
Remember me

We enrolled 262 patients who underwent their first continuous-flow LVAD implantation for end-stage heart failure, including bridge-to-bridge, bridge-to-transplantation, and destination therapy, between January 2005 and March 2023. Patients who underwent conversion from one implantable LVAD to another were excluded. Among these patients, 224 patients were performed the conventional driveline management and 38 patients were performed the modified fixation method. We evaluated the effectiveness of the modified driveline management in comparison with the conventional driveline management. The mean follow-up duration was 854 ± 648 days. All follow-up examinations were completed on July 31, 2023.
All patients and their families provided informed consent to participate in related clinical studies before LVAD implantation.
Conventional and modified driveline managementAt our hospital, LVAD driveline was positioned between rectus abdominal muscle and anterior layer of rectus from end of thoracic cavity to just below skin penetration site at LVAD implantation. We conduct VAD rounds to evaluate and provide advice on driveline management. These rounds are usually conducted once a week by a team of experts, including cardiovascular surgeons, VAD coordinators, and wound-care nurses. We used 0.5% chlorhexidine gluconate or saline for daily care at the LVAD driveline exit site. No special dressings were used, and the LVAD driveline exit site was protected with clean gauze. During the patients’ stay in the intensive care unit (ICU) after LVAD implantation, the cardiovascular surgeon was responsible for the daily care of the LVAD driveline exit site. After leaving the ICU, the wound-care nurses took over this responsibility. Patients received instructions on driveline care from the wound-care nurses until they or their caregivers demonstrated satisfactory cleaning skills. Patient care skills were also assessed during the VAD rounds. After discharge from the hospital, the patients or their caregivers were responsible for driveline care. When the patients took showers, the LVAD driveline exit site remained waterproof. The status of the LVAD driveline exit site was checked during the monthly outpatient treatment by VAD-expert medical doctors and the VAD coordinator nurses.
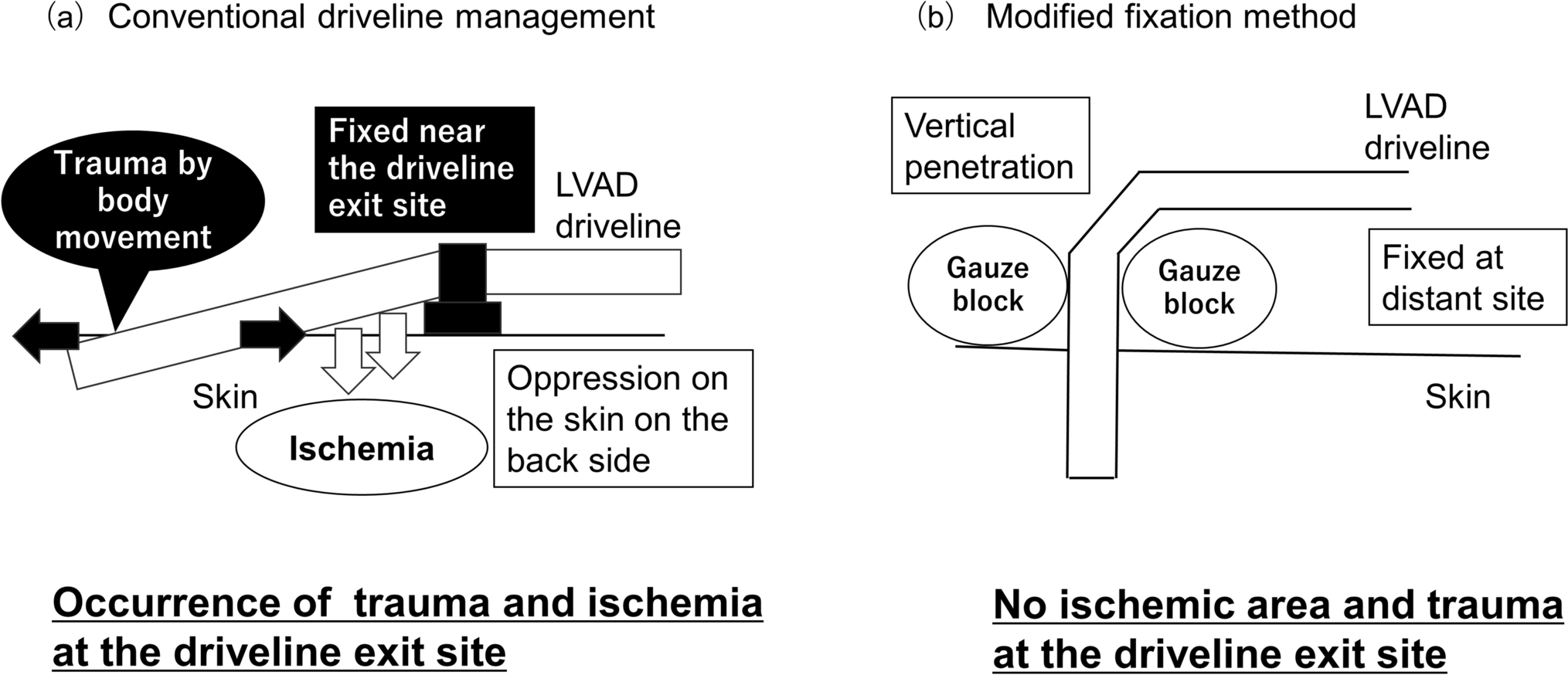
In conventional driveline management (Figs. 1a, 2a), the LVAD driveline penetrated the skin along the body surface and was fixed near the penetration site. This approach led to oppression on the skin on the back side of the LVAD driveline at the exit site, potentially causing skin tissue ischemia, resulting in trauma and ulceration at the LVAD driveline exit site. The movement of the LVAD driveline exit site due to body movements also increased the risk of trauma and driveline infection. Discharge from the LVAD driveline exit site was frequently monitored. Therefore, the fixed position and penetration angle of the LVAD driveline from the skin were changed during the VAD rounds.
Fig. 1
Comparison of concepts in conventional driveline management and modified fixation method. a Concept and problems of conventional driveline management. b Concept of the modified fixation method. Abbreviations: LVAD left ventricular assist device
Fig. 2
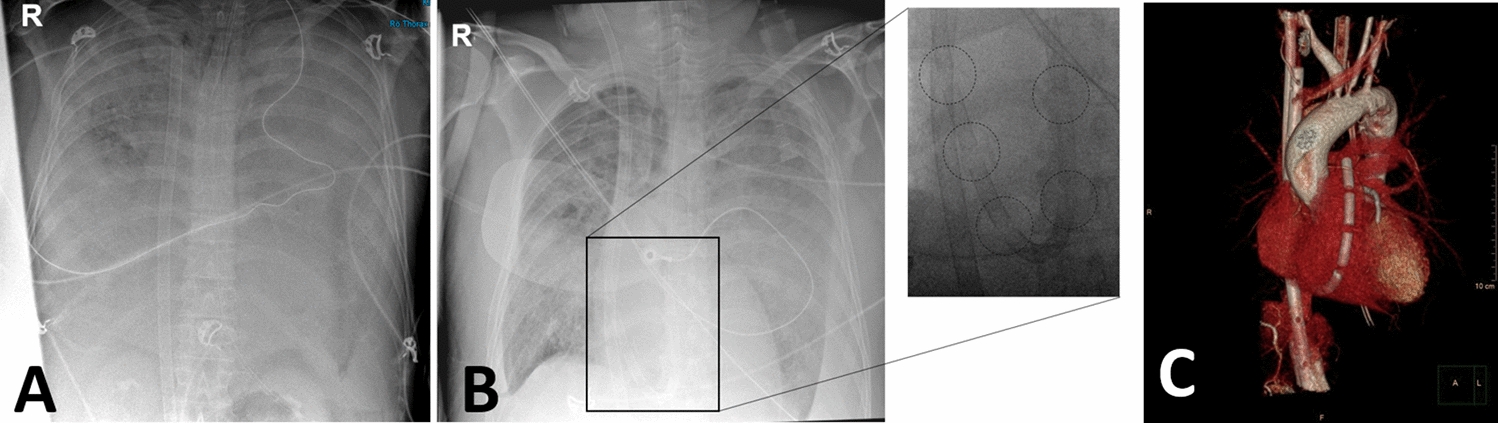
Comparison of conventional driveline management and modified fixation method. a Picture and computed tomography images of skin penetration of the LVAD driveline in a patient with conventional driveline management. b Picture and computed tomography images of skin penetration of the LVAD driveline in a patient with the modified fixation method
The modified fixation method (Figs. 1b, 2b) was implemented to manage the problems associated with conventional driveline management. This modified fixation method involves vertical penetration of the LVAD driveline into the skin. Subsequently, the LVAD driveline was fixed at a distant site on the front of the abdomen. A gauze block was used to assist in vertically fixing the LVAD driveline to the skin. Problems concerning the skin on the back of the LVAD driveline at the exit site were avoided by penetrating the LVAD driveline vertically from the skin. The movement of the LVAD driveline exit site was suppressed by fixing the driveline at a distance from the LVAD driveline exit site (on the front of the abdomen), relieving the stress caused by the movement of the body to the LVAD driveline exit site. The fixed LVAD driveline was protected with gauze, and a special abdominal band was placed over the area to protect the entire LVAD driveline. Overall, the modified fixation method prevented both the ischemia of the skin on the back side of the LVAD driveline and the trauma at the LVAD driveline exit site.
Definition of LVAD driveline infectionsIn this study, an LVAD driveline infection was defined as a deep driveline infection that required treatments including surgical intervention and intravenous administration of antibiotics. Deep driveline infection involved infectious symptoms, including a local increase in temperature and pain around the exit site, elevated inflammatory reaction level, and positive wound culture and abscess from the deep soft tissue around the LVAD driveline observed during surgical debridement for the LVAD driveline infection [7, 14].
Data collectionPatient data included baseline characteristics, etiology, comorbidities, preoperative hemodynamics, laboratory values, echocardiographic parameters, LVAD type, method of driveline management, and duration of LVAD implantation. All patient data were collected from the electronic medical and operative records.
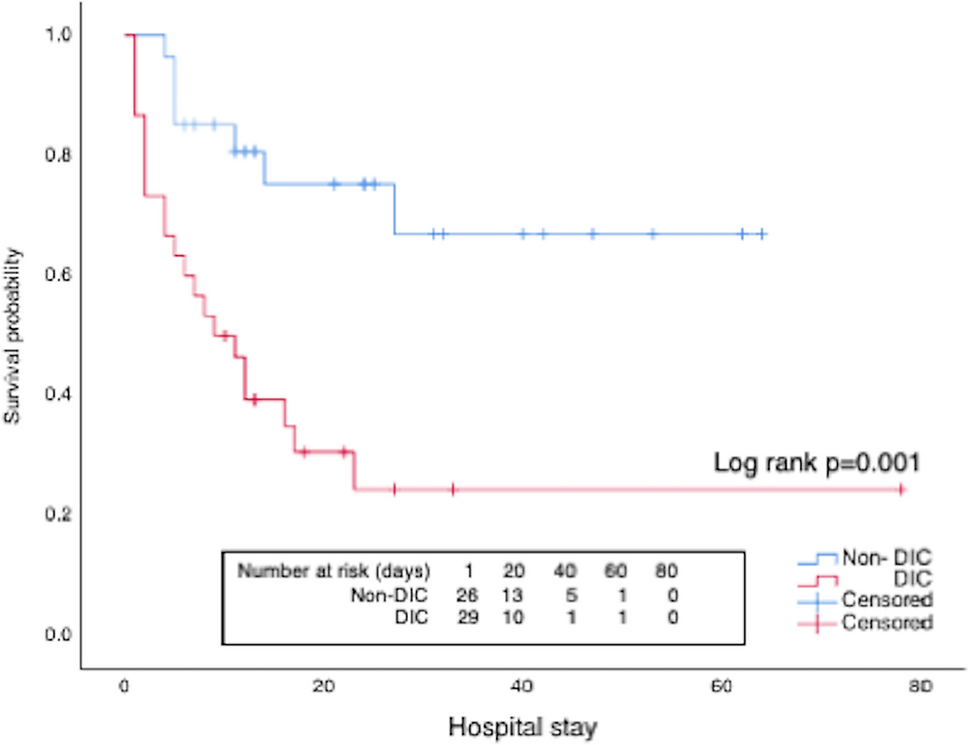
Statistical analysesContinuous variables were presented as the median (interquartile range) or mean ± standard deviation. All statistical analyses were performed using JMP 16.0 (SAS Inc., Cary, NC, USA). Categorical variables were summarized as frequencies and percentages and compared among groups using Chi-square or Fisher’s exact tests. All p-values for the statistical analyses were two-tailed, and statistical significance was set at p < 0.05. Kaplan–Meier analysis was used to calculate the rates of freedom from LVAD driveline infections. Propensity score matching (1:2 matching, with the nearest neighbor matching without replacement) was performed to adjust for significant differences in risk factors of LVAD driveline infection (age, body mass index (BMI), preoperative albumin and preoperative incidence of diabetes mellitus (DM)) between patients with conventional driveline management and modified fixation method.
Comments (0)