We have presented two clinical cases of patients who have received post-operative 5-FU based chemotherapy after having received liver transplantation. There is limited accumulated knowledge concerning differences in toxicity profile of this group of patients compared with those who did not receive liver transplantation.
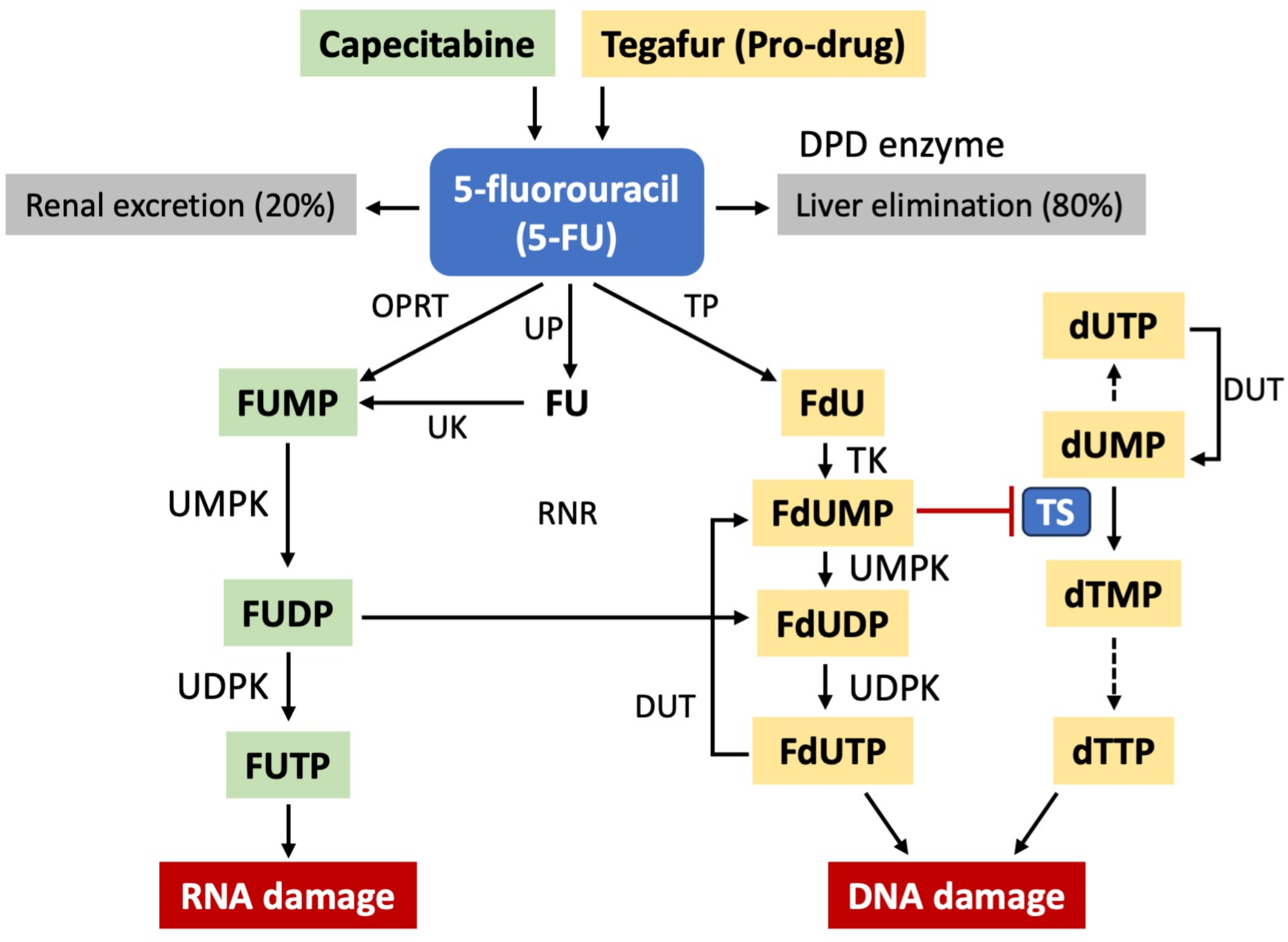
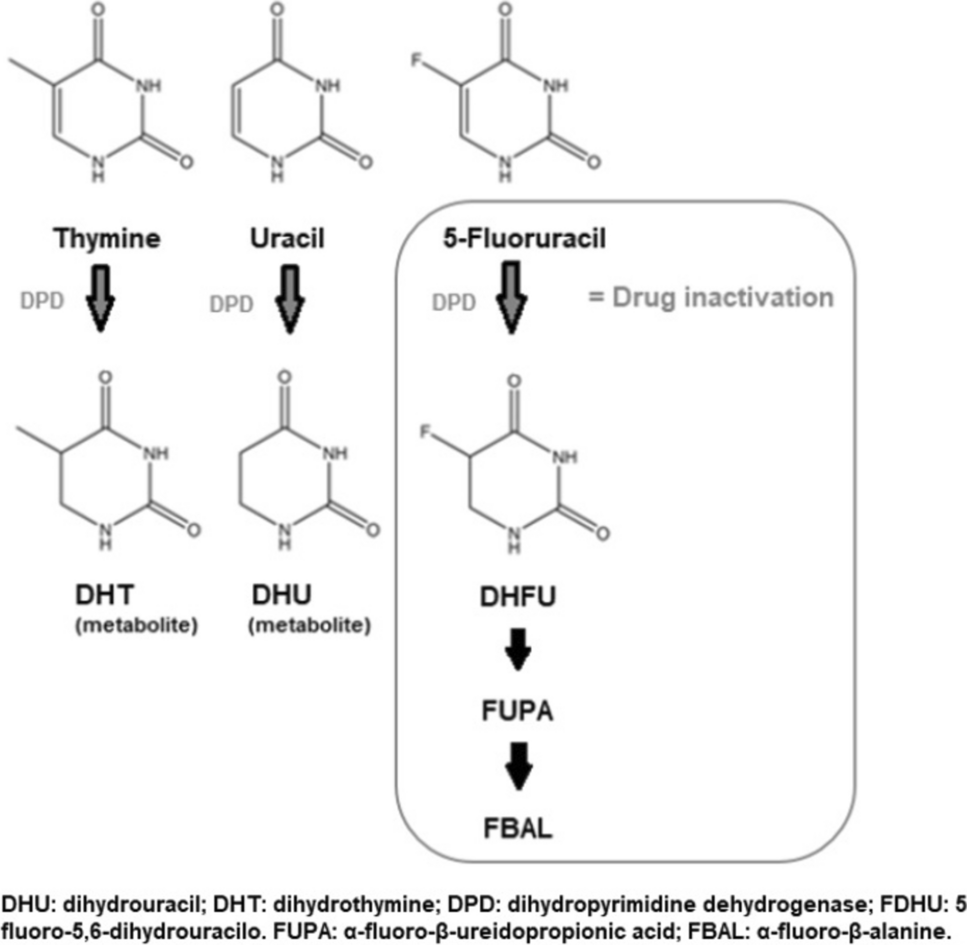
5FU-based chemotherapy is a mainstay of treatment for patients with either colorectal, gastric, pancreatic and biliary tract cancer, both in the palliative and adjuvant setting [26,27,28,29]. It has been extensively proven in past studies how 5FU metabolism is mainly mediated by the liver: indeed, less than 1% of administered 5-FU is turned into active metabolites whereas the remaining portion of the drug is excreted by the kidneys and more than 80% of it is metabolized in the liver [4].
In most recent trials and everyday clinical practice, Capecitabine has been used as substitute to 5-FU: there are some differences in terms of toxicity compared to standard 5-FU but it has been proven that Capecitabine metabolism is similar to standard 5-FU metabolism once that the oral prodrug has been converted into its active metabolites leading to 5-FU accumulation in the tumor [30, 31].
Several guidelines have included DPD deficiency screening as means to reduce the risk of life-threatening 5FU-based toxicity.
For example, in a previously published study of Laures et al. [32] plasma uracil concentration was able to identify patients with DPD deficiency and who would have higher risk of 5-FU related toxicity: median toxicity score was higher in the unscreened group vs. those patients who underwent DPD activity assessment for each cycle of chemotherapy (0 vs. 1; p < 0.001). Cumulative toxicity score during course of treatment was also higher in the unscreened group (0 [min 0; max 4] vs. 0 [min 0; max 6]; p = 0.0028). This difference in toxicity could be mainly traced to different doses of 5-FU that were administered to patients based on DPD assessment as there was a statistically significant difference in 5-FU dose reductions in patients with DPD-deficiency (1056 ± 351 mg/m2/week vs. 1233 ± 251 mg/m2/week in non-deficient patients p < 0.001).
In another study of Meulendijks [6], baseline high uracil concentration (greater than 16 ng/ml) rather than increased uracil/dihydrouracil concentrations were associated with global severe toxicity (OR 5.3, P = 0.009), severe gastrointestinal toxicity (OR 33.7, P < 0.0001), toxicity-related hospitalisation (OR 16.9, P < 0.0001), as well as fatal treatment-related toxicity (OR 44.8, P = 0.001).
In addition to direct and indirect measurement of DPD enzyme activity, another way to assess DPD activity is based, as we have already stated before, on DPYD polymorphisms analysis:
In a large prospective dutch trial [14], 1181 patients were screened for DPD activity by assessment of DPYD polymorphisms analysis in peripheral blood cells (genotypic approach). Eighty-five patients (8%) were found to be heterozygous DPYD allele variant carriers. Toxicity was higher in patients who were DPYD allele variant carriers (33 [39%] of 85 patients) compared to wild type patients (231 [23%] of 1018 patients; p = 0·0013). In addition to that, 5FU dosing strategy based on DPYD allele variant genotype was able to reduce the risk of 5FU related toxicity: in c.1905 + 1G > A allele carriers the relative risk of toxicity was 1.31 (95% CI 0.63–2.73) when comparing different dosing strategy based on the genotype vs. historical controls. Other alleles were also associated with differences in relative risk of toxicity whenever different dosing strategy based on genotype was not used (no toxicity vs. 4.30 [2.10–8.80] in c.1679T > G carriers, 2.00 [1.19–3.34] compared with 3.11 [2.25–4.28] for c.2846 A > T carriers, and 1.69 [1.18–2.42] compared with 1.72 [1.22–2.42] for c.1236G > A carriers). Authors concluded that for c.1905 + 1G > A and c.1679T > G carriers, a 50% initial dose reduction was adequate whereas for patients with c.1236G > A and c.2846 A > T carriers, it should be investigated a dose reduction greater than 25% that is commonly suggested.
In 2020, the European Medicines Agency (EMA) recommended both methods for pre-treatment DPD deficiency testing in clinical practice: phenotyping using endogenous uracil concentration or genotyping for DPYD risk variant alleles [1]. In Italy, the AIOM-SIF (Associazione Italiana Oncologia Medica – Società Italiana di Farmacologia) Working Group recommends the DPYD genotype test be performed on germinal DNA extracted from peripheral blood to identify DPD deficiency [33]. The mutations under analysis are c.1236G > A (rs56038477), c.1679T > G (rs55886062), c.1905 + 1G > A (rs3918290), c.2194G > A (rs1801160), and c.2846 A > T (rs67376798).
All the studies that have been cited before have included a rather heterogeneous group of patients who were candidate to receive 5-fluorouracil based chemotherapy: however, they can offer only limited insight on what should be done in a patient who received liver transplantation.
As previously stated, DPYD genotyping is able to accurately describe DPD liver activity, as it has been shown to have good correlation between DPYD assessment in peripheral blood cells and DPD activity in the liver [8]. However, DPYD genotyping would not be informative for DPD liver activity in a patient who underwent liver transplantation, as the genotype of peripheral blood cells would reflect the genotype of the explanted liver, rather than the donor’s liver.
Based on these assumptions, phenotypic approach might then be considered as the best alternative to genotypic approach as plasma uracil levels would reflect fluoropyrimidine metabolism of the transplanted liver similarly to patients who have never received liver transplantation.
There are, however, a few factors that might reduce the usefulness of phenotypic approaches for DPD assessment in liver transplanted patients; in particular, indirect methods based on plasma uracil methods might have less reliable results due to the frequent occurrence of confounders:
Decreased estimated glomerular filtration rate (eGFR) lower or equal to 45 ml/min was associated to an increase of plasma uracil concentrations leading to an increase of falsely positive results of DPD deficiency assessment when performed with this method [34].
Indeed, patients with gastrointestinal cancer have impaired renal function due to pre-existing conditions of loss of fluids, thus reducing the accuracy of plasma uracil concentration as form of DPD activity assessment: a large retrospective French study [21] showed that 12.7% of Caucasians had uracilemia greater than 16 ng/mL, suggesting that the phenotypic approach might overestimate the diagnosis of DPD deficiency.
In addition to that, there were also warnings concerning significant differences in measured pretreatment uracil levels, most likely as a result of pre-analytical factors in a large multicenter retrospective analysis [35].
Moreover, looking specifically at patients who received orthotopic liver transplantation, it has been described that in the 50 days following the procedure as much as 25% patients experience an increase in serum creatinine levels [36]. This fact might have a relevant impact on the reliability of plasma uracil testing as way to assess DPD activity, particularly in the time-frame when post-operative adjuvant treatment should be started.
Looking at these data, from a hypothetical point of view, there is a lack of evidence concerning the reliability of standard ways to assess DPD activity, either by phenotyping or genotyping approach, in patients who have received liver transplantation. Indeed, the data concerning not only DPD assessment, but also available evidence on the side effects of 5FU based treatment in patients who underwent liver transplantation is also limited:
Brandi et al. [37] reported the outcomes of a series of patients who underwent liver transplantation for liver metastases from colorectal cancer. In the three cases that were reported, even after having experienced disease relapse thus leading to retreatment with 5FU based chemotherapy combinations, toxicities that were recorded were manageable. There was a general increase in the risk of developing severe chemotherapy related side-effects: one patient experienced G4 neutropenia after having received chemotherapy with FOLFOXIRI post-transplant whereas the most severe toxicity that could be seen before liver transplant was G2 neutropenia; one other patient also experienced G3 neutropenia post-transplant when receiving FOLFOX-based chemotherapy whereas in the pre-transplant setting the most severe toxicity that was recorded was G2 neutropenia.
Lin et al. [38] have published a meta-analysis of adjuvant systemic therapy after liver transplantation for HCC: authors report that adjuvant chemotherapy appears to be well-tolerated. The studies included in the meta-analysis are rather heterogeneous and have also included patients who have received doxorubicin and/or cisplatin based chemotherapy rather than 5FU-based treatment. Description of adverse events was also of anecdotal nature, thus reducing its usefulness in describing accurately the likelihood of toxicity.
In addition to that, prospective or retrospective data from patients with liver metastases who have received chemotherapy after liver transplantation are lacking. For example, in previous clinical trials of liver transplantation in patients with liver metastases from colorectal cancer such as SECA-1 and 2 trials [39, 40] no adjuvant chemotherapy was given after liver transplantation thus limiting our knowledge concerning risk of 5FU toxicity in patients who received liver transplantation.
Finally, the recently published TRANSMET trial [16] reported the outcomes for patients with unresectable liver metastases from colorectal cancer who, after having received chemotherapy, were randomised to continue chemotherapy with or without liver transplantation. The study showed that there was an improvement in overall survival for patients who received liver transplantation against those who just continued chemotherapy (HR:0.37, 95%CI:0.21–0.65, p = 0.0003). However, only 46% patients who received liver transplantation remained free from disease at prolonged follow-up, thus the remaining 54% patients required palliative 5-FU based chemotherapy upon relapse. Authors did not specify whether patients after liver transplantation required “de novo” assessment of DPD activity compared to their initial pre-transplant assessment. Apparently, the risk of chemotherapy-related side effects in patients who received liver transplantation and chemotherapy opposed to patients who continued chemotherapy were not significantly different, albeit authors did not report the safety profile of chemotherapy just after liver transplantation, reporting the safety profile as a whole, thus including also the toxicity that was recorded in the pre-transplant phase.
The two patients that we have reported had received liver transplantation in different clinical settings but were found to have incidental discovery of intrahepatic cholangiocarcinoma (iCCA). To our knowledge, there are no published series reporting the administration of postoperative chemotherapy in iCCA after LT.
As liver transplantation surgery is not currently considered a standard of care and given that our patients have not undergone transplantation in clinical trials, we have deemed transplant surgery to be equivalent to liver resection.
In the cases reported, we recommended adjuvant treatment with Capecitabine monotherapy (1250 mg/sqm twice daily dd1-14 once every 3 weeks for 8 cycles), according to the BILCAP [24] schedule. As we aimed to reduce the risk of side effects from 5FU-based chemotherapy, DPD activity assessment was required before treatment start.
Both patients underwent DPYD polymorphisms analysis on DNA derived from a histological sample of the donor’s liver: plasma uracil concentrations as an alternative way to assess DPD activity were deemed to be inaccurate as they would be influenced by pre-existing hampered renal function.
Indeed, both patients had received liver transplantation in the management of liver cirrhosis and in one patient this was complicated by hepatorenal syndrome that was managed by heterotopic kidney transplantation: creatinine clearance of both patients was altered at baseline but eGFR was in the range as to allow start of Capecitabine based adjuvant chemotherapy. Because of this fact, DPYD polymorphisms assessment in donor’s liver tissue was the only reliable option for DPD activity assessment.
The time required for DPYD polymorphism reporting was 16 days in patient A and 21 days in patient B. Although it required longer times compared to standard DPYD polymorphism analysis (usually around 3 work-days), the time lag was due to the issue of tracing back the histologic specimen of the donor. Time required to have the result of DPD activity assessment did not allow us to start adjuvant treatment within the 8 weeks time-frame since initial surgery. This could be a major issue as it has been previously documented in several tumor types that in treatment beginning within 8 weeks should be preferred, in order to increase the likelihood to benefit from such treatment.
It could be safely assumed that the test would have quicker response times should the histologic specimen of the donor be easily available: recent trials of liver transplantation for liver metastases from colorectal cancer such as COLT trial [39] have already managed this issue by means of donor’s liver tissue storage, albeit in an ancillary sub-study. Based on this fact, we suggest that proper handling and storage of the pre-transplant liver biopsy should be done. This would allow to minimize the time required to have the result of this analysis as most of the time lag of the procedure was due to handling and shipping of the histologic specimen, rather than the test itself.
Both assessment resulted to be wild-type and allowed start of Capecitabine-based chemotherapy at full-dose (1250 mg/sqm twice daily for 14 days out of a 21 days period).
Both patients were able to complete 8 cycles of post-operative chemotherapy, albeit dose reduction were required: In patient A, due to increase of creatinine and worsening of renal function, dose of Capecitabine had to be reduced from 1250 mg/sqm bid to 1000 mg/sqm bid. The worsening of renal function was attributed to the fact that the patient had also received heterotopic liver transplantation for hepatorenal syndrome, rather than Capecitabine based toxicity. Indeed, eGFR remained stable throughout the rest of treatment and no severe side effects were recorded. In patient B, due to decrease in platelet count, dose reduction and dose delays were required: it must be noticed however that this patient started treatment with low platelet count due to splenomegaly and thus the impact of Capecitabine on platelet count was marginal.
There is limited evidence on the effectiveness of fluoropyrimidine treatment after LT, with the largest examples coming from studies on adjuvant chemotherapy after liver transplant for hepatocellular carcinoma and unresectable liver metastases of colon cancer [37, 41, 42]. However, none of these studies mention the method used to assess DPYD polymorphisms. Therefore, there are no evidence-based recommendations for managing patients with this complex presentation.
In the medical literature, there is only one other published case that tried to assess DPD deficiency in patient that required 5-FU based chemotherapy after LT [43]. This case involved a patient who had undergone LT to treat end-stage liver disease caused by primary sclerosing cholangitis.
The patient was later diagnosed with pancreatic cancer and needed fluoropyrimidine-based chemotherapy. However, the patient’s liver donor genotype was unknown and testing the DPD activity in peripheral blood cells was not indicative of liver activity due to different genotypes; the medical team proposed the use of therapeutic drug monitoring to ensure the patient’s safety.
During the first cycle of chemotherapy, the researchers reduced the initial dose of the 5-FU components by 30% and monitored the patient’s plasma concentration of 5-FU. Based on this result and the patient’s clinical observations, they were reassured that the patient did not have a severe DPD deficiency.
In this case, authors opted for monitoring 5-FU plasma concentrations as means to reduce the risk of toxicity instead of performing donor liver DPYD genotype as in our two patients. We believe that, owing to the increased number of patients who would be candidate to liver transplantation and who would require post-transplant 5-FU based chemotherapy, assessment based on 5-FU plasma concentration would not be feasible and sustainable: due to changes in patient’s liver conditions between different cycles of chemotherapy, drug monitoring would have to be done for each cycle of chemotherapy instead of just performing transplanted liver tissue DPYD genotyping only once before treatment. An increased number of patients would require a lot of resources just for this assessment and that would not be feasible to do in routine clinical practice.
In addition to that, the patient that was reported did receive polychemotherapy with FOLFIRINOX regimen: there are two additional limitations to drug monitoring as means to prevent treatment related side-effects that would be overcome by liver genotyping:
First of all, patient treatment schedule (once every 2 weeks) allowed for a reliable form of assessment of 5-FU circulating doses in the immediate time following chemotherapy infusion. On the other hand our patient received Capecitabine monotherapy continuously for 2 weeks out of a 3 weeks period: the prolonged exposure to Capecitabine would lead to some difficulties in interpreting the results of one single assessment of circulating 5-FU doses, thus making this form of testing as means of prediction of 5-FU toxicity less relevant.
Secondly, the patient received chemotherapy with FOLFIRINOX regimen: this chemotherapy combination includes, in addition to infusional 5-FU, also Oxaliplatin and Irinotecan. While Oxaliplatin metabolites are mainly excreted by kidneys and there is currently no evidence that liver cytochrome P-450 mediated metabolism is required [44], Irinotecan is extensively metabolized in the liver by UDP-glucuronosyltransferases (UGT) mediated processes.
Altered UGT gene polymorphisms have been also described to be associated with higher risk of Irinotecan-related treatment toxicity [45].
In order to fully estabilish safety profile of treatment in a liver transplant patient who is candidate to receive both 5-FU and Irinotecan combined, liver genotyping of both DPYD and UGT polymorphisms, by using the method that we described, would be able to manage this issue. On the other hand, by increasing the number of drugs that are used in the combination, drug monitoring would become increasingly more difficult and unfeasible.


Comments (0)