
Remember me



Nosocomial pathogens consist of bacteria, viruses, and fungal parasites. Nosocomial bacterial and fungal infections have become a crucial health-related disaster now in our healthcare community because of the rigidity of patients and the frequent usage of hospital devices or equipment. These infections, also known as hospital-associated infections (HAIs), cause major dilemmas in ICUs. Generally, these infections occur or are identified after the entrance of 48–72 h in the hospitals or within 30 days after getting discharged from hospitals [15]. Hospitalization is responsible for these types of severe diseases or infections and promotes patients' risk of acquiring antimicrobial-resistant pathogens. Nosocomial pathogens can spread from neighboring patients, staff members, or hospital facilities, and patients in ICUs become at high risk. A study including 231,459 patients in 947 hospitals reported that about 19.5% of patients in ICUs are suffering from one of HAI [16].
Types of nosocomial infection: Major symptomatic diseases related to nosocomial infections
(A) Central line-associated bloodstream infections (CLABSI)
CLABSI occurs when pathogens enter the patient’s central line and bloodstream. The catheter insertion or dysfunction during erythema or purulence causes infection due to the bloodstream infection (BSI) after removal of the catheter within 48 h, which may lead to illnesses such as endocarditis, osteomyelitis, abscess, suppurative thrombophlebitis, and septic arthritis. Based on studies, some bacteria are listed as causing CLABSI, such as Candida species, S. aureus, Enterococcus species, coagulase-negative Staphylococcus, E. coli, Bacteroides species, and Streptococcus species [17].
(B) Catheter-associated urinary tract infections (CAUTI)
CAUTI relates to different urinary tract infections. However, they can happen with intermittent catheterization, indwelling suprapubic catheters, and catheter removal within 48 h. The primary infectious pathogens are the microflora from fecal and skin. Researchers have listed the most frequent CAUTI pathogens as E. coli, Enterococcus spp., K pneumoniae, Candida species, and P. aeruginosa [18].
Urinary tract infections (UTIs)UTIs are at the top among nosocomial infections and are reported at 40% of hospital infections and 34% of nursing home infections. The urinary catheter during by-passes provides a conduit for bacterial pathogens to spread over the bladder, resulting in nosocomial urinary tract infection. The study says that if the patient stays in hospitals for about three or more weeks, there is a higher chance of infection with nosocomial infection [19].
(C) Pneumonia
Nosocomial pneumonia includes hospital-associated pneumonia (HAP) and ventilator-associated pneumonia (VAP). HAP generally occurs within or after 48 h of hospital entry and can cause aspiration, bacterial translocation, hematogenous spread, and inhalation of contaminated aerosols. VAP can occur in a patient after ventilator treatment to get rid of the respiration problem. Here, some pathogens generally connected to VAP and HAP include P. aeruginosa, Klebsiella oxytoca and pneumoniae, S. aureus, Candida species, Enterobacter species, and Streptococcus species. Common lung disease problems include immunosuppression, abdominal or thoracic surgery, dysphagia, and neutropenia [20].
(D) Surgical site infection (SSI)
SSI occurs within or after a month of hospital admission while fitting prosthetic products. Symptoms of infection, like warmth, erythema, wound dehiscence, and pain, have been seen in SSI. Infection may be obscured and manifested with high systemic signs, such as rigors, fever, and leukocytosis. Risk factors associated with patients are immunosuppression, obesity, malnutrition, hyperglycemia, tobacco, rising age, and joint pain. Pathogens related to SSI are S. aureus, Klebsiella species, and E. coli. Streptococcus species, Coagulase-negative Staphylococcus, Enterococcus species, and Enterobacter species [21].
(E) Clostridium difficile infection (CDI)
CDI occurs after three days of hospital admission with symptoms related to unformed stools. The patient releases stools three or more indistinct in 24 h. Diarrhea is the most prominent symptom of CDI, and some others, such as distention, fever, anorexia, abdominal pain, dehydration, and nausea. C. difficile is a frequent pathogen associated with HAI [22].
Bacterial pathogensBacteria are the most frequent pathogens causing nosocomial diseases or infections. They may be interrelated to the patient's natural flora and infect only when they become ready to get infections. Gram-positive bacteria affect the bloodstream and cause other infections, such as skin infections in hospital-admitted patients, which are fatal. The frequent and comprehensive use and abuse of antibiotics have led to the initiation of drug-resistant bacteria, also known as superbugs, and they become insensitive to mainly known antibiotics [23]. The most common nosocomial bacterial pathogens are A. baumannii, C. difficile, P. aeruginosa, K. pneumoniae, S. aureus, etc. [12]. They also became resistant to numerous antibiotics like Aminoglycosides, Imipenem, Meropenem, Ciprofloxacin, Levofloxacin, Erythromycin, Colistin, etc. [24].
Fungal pathogensIn particular, Candida albicans (C. albicans) are a component of the human microbiota, and most nosocomial infections have an endogenous origin. Immunocompromised patients, especially those in critical condition, are susceptible to invasive candidiasis, which includes candidemia, deep-seated infections, and disseminated hematogenous infections [25]. Nosocomial fungal infections will continue to rise in frequency in the upcoming decades due to the increasing frequency of risk factors for these infections. Candida spp., Aspergillus spp., Mucorales, Fusarium spp., and other molds, such as Scedosporium spp., are the most common nosocomial fungal diseases. Antifungal medication does not reduce the significant morbidity and mortality associated with these infections, which are challenging to identify. The pillars of treatment for nosocomial fungal infections continue to be the early commencement of effective antifungal therapy and the correction of underlying host abnormalities [26].
Health and economic burden of AMRDrug-resistant HAIs are now becoming a global health challenge and contribute to significant morbidity, mortality, and financial burden on patients, families, and healthcare systems. A report says an estimated 13.7 million deaths occurred in 2019 because of bacterial infections; 33 bacteria are associated with these infections.[27]. The cost of medications, the number of hospital days and consulting with healthcare professionals, and the demand for laboratory diagnostic services could all be impacted by rising health costs [28]. According to World Bank projections, health expenses due to AMR might increase by $330 billion in the case of a low burden and $1.2 trillion in the case of a high burden [29]. A study revealed that the national costs associated with six common MDR infections can be substantial at more than $4.6 billion annually, followed by C. difficile ($1 billion) in the USA [30, 31].
UA's traditional and modern technologies of extraction and their derivativesUA’s traditional and modern technologies of extractionUA can be extracted and purified from herbs, flowers, leaves, and fruits, either traditionally or in modern technology. Traditional methods include maceration, Soxhlet, and heat reflux; modern methods include microwave, ultrasound, accelerated solvent, and supercritical fluid. The type of solvent and solvent-to-solid ratio, extraction time, and temperature is the main factors affecting the extraction process. These are operational issues that influence yields and rates. However, mechanical and thermal sample conditioning before extraction is a crucial step that needs to be optimized [32]. The extraction of ursolic acid from fruits and medicinal plants has been described mainly for traditional extraction procedures. The method depended on the raw material. The extraction of ursolic acid from seeds has been compared using conventional solvents such as water and lower alcohols and their combinations with water, acetone, diethyl ether, chloroform, hexane, and ethyl acetate [33]. UA can be extracted from various specific parts of medicinal plants. For example, the extraction from leaves of Paulownia fortune was confirmed by a reduction in a fixed time to reach optimum extraction from 20 min with conventional to 5 min with ultramicropowder. The obtained ultramicropowder of the UA was double that of the orthodox powder [34]. Moreover, the subcritical water extraction (SWE) method was used to extract UA from Hedyotis diffusa. This method uses particle size, extraction temperature, time, and solvent/solid ratio. Extraction pressure has been applied to get the optimum extracted material. It was concluded that SWE was more time-managing, cost-effective, and eco-friendly extraction than other traditional methods [35]. Extraction of UA using organic solvent was incompatible with food applications. So, for extraction of UA from apple peel, they prepared fifteen hydrophobic deep eutectic solvents (HDESs); after strategic comparison, they analyzed that HDESs have nine times higher solubility than traditional solvents like ethanol [36].
Strengthening strategiesMicrowave-assisted extraction (MAE) and ultrasound-assisted extraction (UAE) can increase natural product yield and bioactivity. It is a straightforward, fast, and convenient method. Using UAE, the UA was extracted from Neolamarckia cadamba with a high yield [37]. Likewise, MAE and UAE were used to extract phenolic compounds of Salvia fruticose. Modeling and optimization were done using MAE. They used both UAE and MAE to extract chemical contents but found that MAE was much more efficient than UAE [38]. It has been suggested that enzyme-assisted extraction (EAE) is a low-pollution, low-energy method that helps break down cell walls so that solutes are more easily accessible. Cellulase was cultivated to extract ursolic acid from Chaenomeles sinensis [39].
PurificationThe target products with higher purity are usually obtained by further processing the crude solvent extracts. Typically, this involves applying a decolorization stage using diatomite, siliceous earth, or activated carbon, followed by ethanol elution. This process enables the dried product to present a triterpene acid content of more than 50% wt. or above 90%. UA recovery often requires prior adsorption, crystallization, centrifugation, washing, and drying of the extract from the input material. In research, monolithic polymers were synthesized to purify and enrich the content of UA. Additionally, the purification of crude extracts using distilled water, petroleum ether, ethanol ethyl acetate, acetone, and water before precipitation and recovering ursolic acid with 98–99.5% purity has been proposed. This process is known as solvent fractionation [40]. Chromatographic fractionation is another technique used to purify UA from extracts through the reverse column, layer chromatography, microporous adsorption resin, and silica gel column [32]. Another well-known technique to obtain pure UA from oil is the “response surface methodology” [41].
UA derivativesAs per the literature, the UA was used in biology to check their clinical potency. Various chemical and physical parameters decided that the derivatives of UA (1) can also serve as potential therapeutic agents against various infectious agents [42]. A derivative 3β-acetoxy-urs-12-en-28-oic acid (1a) yields after treating UA with acetic anhydride and pyridine at room temperature (RT). The presence of the acetyl group was confirmed by the 1H-NMR spectrum with signal δH 2.05 typical of hydrogen and the 13C-NMR spectrum with the appearance of the signal at δC 170.9. Another derivative, 3β-formiloxy-urs-12-en-28-oic acid (1b), showed an analysis of the 1H-NMR spectrum found a signal at δH 8.12 for the formyl group and confirmed by δC signal at 161.3 attributed to the carbonyl 1b with the combination of kanamycin represented the best synergistic action against the multidrug-resistant E. coli at the concentration of 64 μg/ml, with reduced MIC value from 128 to 8 μg/ml [4]. In derivatives, for the chemical modifications, generally, the hydroxyl group at position C3, unsaturated double bind at position C12–C13, and the carboxylic acid at position C28 in the upper rings of UA have been targeted [43]. Most of the modifications at these sites have been done to increase the potential and bioavailability of the UA and its derivatives. In a study of the UA structure–activity relationship, researchers synthesized 23 derivatives through modifications at positions C3 and C28. From there, one derivative of 3-O-acetyl ursolic acid was obtained from the acetylation of UA, later treated by bromo-diolefin to yield fatty esters. Later, they also synthesized amide and ester derivatives of UA [44]. Researchers examine an effective location to enhance the biological potential. Adding an acetyl group at C3 and an aminoalkyl at C28 helps improve biological potential [45]. To make the derivative's greater power bioactive and bioavailability, another ester derivative was synthesized by esterification with a suitable acid chloride in the presence of a DAMP catalyst. Claisen–Schmidt condensation and Jones oxidation steps were also done at positions C2 and C3, respectively [46]. Numerous studies have reported various UA derivatives in their quest for more beneficial chemicals. These are a few UA analogs that use positions C2, C3, C20, and C28 and have interesting processes linked to infections and diseases that are currently in existence. Castanea crenata Sieb. et Zucc is the naturally occurring source of (2α,3β,7β,23-tetrahydroxyurs-12-ene-28-oic acid), a UA derivative compound. This compound was confirmed by several spectroscopic techniques, such as IR, 1H-NMR, 13C-NMR, and HR-ESI MS [47].
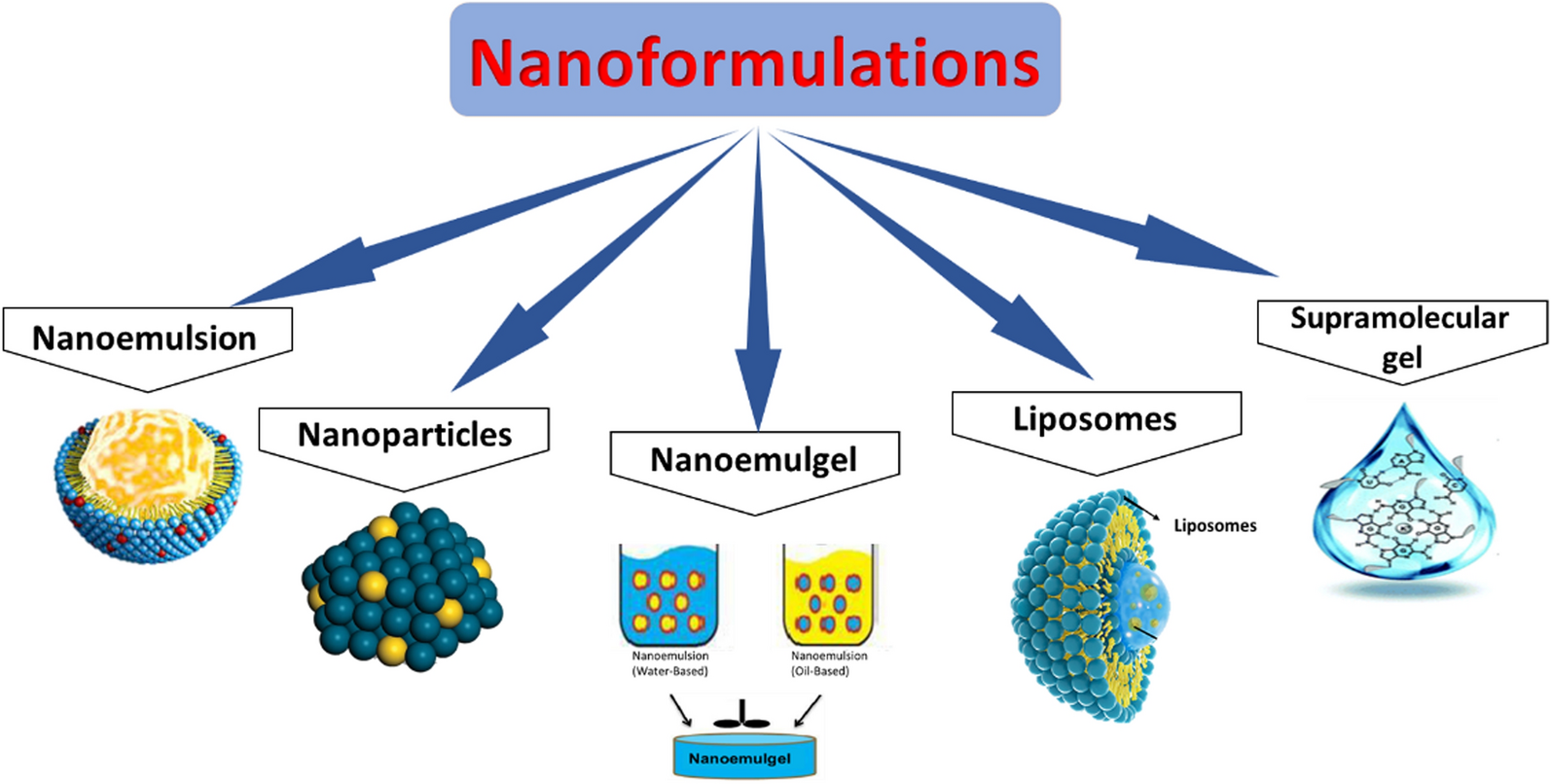
UA and their nanoformulationsPure-extracted compound therapy to treat any infection or disease is not enough after a time. UA is a viable choice for developing a wide range of medical disorders and other life-threatening diseases due to its biological role in developing new therapeutic strategies [48]. Its drawbacks include multidrug resistance, low bioavailability, weak solubility in aquatic environments, and a minor drug loading over colloidal nanocarriers (nanoemulsion, nanocapsules, nanoparticles, nanosheets, nanocrystal, etc.). Nowadays, various formulations of UA with or without any carriers in numerous forms performed by researchers, such as nanoemulgel, nanoparticles, liposomes, microemulsion, hydrogel, polymer micelles, and supramolecular gel, etc. (Fig. 1) [49].
Fig. 1
Different types of nanoformulations
Nanoemulsion: A promising drug delivery method for various medications, including biopharmaceuticals, was mentioned: nanoemulsion. A heterogeneous network called a nanoemulsion comprises droplets of one immiscible liquid dispersed across another liquid. In a nanoemulsion system, the nanoranges of two immiscible liquids, oil, and water, are combined, and suitable surfactants or cosurfactants with a suitable hydrophile–lipophile balance value are added to create a homogenous solution. The nanoemulsion approach is most medications' best drug delivery strategy since it maximizes efficacy while lowering toxicity. The range of this thermodynamically stable system is 10–100 nm. By boosting the absorption of poorly soluble medicines through the skin, extending the time that the drug is processed in the targeted location, and ultimately reducing side effects, nanoemulsion presents a promising alternative for improving the penetration of the drug delivery system and targeting those drugs [50].
Nanoparticles: By improving the solubility and stability of encapsulated pharmaceuticals, facilitating membrane transport, extending the duration of blood residency, localizing medications at the therapeutic site, and demonstrating endosomal escape, nanotechnology enhances the efficacy of treatment [51]. Likewise, UA has low water solubility and bioavailability, preventing it from working to its full potential. Thus, ursolic acid is encapsulated in natural or synthetic polymers to improve its therapeutic efficacy. One natural polymer that has been used to create nanoparticles that increase medicinal efficacy is chitosan [52]. The number of clinical studies focused on nanoparticles for drug delivery is expanding quickly due to the fascinating growth of nanotechnology and advancements in biology and medicine. Certain nanoparticles, such as those based on metal, phytochemicals, polymers, and lipids, can play an important role in vaccine clinical development and production.
Nanoemulgel: This carrier combines a nanoemulsion based on polymeric hydrogel and enhances the topical efficacy of various weak permeable hydrophobic therapeutics. This attracts scientists to innovate novel drugs related to skin disorders because of the excellent penetration power of nanoemulgel. Nanoemulgel can release therapeutic agents successfully and has a promising drug affinity to diffuse from the carrier to cross barriers. While oil droplets from the gel are released, they transfer to the hydrophilic phase. The whole mechanism is based on the inner crosslink density and network of polymer chains [53]. In a study, UA-based nanoemulgel was formulated, confirmed by the texture that includes viscosity, contact and adherence power with skin, spreading power, and soft consistency. UA's release was slow and controlled [54].
Liposomes: Liposomes are spherical vesicles with an aqueous core surrounded by one or more concentric phospholipid bilayers. Liposomes, which are biodegradable and harmless, are an effective drug delivery method for various medications. Using liposomes as a drug delivery technology has capitalized treatments for different biomedical applications by enhancing the biodistribution of chemicals to target areas in vivo, stabilizing therapeutic compounds, and removing barriers to cellular uptake [55]. It has been discovered that the UA causes nonbilayer formations (local structures that resemble cubic or hexagonal shapes) and destroys the layered packing of typical multilamellar vesicles. This trait was explained by the conical geometry of UA–lipid interactions that spontaneously formed in the lipid layers. Since UA and kinase inhibitors share many chemical characteristics, combining the two to implant an inhibitor and UA into lipid bilayers may offer additional benefits for customizing liposomes and creating combination drug carriers [56].
Supramolecular gel: In recent years, there has been a sharp increase in the production of supramolecular hydrogels that self-assemble in water using low molecular weight gelator (LMWG) building blocks. A variety of gels have been created with advanced technological purposes in consideration, such as wound healing, optoelectronics, regenerative medicine, pharmaceutical formulation, energy storage, and environmental cleanup. Gels can be optimized for certain purposes based on their physical characteristics (such as stiffness or porosity) and the chemical programming in the LMWG scaffold [57]. In a study, a new hydrogel based on ursolic acid was created by capturing water molecules in the air and using a straightforward triterpenoid derivative self-assembly process in methanol. The resultant hydrogel has a strong heat resistance, good elasticity, and a porous morphology [58]. Supramolecular gel's interaction with iodine is predicted to be improved by adding electron-rich units, which will also boost the absorbents' ability to capture iodine. The resultant supramolecular gel is perfectly rheological and has a porous shape. Based on data analysis, the amorphous structure of this supramolecular gel can be described by the stacking of π-π between molecules [59].
UA and UA's formulations approach toward pharmaceutical and biological activitiesUA is a naturally occurring substance with a wide range of biological and pharmacological characteristics, making it a promising material for several therapeutic uses. This review presents information on the presence and biosynthesis of this widely distributed, physiologically active molecule, together with the current knowledge about its medicinal qualities. UAs and derivatives' anticancer or antitumor, antibacterial, antiviral, anti-inflammatory, antidiabetic, hepatoprotective, neuroprotective activity, and potential against several life-threatening and chronic diseases have received special attention [60].
Antibacterial: Nosocomial infections with growing multidrug resistance are an emerging problem across the globe, leading to significant morbidity and mortality and affecting public health severely. [61] With the discovery of novel compounds and derivatives that are effective against bacterial infections, there is a belief that using naturally occurring compounds as a substitute will result in a better and more hopeful therapeutic impact [62]. Human chronic infections are lethal; nearly 80% of infections are caused by biofilm-forming bacteria. These bacteria enhance their pathogenicity by reducing the penetration of antibiotics through EPS, mutating at the target site of drug molecules, collecting enzymes that help in enzyme degradation, and stimulating gene expression involved in the efflux pump [63]. Nanotechnology with phytochemicals has become the opportunistic window to combat the AMR problem. In research, a nanocomposite of ursolic acid-loaded chitosan nanoparticles (UA-Ch-NPs) was synthesized, and they found the significant inhibition of nosocomial pathogen S. aureus with the MIC value of 32 μg/ml that is lower than the MIC value of crude UA which is 64 μg/ml [64]. Streptococcus mutans (S. mutans) is a promoting pathogen for dental caries and can form strong biofilm by secreting glucosyltransferases (GTFs), which synthesize the extracellular polysaccharides (EPSs). UA showed potent antibiofilm effects by targeting the substrate of GTFs to halt the secretion of EPSs. Further, it was confirmed by GTF activities, computer simulations, site-directed mutagenesis, and capillary electrophoresis (CE) [65]. UA also showed synergistically biofilm inhibition with xylitol with high efficacy against S. mutans and S. sobrinus in the oral atmosphere [66]. After showing the antimicrobial activity of UA at the MIC value of 0.8 mg/ml against nosocomial pathogen carbapenem-resistant Klebsiella pneumoniae (CRKP), the researcher checked the other parameters involved in inhibition, such as cellular morphology alteration, intracellular pH (pHin) variations, ATP concentration, cellular integrity of the membrane, and biofilm-related gene expressions. They focused on biofilm-related gene target expression evaluated by qRT-PCR. MrkA, luxS, pgaA, wbbM, and wzm gene expression was detected after treating CRKP cells with UA. Four genes, luxS, pgaA, wbbM, and wzm, were downregulated significantly compared to untreated control [67]. These findings suggested that UA has the potential to combat AMR problems with a combination of other phytochemicals, antibiotics, and nanocomposites.
Antifungal: The treatment of fungal infections is now limited to a few antifungal medicines, such as amphotericin B and fluconazole. Furthermore, the introduction of fungal diseases that are resistant to drugs has made patient care even more difficult. Fungal biofilms are a growing clinical concern linked to elevated mortality rates [68, 69]. Various studies proved that the UA might be effective against nosocomial fungal infections. MIC for Cryptococcus neoformans H99 was observed at 0.25 mg/mL of UA. Likewise, the growth curve demonstrated that UA suppressed C. neoformans H99, indicating that UA had outstanding antifungal effects. [70]. Similarly, three aromatic ester derivatives of UA, 3β-(2-iodo) benzoylursolic acid, 3β-(3,4-dimethoxy) benzoylursolic acid, and 3β-nicotinoylursolic acid, showed potent inhibitory activities against C. albicans. [71].
Antiviral: Although viruses play a significant role in nosocomial infections, there is typically not enough data to track trends in incidences because hospital outbreaks are frequently caused by viruses from community-based epidemics and the requirement to start specific laboratory testing. In a study, it is estimated that rotavirus (RV) causes over 129,000 diarrheal fatalities in children globally, of which > 90% occur in countries like Africa and Asia. It is still among the most important infections linked to pediatric diarrheal deaths in the vaccine era [72]. Antiviral reagents can be classified into two classes based on their inhibitory mechanisms: (i) inhibitors that target the viruses directly and (ii) inhibitors that target components within the host cell. Antivirals that target viruses (VTAs) can either directly (DVTAs) or indirectly (InDVTAs) limit the biological activities of viral proteins, primarily enzymatic activities, or prevent the proper assembly of the machinery needed for viral replication [73].
Bacterial membrane interaction with UAUA interaction in cell envelop metabolism disruptionAccording to studies, treating drug-resistant bacteria with a combination of medications can effectively slow down or halt their development. The suppression of metabolic pathways, disruption of the bacterial membrane structure (Fig. 2), disruption of cell wall construction, and interference with bacterial protein and nucleic acid synthesis are the mechanisms by which antibiotics work against infections caused by bacteria [74]. In contrast, S. aureus strains that produce penicillin-binding protein 2a (PBP2a), a protein with a decreased binding affinity to β-lactam antibiotics, develop resistance to these drugs [75]. The treatment of infectious diseases is now significantly hampered by AMR despite numerous efforts over the past few decades to identify the most effective antimicrobials to combat this problem. Therefore, developing novel medications is essential to halting the spread of AMR worldwide. Promising antibiotic alternatives include antimicrobial peptides (AMPs) and cell-penetrating peptides (CPPs), which target membranes. Short amino acid sequences known as AMPs and CPPs have potential therapeutic advantages in addition to their antibacterial action [76].
Fig. 2
Bacterial interaction with UA
In a study, UA isolated from leaves of Acanthopanax henryi was screened to check antibacterial against MRSA alone and with oxacillin. They found a significant MIC value of UA 6.25 μg/ml. They used Western blot to analyze the expression level of PBP2a using UA-treated cells. They found that the PBP2a expression in the combination group decreased by 36.98%. That indicates the UA may be involved in the protein synthesis interruption by damaging RNA [77]. The proteins called porins are found in the outer membrane of bacteria. These proteins can create holes filled with water that regulate the flow of various substances and nutrients across the membrane. They are among the potential targets that antibacterial agents may have. It was discovered that E. coli had porins [78]. Based on their structural differences, porins are classified as monomeric, dimeric, or trimeric [39]. Furthermore, they can be divided into three categories based on their functions in membrane integrity and antibiotic transport: Nonspecific porins (OmpC, OmpF) act on both membrane safety and antibiotic transport, while specific porins for antibiotic transport (LamB, YddB) and porins specific for membrane integrity (OmpA). A rise in bacterial antibiotic resistance is linked to changes in porin structure. For example, OmpF porin is responsible for transporting a variety of antibiotics, such as β-lactams and fluoroquinolones [79]. A. baumannii decreases porin expressions like Caro and Omp 22–33 to withstand carbapenem. Additionally, it alters the integrity of the outer membrane to develop colistin resistance. There are three different mechanisms by which P. aeruginosa resists different antibiotics: intrinsic, acquired, and adaptive. P. aeruginosa fights antibiotics such as β-lactams, quinolones, and aminoglycosides by altering the outer-membrane primary component, the lipopolysaccharides (LPS). This is an example of intrinsic-type resistance [80, 81]. In certain cases, the antibacterial activity of plant extracts might affect critical stages in the pathogenic process. Methicillin-sensitive and methicillin-resistant S. aureus isolates produced less α-hemolysin and staphylococcal enterotoxins A and B after being treated with subinhibitory amounts of thymol or eugenol [82].
Efflux pump (EP) system and UA interaction: phytotherapeutics—the potent efflux pump inhibitors (EPIs)All of these bacteria reported antibiotic resistance mediated by efflux pumps, which are highly conserved components found in all kinds of ce
Comments (0)