary Table 1).
Exposure
The main study exposure was primary bariatric surgery, including the procedures gastric bypass, gastric banding, sleeve gastrectomy, and duodenal switch (Supplementary Table 1). The secondary exposure was gastric bypass alone, which was the dominating bariatric procedure in the Nordic countries during the study period. Bariatric surgery was compared with non-operative care for morbid obesity and related comorbidities, including advice and medical treatment. Data on bariatric surgery came from the national patient registries, which have been validated for high completeness and accuracy [15,16,17]. The patient registry in Sweden has specifically been validated for bariatric procedures by comparing registry data with medical records and operation charts in 938 patients, showing 97% concordance [18].
Outcomes
The main outcome was incidence of end-stage liver disease. The secondary outcome was mortality in end-stage liver disease. End-stage liver disease included liver cirrhosis, esophageal or gastric varices, liver encephalopathy, hepatorenal syndrome, portal hypertension, ascites due to liver disease, liver failure, and liver transplantation. These diagnoses were identified from the corresponding diagnosis codes in the national patient registries (Supplementary Table 1). Mortality in end-stage liver disease was defined as death with one of the above-listed diagnoses as the main cause of death in the national cause of death registries, which have > 96% completeness for the cause of death [13].
Statistical Analysis
Follow-up started 1 year after the date of obesity diagnosis (cohort entry). This 1-year time latency allowed for a lead time between the exposure attainment (bariatric surgery) and occurrence of outcomes. Thus, person-time and cases in both exposed and unexposed cohorts that occurred during this first year of follow-up were excluded from the analyses. Patients with obesity diagnosis who underwent bariatric surgery after the 1-year latency period were censored from the non-operated group and instead contributed person-time in the operated group from the date of surgery onwards, meaning that an individual could contribute time at risk in both groups. Follow-up ended at the date of end-stage liver disease diagnosis (for the main outcome only), death, or end of the study period, whichever occurred first. Cox proportional hazards regression was used to calculate hazard ratios (HR) with 95% confidence intervals (CI) for both outcomes. The time metric for the analysis was age at the date of obesity diagnosis or bariatric surgery [19, 20]. Hence, all analyses were adjusted for age and accounted for left truncation of the data due to unknown onset of obesity. A multivariable model adjusted for another five potential confounders: sex (female or male), calendar year (continuous), diabetes (yes or no), Charlson comorbidity index (excluding diabetes) (0, 1, or ≥ 2), and country (Denmark, Finland, Norway, or Sweden). Diabetes and Charlson comorbidity score were defined by the corresponding diagnosis codes in the national patient registries (Supplementary Table 1). The analyses were stratified by duration of follow-up (1–5, 5–10, 10–15, and ≥ 15 years), age (below and above the median), sex (female and male), and diabetes (yes or no).
To evaluate if any identified association was explained by differential development of liver diseases other than steatotic liver disease among the operated and non-operated patients, we conducted an analysis where patients were censored upon developing excessive alcohol consumption or liver diseases other than MASLD or non-alcoholic steatohepatitis during follow-up (Supplementary Table 2).
The proportional hazard assumption was not met for all analyses, but we stratified the HR by follow-up time which relaxed the assumption of proportional hazards. All analyses were determined in a detailed study protocol completed prior to data analysis. The data management and statistical analyses were conducted by a senior biostatistician (GS) using the statistical software STATA/MP 15.1.


Comments (0)