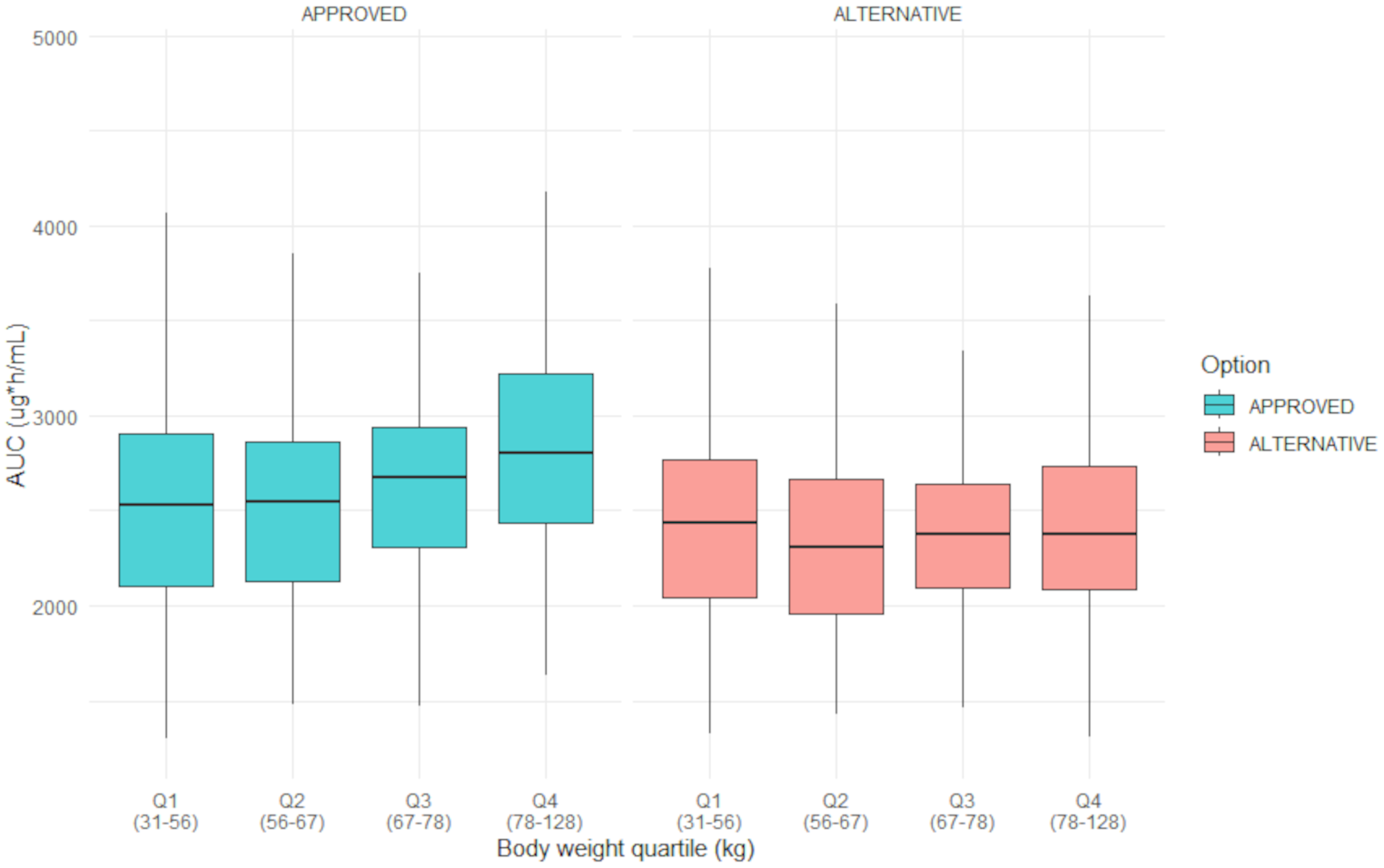
Our investigation shows that an alternative dosing regimen based on weight-bands for enfortumab vedotin will reduce drug spillage and reduce drug expenses. Up to 20% of drug costs can be saved while maintaining an equivalent exposure for the population across the weight range. Moreover, the observed exposure appears more evenly distributed across the bodyweight range in the alternative regimen compared to the approved regimen. The pharmacokinetic variability with this weight-band dosing regimen does not increase and shows that variability does not increase with weightband dosing compared to linear mg/kg dosing.
The predicted GMRs of the AUC and Ctrough of the alternative dosing regimen lie within the equivalence boundaries for drugs with a narrow therapeutic window. In our analysis, the reduction for all calculated AUC and Ctrough for the whole population in the alternative dosing regimen were less than 10%. In the exposure-response analysis performed by the manufacturer, no statistically significant exposure-efficacy relationship was found for OS. However, a positive trend was observed for the response rate for all exposure quartiles. In this analysis, the average concentrations (Cavg) was used as the exposure metric [25]. Although this metric can be linked to AUC, other metrics, such as Cmax and Ctrough, were not explored. Additionally, exposure levels of MMAE based on Cavg negatively correlated with OS [25]. Due to the absence of a significant exposure-efficacy relationship for OS and the observed response across the studied dosing range of 0.5 mg/kg to 1.25 mg/kg, the slight reduction in exposure is unlikely to impact efficacy [14, 25,26,27]. Moreover, in the exposure-response analysis a significant exposure-toxicity relationship was observed. Patients in higher body weight quartiles had a relatively greater exposure, leading to an increased safety risk [14, 25, 28]. Specifically, enfortumab vedotin-induced peripheral neuropathy is a common adverse event leading to potentially permanent symptoms and disability, and which could significantly impact treatment adherence and interfere with long-term treatment outcomes [14, 28]. In our analysis, the proposed alternative dosing regimen resulted in a slight reduction in exposure for the population and a more even distribution across all body weight quartiles, which may improve safety and lower the risk of adverse events. This also implies some nuance to the conclusion by the manufacturer that a weight-based dosing regimen suggests a smaller variability in exposure compared to fixed dosing. In their exposure-response analysis, the weight-based dosing regimen was compared to a fixed-dose of 95 mg (based on an average body weight of 75 kg) [25], as opposed to the proposed rounded weight-band dosing regimen in our study. In addition to the accordance of the exposure metrics of the alternative dosing regimen with the FDA guideline for PD-1/PD-L1 inhibitors, the used equivalence boundaries of 90–111% in our analysis are conservative. Since our analysis relied on the pharmacokinetic model provided by the manufacturer and employed conservative criteria for equivalence, we propose that this dosing regimen can be readily implemented in clinical practice. Analogous dosing regimens developed through modelling and simulation for PD-1/PD-L1 inhibitors are endorsed by FDA guidelines, supporting their implementation [18].
Major advances in anticancer therapy developments with a hefty price tag support the need for cost reduction. The ADCs are an emerging class of potent anticancer drugs that provide highly effective therapy advances in the treatment of hematologic and solid malignancies. Coupled with these advances are economic challenges related to the ability to pay for these therapies together with the growing number of eligible patients and the expansion of approved indications. Enfortumab vedotin is no exception. In the Netherlands, total costs of enfortumab vedotin monotherapy were over €2,300,000 in 2023 [29]. Although the results of the phase 3 study in combination with pembrolizumab are impressive, the addition of pembrolizumab will even further increase drug expenses [9]. Furthermore, the shift to first-line therapy will increase the number of eligible patients. It is estimated that in the Netherlands alone around 1,200 patients with advanced or metastatic UC per year will be eligible for the first-line combination therapy [30]. Based on a median 12 cycles per patient [9], the total costs per patient are estimated to be € 152,411.04 and in total more than € 182,000,000 per year, from a Dutch perspective, with long-term responders having even a more pronounced effect on costs [24, 30]. This emphasizes the need to optimize the cost-effectiveness of enfortumab vedotin treatment and further reduce the drug costs without compromising effective exposure. In our analysis, a reduction at the 1.25 mg/kg dose level of 15% could be achieved. This could lead to cost savings up to approximately € 22,000 per patient based on whole vials, and a reduction of € 27.000.000 each year from a Dutch perspective. When conducting a cost-effectiveness analysis based on our proposed alternative dosing regimen, all factors remain the same with the exception of the drug costs. Since drug costs will be lower, the alternative dosing regimen will have a higher probability to be cost-effective. Since drug prices of enfortumab vedotin and the variation in body weight may vary across countries, the reduction in costs could potentially be even greater. For example, body weight in the United States of America is generally higher, thus the cost savings of the alternative dosing regimen on a population level will be greater with an increasing body weight [31].
In addition to the cost savings, using rounded doses based on weight-bands and the use of whole vials can have added benefit in reducing drug spillage compared to individual weight-based dosing with partially used vials. In clinical practice, it may happen that a drug has already been prepared, but the patient is not able to receive the drug. In the case of individual weight-based dosing, the prepared infusion bag will be thrown away, whereas with a rounded dose, the infusion bag could potentially be used for another patient with a similar body weight.
In conclusion, this study shows that drug costs and drug spillage of enfortumab vedotin can be reduced by using a weight-based dosing regimen while maintaining an equivalent exposure and achieving a more evenly distributed exposure across the body weight range. Although potential cost reduction and waste avoidance begins with the manufacturer, the possibilities that are provided with alternative dosing regimens should be further explored by both clinical healthcare providers and government. Since the costs of enfortumab vedotin together with the growing number of patients that are eligible for combination therapy with pembrolizumab are substantial, implementation of the presented alternative dosing regimen should be considered.


Comments (0)