
Remember me



We analyzed 97 patients with IPF and 76 healthy participants. The median follow-up time in the patients with IPF was 40.1 months (21.4 − 62.3 months). The main characteristics of the patients and healthy participants are shown in Table 1 and Supplementary Information S1. The patients with IPF were significantly older than healthy participants (68.0 years and 61.5 years, P = 0.024). No significant differences in sex, body mass index (BMI), or pack-year smoking history were observed between patients with IPF and healthy participants. The patients with IPF had a significantly lower forced vital capacity (FVC) than healthy participants (74.3% vs. 95.0%, P < 0.0001). No significant differences in serum sTLR4 levels were observed between the patients with IPF and the healthy participants (1.0 ng/mL [0.7 − 1.8] and 1.2 ng/mL [0.8 − 3.1], P = 0.22; Supplementary Information S2).
Table 1 Clinical characteristics of the study participantsAssociation of sTLR4 with AE-IPF and Prognosis of IPFTwenty-three patients (23.7%) developed AE-IPF over 5 years. The 5-year survival rate was significantly lower in the patients with AE during the 5-year period compared to those without (P < 0.0001; Supplementary Information S3).
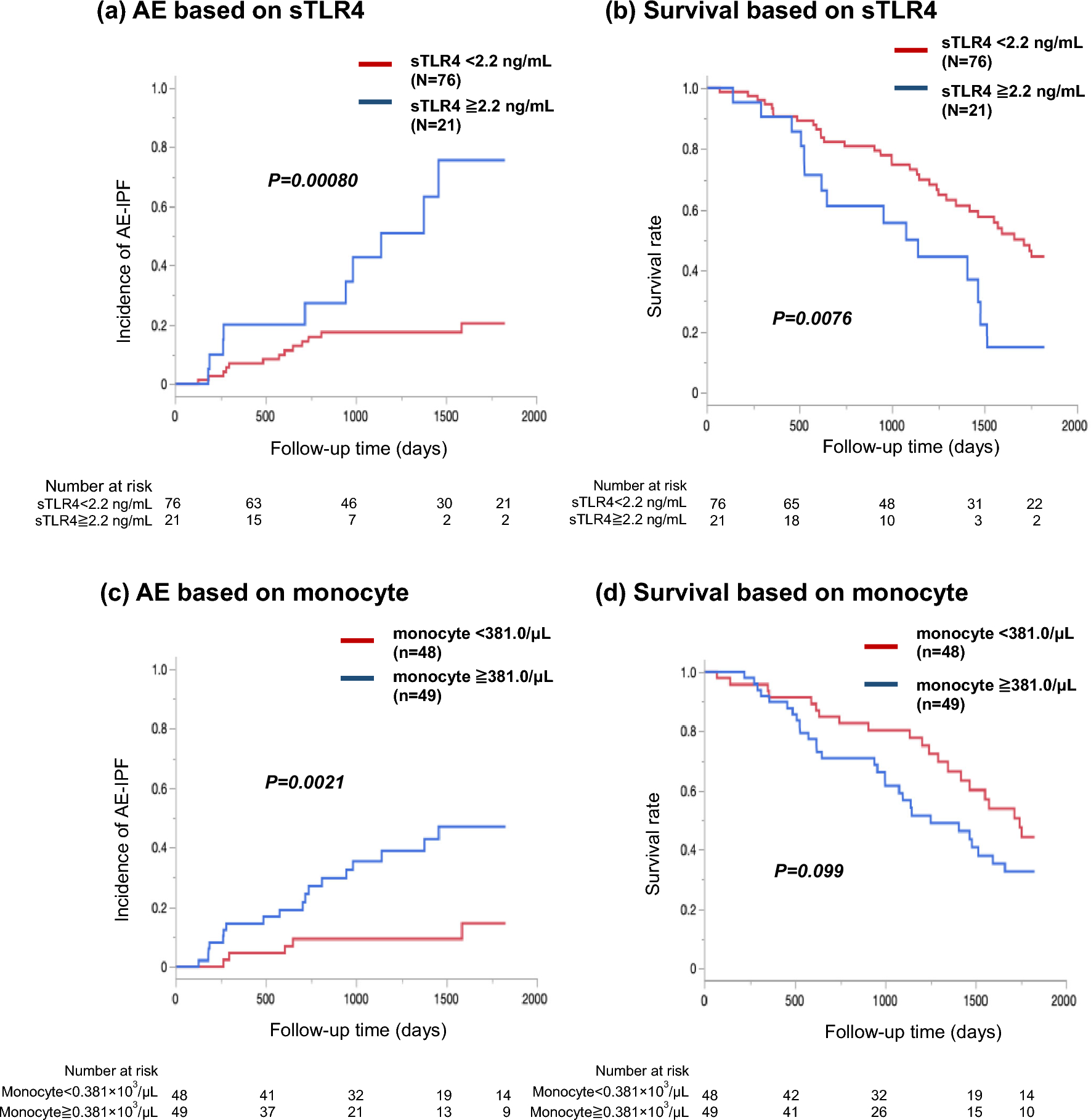
The optimal cut-off level of sTLR4 for predicting AE-IPF was 2.2 ng/mL (sensitivity, 43.5%; specificity, 85.1%), as identified by ROC curve analysis. Kaplan–Meier curve analysis and log-rank tests revealed that sTLR4 levels ≥ 2.2 ng/mL were associated with a higher incidence of AE-IPF (P = 0.00080; Fig. 1a). No significant differences in clinical characteristics were observed between patients grouped by sTLR4 levels (Table 1).
Fig. 1
Incidence of AE-IPF and survival rate based on serum levels of sTLR4 and monocyte. In Figure a and b, red solid line indicates the patients with lower levels of sTLR4 (< 2.2 ng/mL), and blue solid line indicates the patients with higher levels (≥ 2.2 ng/mL). Among patients with IPF, those with higher levels of serum sTLR4 (≥ 2.2 ng/mL) showed a significantly higher incidence of AE-IPF (a) and poorer survival (b) than those with lower levels. In Fig. c and d, red solid line indicates the patients with lower levels of monocyte (< 381/μL), and blue solid line indicates the patients with higher counts (≥ 381/μL). Patients with higher monocyte counts (≥ 381/μL) showed a significantly higher incidence of AE-IPF (c) and tendency of poor survival (d) compared with patients with the lower counts in patients with IPF. IPF, idiopathic pulmonary fibrosis; sTLR4, soluble Toll-like receptor 4; AE, acute exacerbation
Additionally, the association between sTLR4 levels and the survival rate was analyzed. Soluble TLR4 levels ≥ 2.2 ng/mL were associated with a lower survival rate in patients with IPF (P = 0.0076; Fig. 1b).
Association Between Serum sTLR4 Levels and Baseline CharacteristicsIn patients with IPF, Spearman’s correlation coefficients revealed that serum levels of sTLR4 were positively, although weakly, correlated only with monocyte count as shown in Fig. 2 (P = 0.032, rs = 0.21). However, there was no association between serum levels of sTLR4 and BMI, pack-years, FVC, white blood cell count, neutrophil count, lymphocyte count, platelet count, or C-reactive protein (CRP) levels (Supplementary Information S4).
Fig. 2
Association between sTLR4 levels and monocyte counts. Fig. 2 shows a weak correlation between serum levels of sTLR4 and monocyte counts (P = 0.032, rs = 0.21). sTLR4, soluble Toll-like receptor 4
Association of Monocyte Count with AE-IPF and Prognosis of IPFThe optimal cut-off level of monocyte counts, as identified by ROC curve analysis, for predicting AE-IPF was 381/μL (sensitivity, 78.3%; specificity, 58.1%). Kaplan–Meier curve analysis and log-rank test revealed that monocyte levels ≥ 381/μL were associated with a higher incidence of AE-IPF (P = 0.0021; Fig. 1c). The survival rate tended to be lower in patients with high monocyte counts (P = 0.099; Fig. 1d). The clinical characteristics of patients grouped by monocyte levels are shown in Table 1. There were more men in the high monocyte level group, but no other significant differences were observed between the two groups.
Cox Hazard Analyses to Identify the Independent Predictive Factors for AE-IPF and Poor Prognosis of IPFIn the univariate Cox proportional hazards models, serum sTLR4 ≥ 2.2 ng/mL was significantly associated with higher incidence of AE-IPF and shorter survival in the patients with IPF. On the other hand, monocyte count ≥ 381/μL was significantly associated with only higher incidence of AE-IPF (Table 2).
Table 2 Cox proportional hazards analysis to identify predictive factors for AE and prognosis of IPFMultivariate Cox proportional hazards analysis included sTLR4 ≥ 2.2 ng/mL, monocyte count ≥ 381/μL, and FVC as explanatory variables because sTLR4 and monocyte count showed a significant association with AE and lower percentage of FVC was well known as a risk of AE and shorter survival. In this multivariate analyses, sTLR4 ≥ 2.2 ng/mL and monocyte count ≥ 381/μL were independently associated with higher incidence of AE-IPF. Additionally, sTLR4 levels and FVC, but not monocyte count, were independently associated with survival in patients with IPF.
Risk Stratification of AE-IPF Based on the Combination of sTLR4 and MonocyteIn the exploratory analysis, the participants were divided into three groups according to the number of AE risks consisted of sTLR4 level and monocyte count identified in this study. Patients with two risks defined as group A (17 patients with sTLR4 level > 2.2 ng/mL and monocyte counts > 381.0/μL), patients with one risk defined as group B (36 patients with either higher levels of sTLR4 or higher monocyte counts), and patients with no risk defined as group C (44 patients with lower level of sTLR4 and lower monocyte counts). Group B included 4 patients with higher levels of sTLR4 and lower monocyte counts, and 32 patients with lower levels of sTLR4 and higher monocyte counts.
The characteristics of the three groups are summarized in Supplementary Information S5. No significant differences in age, sex, BMI, smoking history, and FVC were observed among the three groups. Kaplan–Meier curve analysis and the log-rank test revealed that the incidence of AE-IPF in group A (higher levels of sTLR4 and monocyte) was higher than that in groups B and C (Fig. 3). Univariate and multivariate Cox proportional hazards analyses showed that patients in group A had the highest risk of developing AE-IPF (Table 3).
Fig. 3
Incidence of AE-IPF based on the combination of sTLR4 and monocyte. In Fig. 3, three patients’ groups are defined based on sTLR4 level and monocyte count; Group A (red solid line), patients with sTLR4 level > 2.2 ng/mL and monocyte counts > 381/μL; Group B (green solid line), patients with either higher sTLR4 level or higher monocyte counts; Group C (blue solid line), patients with lower level of sTLR4 and monocyte counts. The incidence of AE-IPF is higher in Group A than that in Groups B and C. AE-IPF, acute exacerbation of idiopathic pulmonary fibrosis; sTLR4, soluble Toll-like receptor 4
Table 3 Cox proportional hazards analysis for analysing the association between AE-IPF and the combination of sTLR4 and monocyte
Comments (0)