This study identified two key findings: (1) LBM-based SUV normalisation significantly reduces weight dependency compared to BW-based normalisation, and (2) bone marrow demonstrated low variability and SUVs below previously reported SUVs of tumour lesions and is therefore the most reliable reference tissue for visual analysis and comparison in [1⁸F]mFBG PET-CT imaging. If uptake exceeds normal bone marrow uptake, it may be considered pathological. These findings provide critical insights into optimising both quantitative and visual PET imaging in both paediatric and adult patients by addressing weight dependency and variability in SUV measurements.
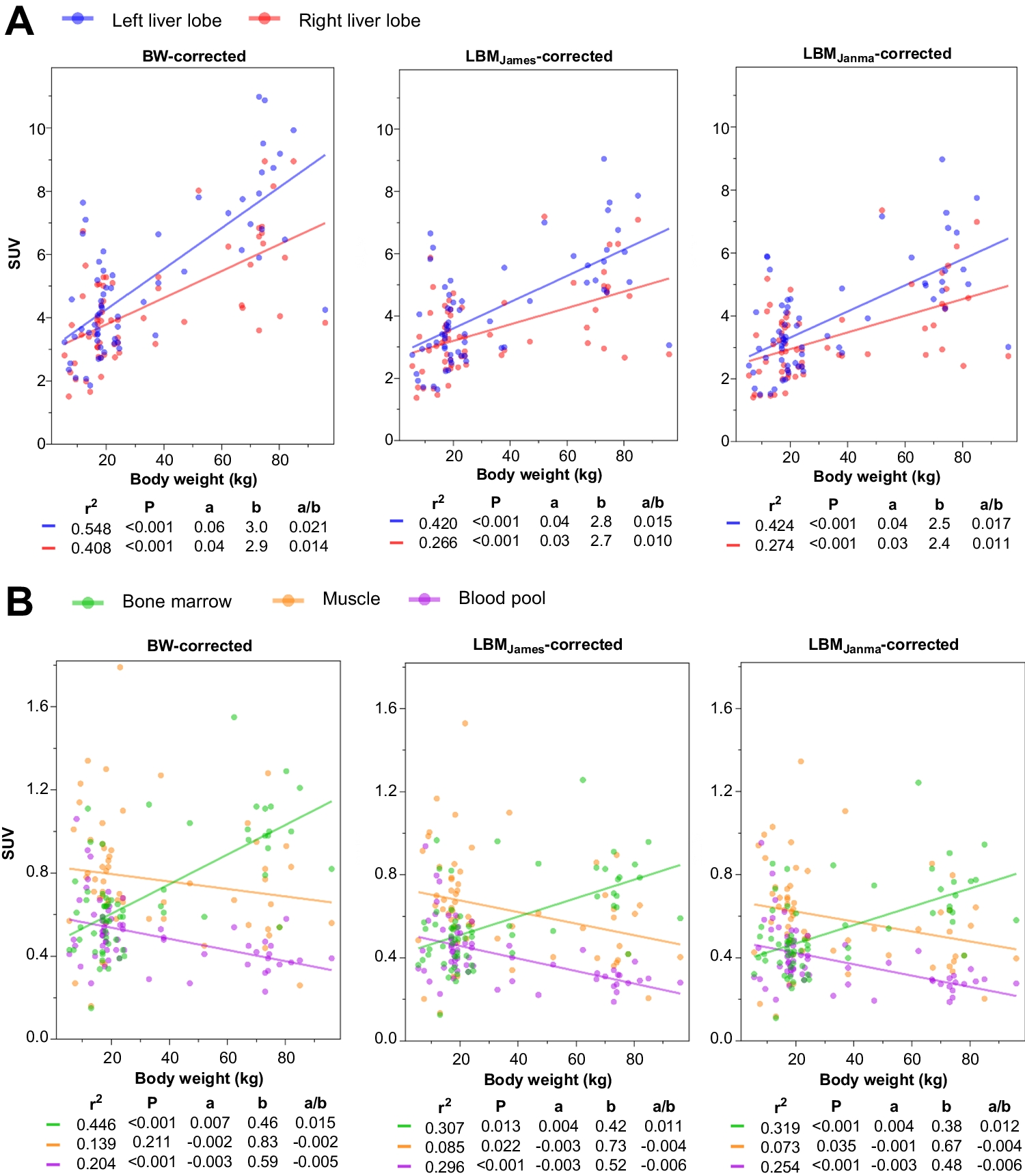
SUVBW normalisation exhibited the highest variability and strongest correlation with body weight across all reference tissues, except the blood pool. In contrast, LBM-based normalisation significantly reduced weight dependency, providing improved consistency and precision. Both SUVLBMJames and SUVLBMJanma formulations yielded comparable results, with SUVLBMJanma showing slightly lower a/b ratios, indicating marginally greater independence from body weight. These differences, though statistically small, suggest that SUVLBMJanm may be preferable for achieving more consistent SUV measurements, particularly in diverse patient populations with varying body compositions.
These findings confirm that LBM-based normalisation is superior for quantitative analyses in [1⁸F]mFBG PET-CT imaging. Prior studies on [1⁸F]FDG PET imaging in adult populations have demonstrated similar advantages of LBM adjustments in reducing weight dependency [13,14,15, 18, 19]. Our findings expand knowledge to paediatric patients, where limited research exists on SUV normalisation methods, and align with recommendations from PERCIST 1.0 for oncologic PET imaging [10]. Direct LBM measurements from CT scans are not yet available in PET-CT analysis. For this study, we used SUVBW, SUVLBMJanma, and SUVLBMJames because they are routinely available in PET viewing software. Future advancements in automatic CT-based LBM estimation could refine SUV normalisation. Although predictive LBM models such as James and Janmahasatian improve SUV normalisation, direct PET-CT-derived LBM measurements could provide a more individualised and precise alternative. Future developments in automatic CT-based LBM estimation may allow for real-time assessment of body composition, particularly in patients undergoing treatment-related muscle loss or growth-related changes in pediatric populations.
Similar to [1⁸F]FDG, we did not observe any measurable uptake of [1⁸F]mFBG in adipose tissue. This absence of uptake explains why SUVBW tends to overestimate SUV values, particularly in patients with higher fat mass, as the BW-based formula includes non-metabolic adipose tissue, leading to artificially inflated SUV measurements. In contrast, LBM-based normalisation provides a stronger correlation with reference tissues because it accounts only for metabolically active compartments of the body, thereby reducing variability and weight dependency. This further reinforces the use of LBM-adjusted SUV methods for more accurate quantification in [1⁸F]mFBG PET-CT, particularly in patients with variable body compositions.Although both LBM normalisation methods (SUVLBMJanma and SUVLBMJames) reduced variability and weight dependency compared to BW normalisation, only minor differences were observed between these LBM normalisation formulas. For instance, SUVLBMJanma consistently resulted in slightly lower a/b ratios compared to SUVLBMJames across all reference tissues, suggesting marginally greater weight independence. However, these differences were minor.
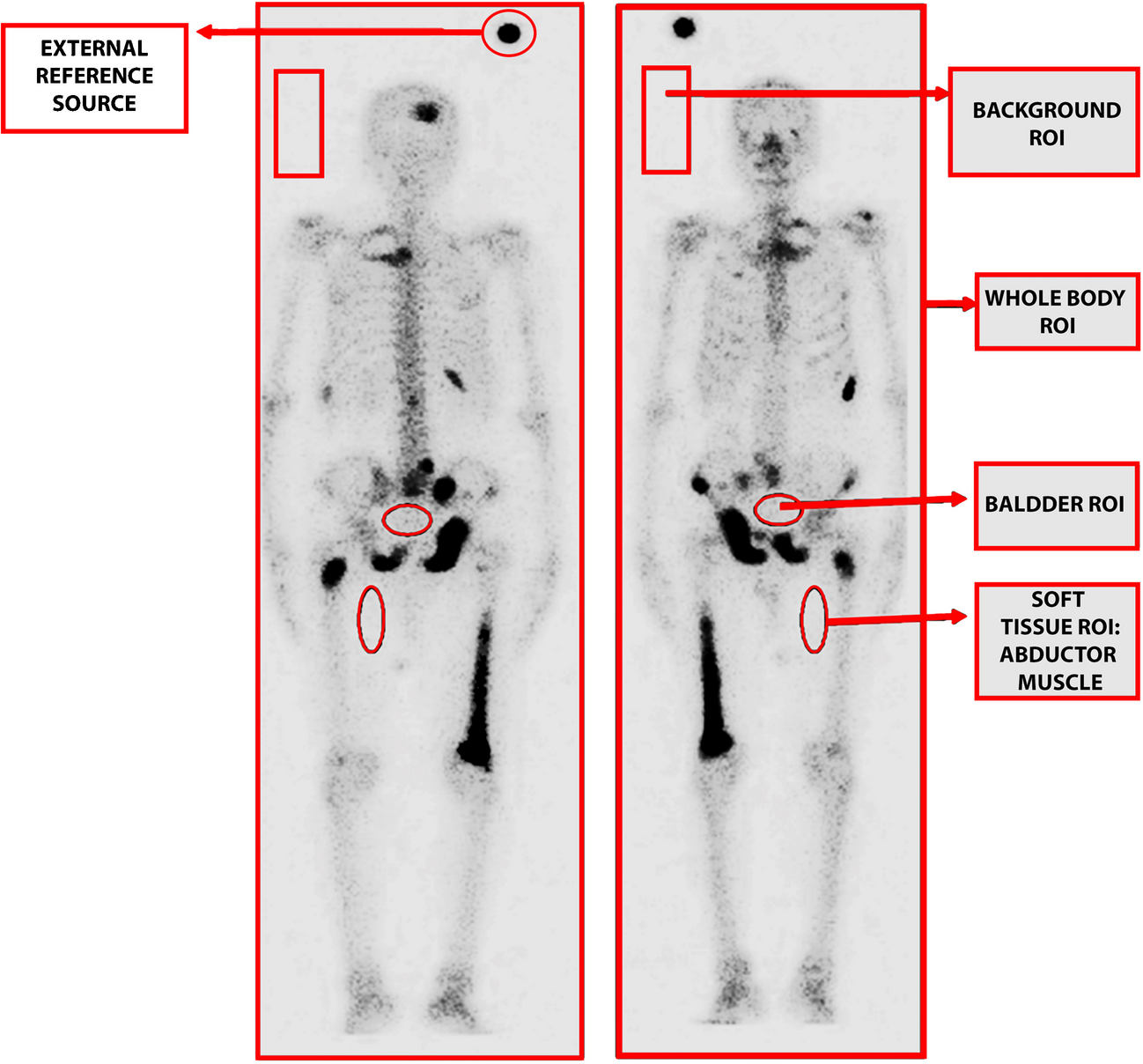
The differences in SUV uptake across reference tissues have important implications for [1⁸F]mFBG PET-CT quantification. The liver exhibited high uptake, often exceeding lesional SUV levels, making it unsuitable as reference tissue due to the risk of overestimating pathological uptake. Additionally, unexplained differences in uptake between the left and right liver lobes, along with metabolic activity variations and physiological fluctuations, may introduce additional inconsistencies. The blood pool had the lowest SUVs, potentially leading to false positive bone marrow assessments if used as a reference tissue. In contrast, bone marrow exhibited stable and reproducible SUVs, with minimal dependency on body weight, supporting its use as the preferred reference tissue in cases where diffuse bone marrow involvement is not suspected. However, if diffuse or multifocal bone marrow involvement is present or suspected, as is often the case in neuroblastoma patients, muscle serves as a good alternative reference tissue. Muscle displayed moderate uptake levels with relative low variability. These findings highlight the importance of selecting a reference tissue that minimises interpatient variability while maintaining reliable SUV quantification.
The integration of LBM-adjusted SUVs and bone marrow as a reference tissue for [18F]mFBG PET-CT has the potential to enhance therapy response assessments in neuroblastoma and phaeochromocytoma. LBM-adjusted SUVs reduce variability and body weight dependency, offering more consistent quantitative measurements within patients over time and across patients. Bone marrow, with its low variability and balanced uptake, provides a robust baseline for detecting changes in pathological uptake, particularly in skeletal metastases. Standardising LBM-adjusted SUV measurements and using bone marrow as a reference tissue may improve response assessment by reducing variability in SUV quantification. This could enhance the accuracy of distinguishing physiological uptake from residual disease and support the development of standardised response criteria in multicentre trials. These advantages may facilitate improved accuracy in treatment monitoring and outcomes assessment in both paediatric and adult oncology patients.
This study benefits from a relatively large cohort of [1⁸F]mFBG PET-CT imaging, including both paediatric and adult patients with diverse demographics in terms of age, gender, and tumour types. Standardised imaging protocols ensured consistency across datasets, enhancing the reliability of the findings. However, several limitations must be noted. Including two different tumour types may have influenced results, however, the sample size was insufficient for stratification by tumour type. Additionally, the overall sample size (63 scans from 35 patients), particularly the paediatric subgroup (46 scans from 20 patients), may limit the statistical power of the findings. While this study provides valuable initial insights into SUV normalisation and reference tissue selection, a larger multicenter dataset would strengthen statistical robustness and generalisability. Future studies should aim to validate these findings in larger cohorts, such as those reported in Wang et al. for neuroblastoma patients, to further support clinical applicability [3]. Multiple scans per patient may have introduced bias, although these reflect distinct functional or metabolic states during treatment. Undetected lesions in reference tissues, despite exclusion of patients with liver metastases, could have influenced SUV measurements. Blood pool measurements may have been less reliable due to smaller sampling volumes. While the James and Janmahasatian formulas are widely used for SUV normalisation, they were developed based on adult body composition data and do not fully account for the dynamic changes in muscle and fat proportions during pediatric growth. The Peters formula has been proposed as a more suitable alternative for children under 14 years old, as it is based on extracellular fluid volume estimation rather than weight-based models [20]. However, normalisation to the Peters formula is not currently available in standard PET viewing software, which limits its practical implementation in clinical imaging. Future research should explore the integration of pediatric-specific LBM models, such as the Peters formula, into PET software to improve SUV normalisation accuracy in young patients. While the Peters formula provides a pediatric-specific alternative to adult-derived LBM models, direct CT-based LBM measurements would allow for a more precise, individualized approach in both pediatric and adult patients. The feasibility of integrating both paediatric and imaging based assessments into PET analysis workflows should be explored.
Additionally, our study did not explicitly assess gender-based differences in SUV normalisation, although the James formula applies different mathematical models for males and females. Variations in weight coefficients and quadratic adjustments could introduce minor differences in SUV calculations, particularly in pediatric patients undergoing developmental changes. While previous studies suggest that James-based LBM estimations may perform slightly better in females[18], further research is needed to determine whether gender-specific differences in LBM estimation significantly affect SUV normalisation in [1⁸F]mFBG PET-CT. Future studies with larger cohorts should explore this aspect to refine SUV normalisation strategies further. Furthermore, the assumption that norepinephrine transporter (NET) expression remains constant may not account for potential physiological changes in [1⁸F]mFBG uptake with age or weight. Finally, differences in reconstruction protocols between adults and paediatric patients (4.0 mm vs. 4.5 mm Gaussian filtering) may influence SUVmax and SUVpeak. Moreover, variations in PET-CT reconstruction algorithms across different imaging centers may further impact SUV comparability. The European Association of Nuclear Medicine (EANM) has developed updated harmonisation strategies through the EANM Research Ltd (EARL 2) program to improve cross-scanner reproducibility [21]. Future studies should validate SUV normalisation methods across multiple PET-CT systems in accordance with these standardisation guidelines to enhance consistency and clinical applicability. However, SUVmean, which was the primary focus of this study, is less sensitive to such differences, minimizing their impact on the study's conclusions. Future studies could further investigate the influence of gender-specific body composition differences and reconstruction protocols on SUV variability, particularly for SUVmax and SUVpeak.

Comments (0)