Study sample
We conducted an exploratory study and invited all patients who were enrolled at the inpatient and daycare unit of the Department of Psychosomatic Medicine and Psychotherapy at the University Hospital Erlangen, Germany, between September 2019 and March 2020 for participation. Inclusion criteria were age ≥ 18 years, sufficient German language proficiency, and regular admission for an inpatient or daycare unit treatment. Exclusion criteria were acute psychotic disorder, degenerative brain disorders (e.g. Alzheimer’s disease), acute suicidality, and current substance dependency. This strategy resulted in the inclusion of 67 individuals (54 females, 13 males, average age 39.6 years ± 14.5, range from 21 to 67 years). During the first two days of enrollment, a structured clinical diagnostic interview was conducted by trained psychologists. Before starting treatment and at the last day of enrollment, patients completed the psychometric assessments using an electronic system, and blood was drawn for biological analyses. Patients received intensive psychosomatic-psychotherapy treatment for eight weeks including an adjustment of psychotropic drug administration if appropriate. About half of patients received antidepressant medication (53.6%). Most patients received a monotherapy of selective serotonine reuptake inhibitors (SSRI, N = 8), a monotherapy of selective serotonine and norepinephrine reuptake inhibitors (SSNRI, N = 5), or a monotherapy of noradrenergic and specific serotonergic antidepressants (NaSSA, N = 2). Five patients took a combination of a SSRI/SSNRI or NaSSA and a tricyclic antidepressant agent, and 2 patients took a combination of a norepinephrine-dopamine reuptake inhibitor and a SSNRI or NaSSA. Anti-inflammatory medication was applied to 21.4% of patients. 12 patients received anti-inflammatory drugs (NSAIDs, corticosteroids, monoclonal antibodies, or mesalazine) during the observation period (Table 1). 11 patients did not indicate their medication. This inpatient and daycare psychotherapeutic treatment is special for Germany, and health insurances reimburse expenses. Only those individuals who participatedat both time points were included in the analysis in order to provide longitudinal data. The study was approved by the Ethics Committee of the Friedrich-Alexander-University Erlangen-Nürnberg (FAU, ID 200_19 Bc) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Table 1 Socio-demographic and clinical characteristics of included patients. NSAIDs, nonsteroidal anti-inflammatory drugs, SSRI, selective serotonine reuptake inhibitors, SSNRI, selective serotonine and norepinephrine reuptake inhibitors, NaSSA, noradrenergic and specific serotonergic antidepressantsBlood collection and cortisol measurement
Blood was collected at 8 a.m. in the morning after overnight fasting to minimize circadian and nutritional effects. To obtain blood plasma, whole blood was collected into EDTA-containing vials (Sarstedt, Germany), centrifuged for 10 min at 2000× g at room temperature, aliquoted, and stored at − 80 °C for later assays. Samples were processed within two hours. Cortisol was quantified at the Central Laboratory of the Universitätsklinikum Erlangen, Germany (DIN EN ISO 15189 accredited) from separately collected vials using an electro-chemiluminescence immune assay (Elecsys Cortisol II Kit) on a cobas e801 device (Roche, Switzerland).
Psychometric assessment
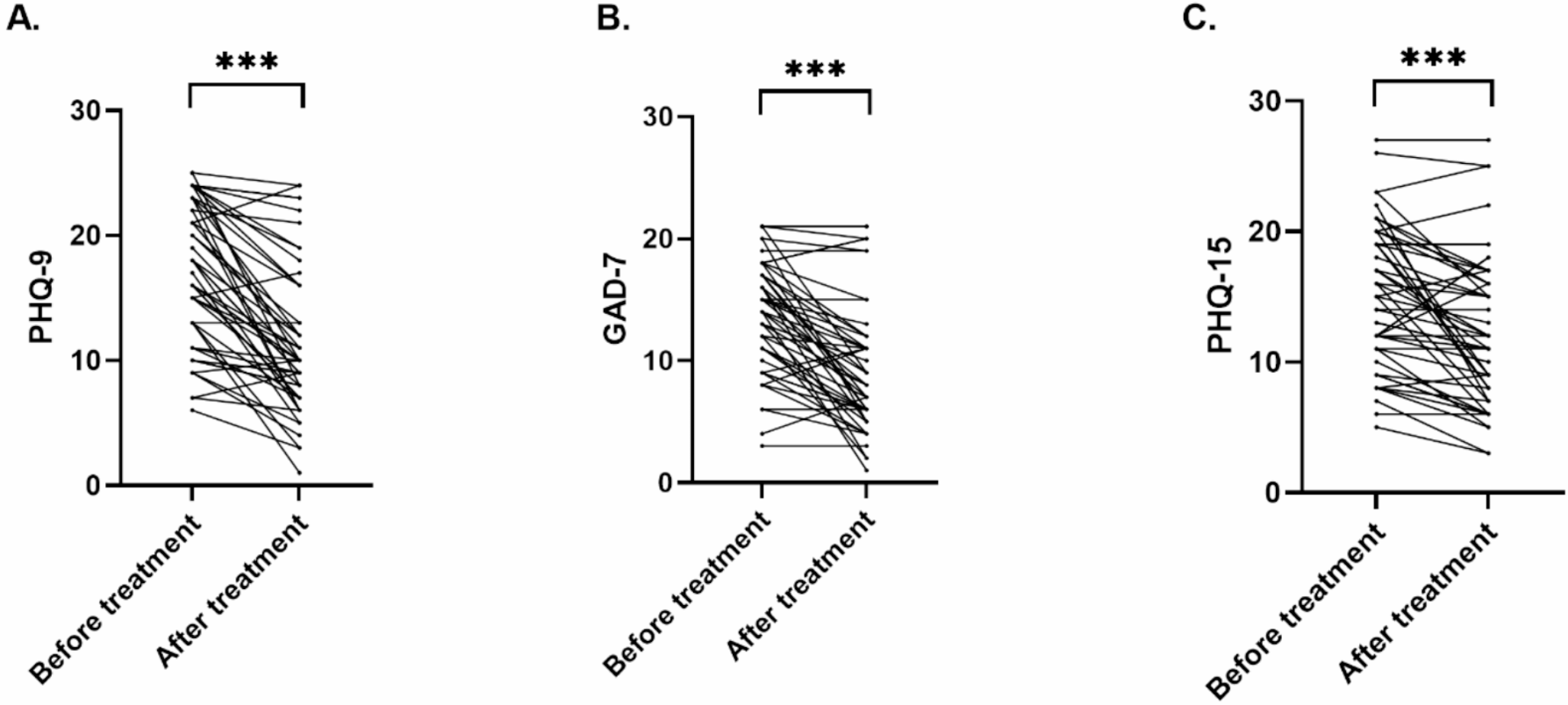
For obtaining a standardized diagnosis, trained psychologists conducted the structured clinical interview MINI-DIPS (Diagnostisches Interview bei psychischen Störungen, in German only). To assess the symptom severity of mental disorders before and after treatment, we conducted the German version of the Patient Health Questionnaire (PHQ-D, Gesundheitsfragebogen für Patienten; [34]) that includes subscales to assess symptom severity of depression (PHQ-9), somatization (PHQ-15) and generalized anxiety (GAD-7) [35] using an electronic system.
Psychosomatic treatment
Patients received a multimodal group-based therapy [35, 36]. Techniques of both cognitive behavioral and psychodynamic psychotherapy were applied. Weekly psychotherapeutic elements were psychotherapy in individual (1 × 50 min) and group (2 × 100 min) format, skills training (2 × 60 min), mindfulness and relaxation methods (2 × 50 min), art therapy (1 × 120 min), Concentrative Movement Therapy (1 × 120 min), and psychopharmacological therapy, if appropriate. Standardization and quality of treatment was controlled by weekly team meetings and internal and external supervision of the whole therapeutic team.
Enzyme activity assays for sphingomyelinases and ceramidase
The activity of sphingolipid enzymes was quantified in blood plasma using fluorescent substrates, BODIPY-FL-C12-Sphingomyelin (D-7711, Invitrogen, Carlsbad, CA, USA/Life Technologies, Grand 15 Island, NY, USA) for secreted ASM (S-ASM) [37] and NSM [38] and NBD-C12-ceramide (Cay10007958-1, Cayman Chemical, via Biomol GmbH, Hamburg, Germany) for NC as described previously [37]. Briefly, the reaction was performed in 96 well polystyrene plates with 58 or 50 pmol fluorescently labelled SM or Cer, respectively, in a buffer mix totaling 50 µl in volume. The reaction was initiated by the addition of 6 µl of a 1:10 dilution of plasma in physiological 154 mM NaCl solution. After incubation at 37 °C for 6–48 h depending on the enzyme, reactions were stopped by freezing at − 20 °C and stored until further processing. For direct chromatography, 1.5 µl of the reaction was spotted directly without further purification on silica gel 60 thin layer chromatography plates (ALUGRAM SIL G, 818232, Macherey-Nagel, Düren, Germany). Product and uncleaved substrate were separated using ethyl acetate with 1% (v/v) acetic acid as a solvent for all enzymes. Spot intensities were detected on a Typhoon Trio scanner and quantified using the ImageQuant software (GE Healthcare Life Sciences, Buckinghamshire, UK). All enzyme activity assays were carried out with four replicate dilutions of each sample and using the same lot of reagents and consumables and performed by a single operator.
Sphingolipid quantification by liquid chromatography tandem-mass spectrometry (LC-MS/MS)
Blood plasma (20 µl) was subjected to lipid extraction using 1.5 ml methanol/chloroform (2:1, v/v) [39]. The extraction solvent contained d7-sphingosine (d7-Sph), d7-sphingosine-1-phosphate (d7-S1P), ceramide C17:0 (Cer17:0) and sphingomyelin C16:0-d31 (SM16:0-d31) (all Avanti Polar Lipids, Alabaster, USA) as internal standards. Sample analysis was carried out by liquid chromatography tandem-mass spectrometry (LC-MS/MS) using a 1260 Infinity HPLC coupled to a 6490 triple-quadrupole mass spectrometer (both Agilent Technologies, Waldbronn, Germany) operating in the positive electrospray ionization mode (ESI+). Analytes were measured by multiple reaction monitoring (MRM) as described [40]. Quantification of Cer and SM sub-species (fatty acyl chain lengths: 16:0, 18:0, 20:0, 22:0, 24:0 and 24:1), as well as Sph and S1P was performed with MassHunter Software (version 10.1, Agilent Technologies). Sphingolipid plasma levels are expressed as “pmol/20 µl” or molar ratios.
Statistical analysis
We examined changes between both time points using paired t tests or Wilcoxon matched-pairs signed rank test after testing for normality of differences. ANOVA with repeated measures was applied when co-factors were included. We corrected for multiple testing using the Benjamini-Hochberg method [41], corrected for 15 tests and report corrected p values in the results section. The significance level was set to 0.05. A statistical trend was defined for significance levels up to p = 0.1. Figures show mean values and standard deviation (SD). Statistical analyses were performed using R V 4.2.0 [42], GraphPad Prism, and IBM SPSS Statistics version 21.



Comments (0)