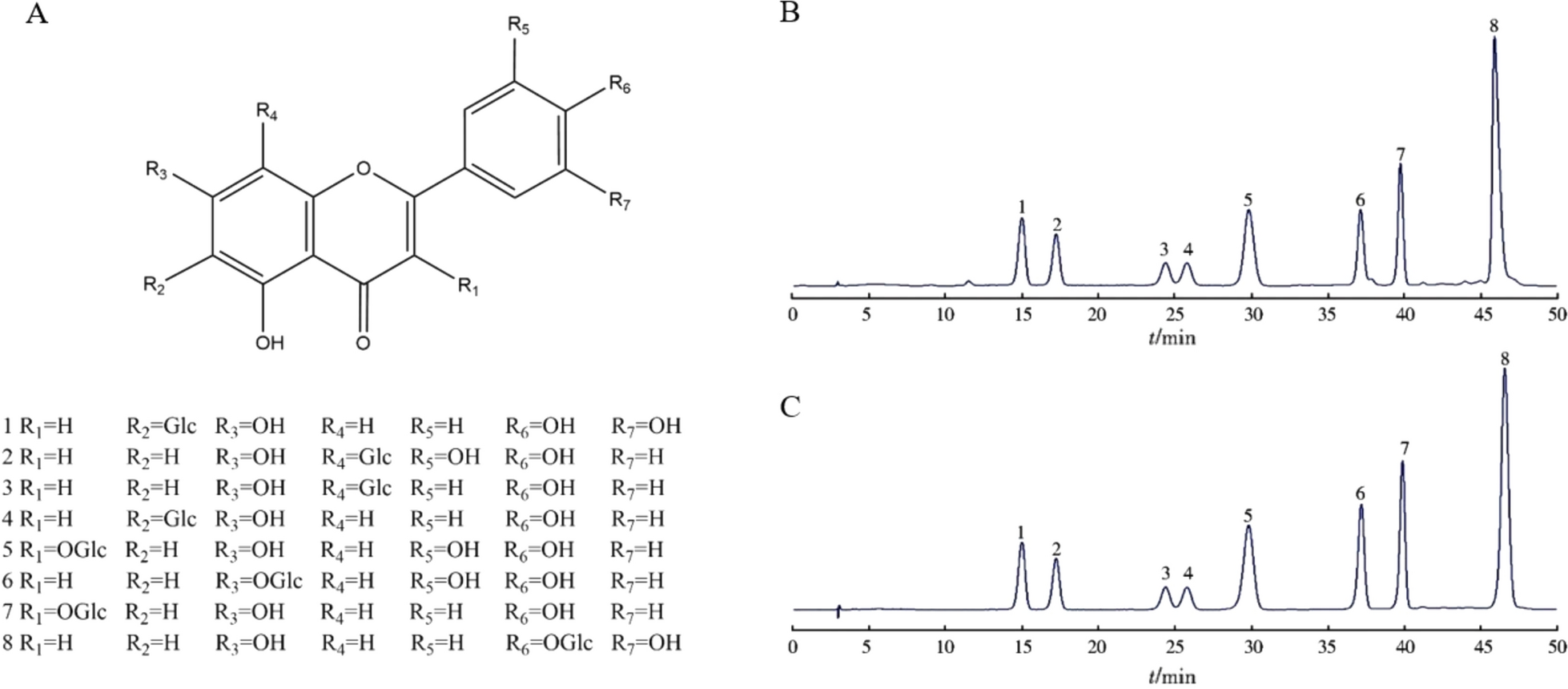
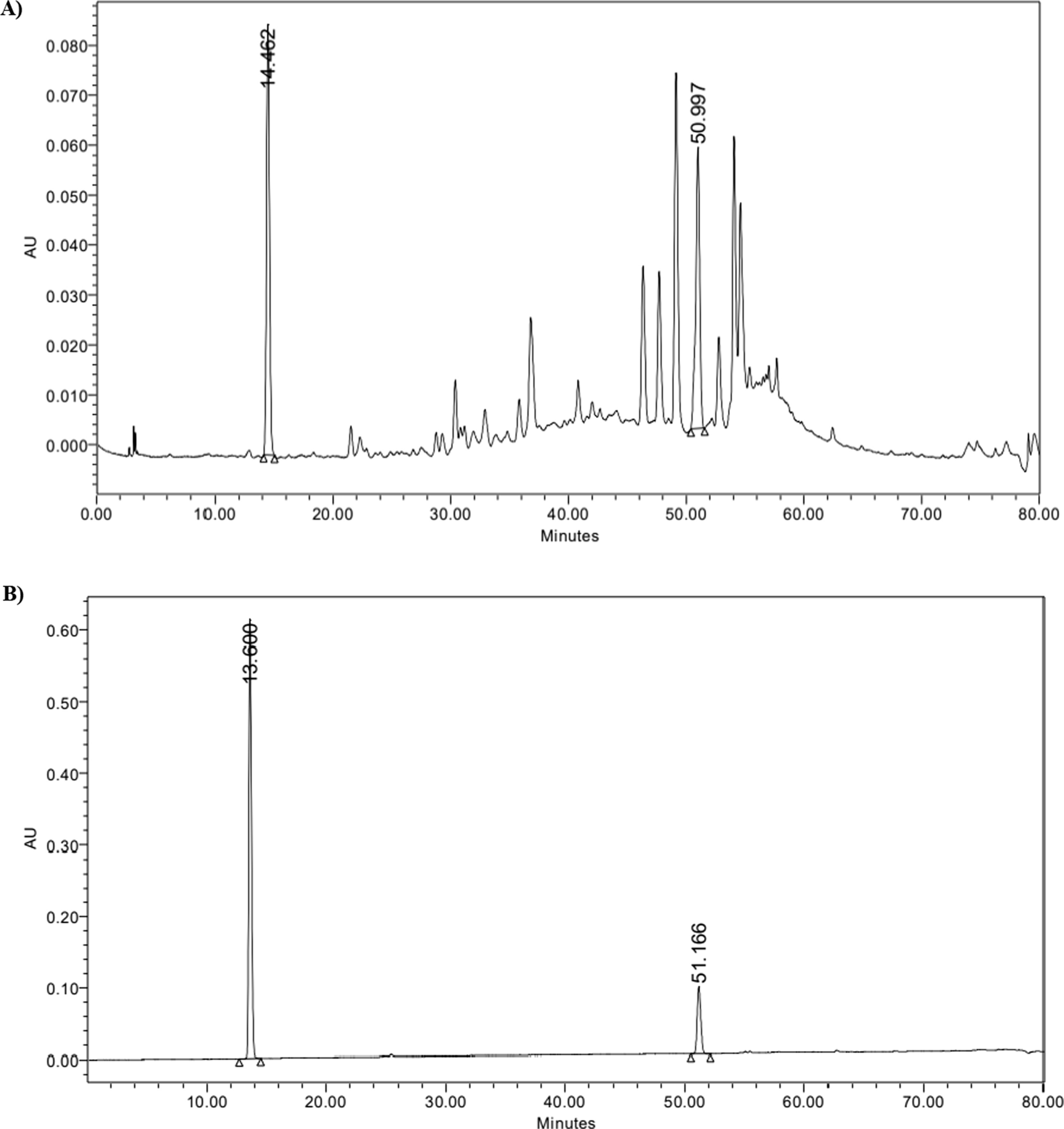
Globally, diabetes has become a serious health concern, with over 90% of cases of DM being type 2 diabetes [30]. About one-third of patients with cirrhosis also have diabetes, and people with type 2 diabetes have a higher risk of developing chronic liver disease, including steatohepatitis and non-alcoholic fatty liver disease [31]. This study assessed the CU’s in vivo antidiabetic and hepatoprotective effect in STZ-induced diabetic mice. STZ is a cell-specific toxin that causes DNA damage and free radical production in pancreatic islets, which results in permanent damage [32]. Prior to the pharmacological study, the extract was chemically characterized. The HPLC chromatogram of the CU showed that gallic acid and rutin are among the major constituents of the extract. They were selected as markers because of their wide availability, cost-effectiveness and efficacy in clinical trials, which are important factors for QC protocols. The biochemical, molecular and histopathological levels evidenced the CU efficacy. Notably, the extract showed a dose-related activity, with 400 mg/kg being the most active dose. The study disclosed the possible underlying molecular mechanisms and assessed the histopathological changes.
The ameliorative CU activity against diabetes and diabetes liver complications.
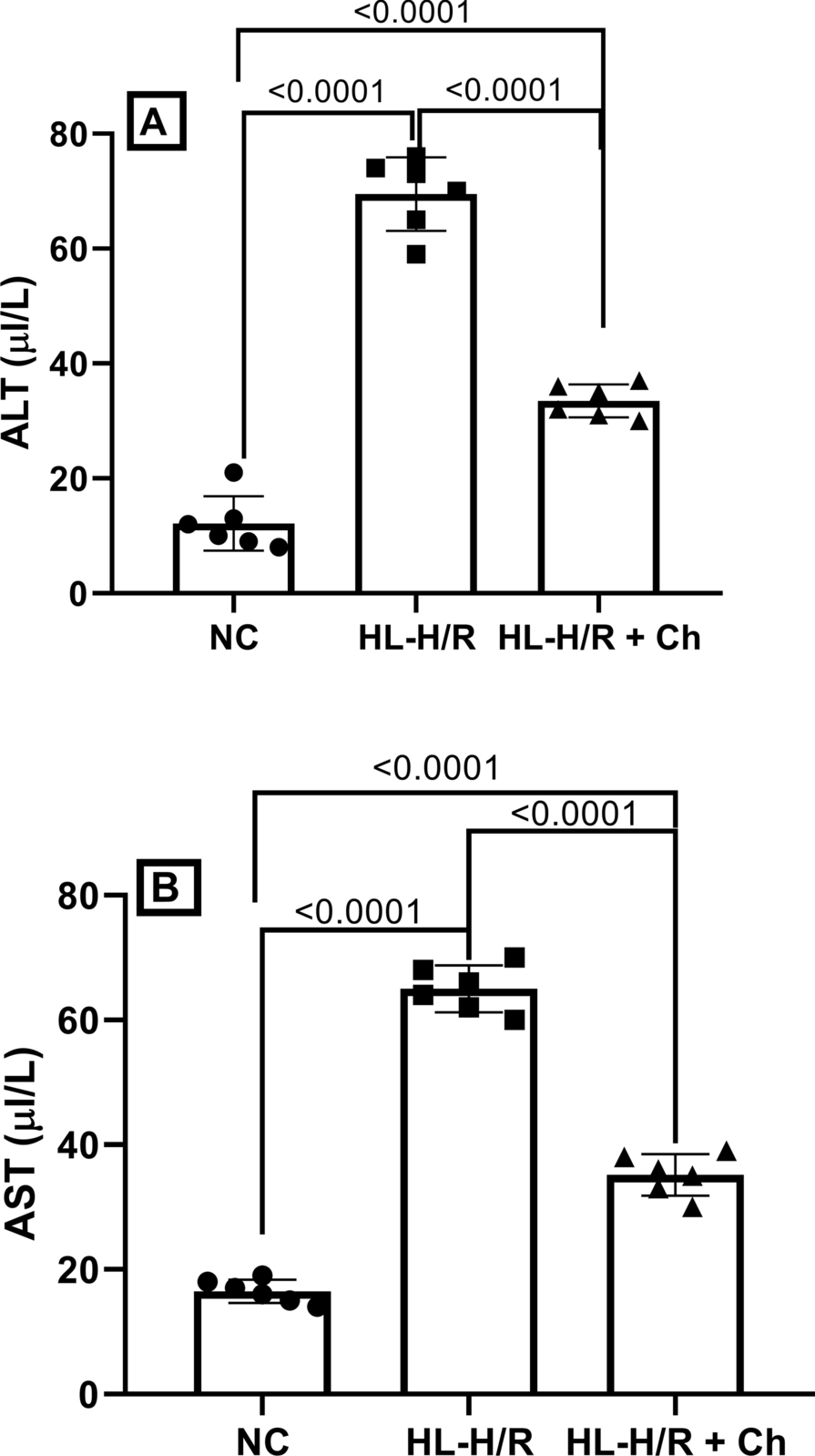
CU had effectively restored serum insulin, resulting in a significant decrease in serum glucose. These effects were reflected in increased body mass. These effects suggest CU-protected Langerhans cells against STZ toxicity, maintaining insulin secretion. CU would be beneficial for type 2 DM patients regarding these aspects. Elevated liver enzymes are correlated with higher odds of diabetes [33]. This could be related to oxidative stress induced by DM [34]. It was reflected in the current study by low GSH and high MDA levels (Fig. 4). CU phenolics had counteracted this oxidative stress leading to restoration of GSH levels and reduction in the oxidative stress marker MDA.
CU normalized the hepatic carbohydrates metabolic enzymes and replenished the glycogen content
The liver is involved in glycogen formation and controls postprandial hyperglycemia. It is well recognized that diabetes mellitus affects the liver's normal ability to synthesize glycogen [35]. Furthermore, partial or complete insufficient amounts of insulin in DM disrupt the metabolism of carbohydrates and lower the activity of the enzymes phosphofructokinase, hexokinase and glucokinase, which depletes muscle and liver glycogen. These enzymes provide an approach for evaluating the peripheral utilization of glucose [36]. CU effectively normalized the hepatic carbohydrate metabolic enzyme hexokinase and restored the glycogen content almost to the normal level. These activities in turn revealed the CU insulin-mimetic activity and its ability to facilitate the glucose uptake by the cells. On the other hand, glucose-6-phosphatase and fructose-1,6-bisphosphatase are crucial enzymes in gluconeogenesis [37]. The activity of these enzymes was reduced significantly by CU. Consequently, CU will result in the inhibition of gluconeogenesis and, hence, lower endogenous glucose synthesis.
CU elevated the expression of insulin receptors and glucose transferase
Insulin receptors (IRs) and insulin receptor substrates (IRSs), two important proteins in the insulin signaling system, are downregulated in the livers of diabetic rodents and humans [38]. The maintenance of glucose metabolism largely depends on IRSs, the major mediators of insulin signaling [39]. Tyrosine phosphorylation of the IRS protein is necessary for the metabolic effects of insulin [40]. This phosphorylation triggers a signaling cascade by activating PI3K and the serine/threonine kinase Akt/PKB. Furthermore, hepatic nutritional homeostasis is particularly dependent on IRS-2, as it mediates the anabolic effects of insulin via the PI3K-AKT cascade [41]. In the current study, CU upregulated IR, IRS-1 and IRS-2 mRNA expression.
The glucose transporter gene GLUT2 regulates the hepatocytes' ability to absorb and release glucose across the plasma membrane. It preserves the balance of glucose inside and outside liver cells. However, the expression of GLUT2 is drastically decreased in DM [42]. CU increased GLUT2 levels in the hepatocyte membrane by increasing mRNA expression.
CU upregulated PI3K and p-AKT signaling in liver tissue
Insulin initiates the PI3K/AKT signaling pathway by binding to insulin receptors on the cell membrane. The main mechanism of insulin signal transduction, which controls glucose uptake, glycogen formation and breakdown, is the PI3K/AKT signaling pathway [43]. Insulin binds to the α subunit of IR on liver cells, activating IRS in the process. Subsequently, IRS binds to PI3K's regulatory subunit, p85, and activates the catalytic subunit, p110. Phosphatidylinositol (3,4)-bisphosphate and phosphatidylinositol (3,4,5)P3, which are produced by activated PI3K, promote the activation of AKT [44].
Activated AKT results in the following: Extracellular glucose is more easily transported into cells when active AKT encourages the translocation of glucose transporter 4 to cell membranes. In addition, it facilitates the synthesis of glycogen and inhibits hepatic gluconeogenesis. Thus, the control of the liver's glucose metabolism is mostly dependent on the insulin-PI3K/AKT signaling pathway. CU effectively ameliorated STZ-induced downregulation of p-PI3K and AKT.
CU retrieved histopathological changes in liver tissues
Previous findings showed that STZ causes histological changes in the liver of diabetic mice. Liver cells of the STZ diabetic animals after 4 weeks from injection displayed severe congestion, necrotic foci, hydropic changes and aggregation of lymphocytes between the hepatocytes, among other more advanced abnormalities. Furthermore, after six weeks of STZ injection, mononuclear inflammatory cell infiltration, severe hydropic degeneration alterations and kupffer cell hyperplasia can be identified [45]. CU retrieved histopathological changes caused by STZ through inhibition of inflammatory cell infiltration and hyperplasia as well as CU limited degeneration of the hepatocytes, showing apparently normal hepatic parenchyma at 400 mg/Kg dose.
Different phenolic acids were quantified from C. uvifera aqueous, ethanolic and acetone leaves extracts such as syringic, ferulic, gallic, o/p-coumaric, ellagic, caffeic acids and others [12]. In the following sections, the antidiabetic activity of these constituents will be discussed. It is reported that high consumption of polyphenols may reduce the risk of diabetes incidence, control the postprandial glycemia and prevent the onset of glucose intolerance. These effects are mediated by facilitating the insulin response and attenuating the release of glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1 [46].
Gallic acid (GA) was quantified in CU with a concentration of 0.09 mg/g extract, and also, it was isolated from C. uvifera leaf extract [47]. A study showed that GA increased glucose uptake by promoting the translocating of GLUT4 to the plasma membrane of rat adipocytes in a dose-dependent manner. Indeed, authors had concluded that the antidiabetic activity of mulberry leaves could be attributed to its gallic acid content [48]. Interestingly, GA alleviated DM detrimental effects in high-fat diet-fed streptozotocin-induced insulin resistance in diabetic rats. GA-treated rats had lower body weight gain, lower fasting blood glucose and lower insulin resistance [49]. Furthermore, the levels of glycogen content and the activity of glucose-6-phosphatase, fructose-1,6-bisphosphatase and hexokinase were dramatically restored to almost normal levels. These beneficial effects were mediated by increased expression of PPARγ (peroxisome proliferator-activated receptorγ) in adipocytes; consequently, GLUT4 was translocated and activated in PI3K- p-AKT dependent pathway [49]. Molecular docking showed that GA had promising interaction against GLUT4, GLUT1, PI3K and p-AKT. Moreover, histological examination revealed consistent distributions of pancreatic islets, adipose and hepatic cells with seemingly normal structures [49, 50]. Moreover, a study evaluated the antidiabetic activity of different hydroxybenzoic acid derivatives. GA suppressed the overexpression of microRNA-1271 generated by free fatty acids and upregulated its targets, such as p-IRS, p-PI3K, p-AKT and p-FOXO1, accompanied with the modulation of glucose metabolism genes [51].
GA was also found to be effective in clinical trials. In single-cell gel electrophoresis assays, oxidized purines are significantly reduced by 31% and pyrimidines by 2% after administration of GA, 15 mg for 7 days for patients of type 2 diabetes [52]. Moreover, following the intervention, the plasma concentrations of C-reactive protein and oxidized LDL were decreased by 39% and 24%, respectively. Consequently, a small quantity of GA (within the daily consumption range in Central Europe) lowers markers reflecting inflammation and elevated risks of CVD and cancer, as well as preventing oxidative DNA damage [52].
Several phenolic acids ameliorated DM manifestations. HbA1c and fasting plasma insulin levels were dramatically reduced by syringic acid, with improvement in liver glucose homeostasis [53, 54] Furthermore, ferulic acid (FA) has been demonstrated to increase the levels of insulin, glycogen and glucokinase, as well as lower the enzymes glucose-6-phosphatase and phosphoenolpyruvate carboxykinase in mice fed on high-fat diet [55]. Furthermore, FA was reported to regulate the gene expression of GLUT2 in the liver of diabetic rats [56]. Moreover, it raised the protein expression levels of IRS-1, PI3K and AKT in the muscles and brains of obese mice treated with FA, which could relieve obesity-related insulin-resistant case [57].
Ellagic acid (EA) enhanced the expression of IRS-1, AKT and ERK in HepG2 cells exposed to high glucose levels; simultaneously, EA downregulated the MDA level, counteracted oxidative stress and increased the glucose consumption by cells [58]. In DM-type 2 rats, EA raised GSH levels while suppressing serum MDA, TNF-α and IL-6. It also decreased liver enzymes ALT, AST and blood glucose [59].
Furthermore, caffeic acid caused upregulation of the expression of IRS-1, AKT, PI3K and GLUT4 [60]. In another study, caffeic acid lowered plasma glucose and glucose-6-phosphatase while increasing body weight and plasma insulin in diabetic rats [61]. Protocatechuic acid found in CU extract [47] has been shown to be able to counteract insulin resistance in obese volunteers by raising the levels of p-Tyr-IRS-1 and p-AKT in the visceral adipose tissue. Furthermore, protocatechuic acid reduced the inflammation and PTP1B activity [62]. In addition to lowering blood glucose levels and gluconeogenic enzymes, p-coumaric acid was reported to modify lipid and glucose metabolism via activating GLUT2.
Flavonoids are ubiquitous phenolic compounds in plants and their beverage products. Numerous in vitro and animal studies support that dietary flavonoids positively impact glucose homeostasis. In addition, through a variety of intracellular signaling mechanisms, flavonoids have been demonstrated to control carbohydrate digestion, insulin secretion, insulin signaling and glucose uptake in insulin-sensitive tissues [63]. Several flavonoids were isolated from C. uvifera leaves extract such as quercetin, myricetin and kaempferol derivatives [47, 64]. Their impact on DM and its complications would be displayed in the following paragraphs.
Rutin was quantified in this study in CU with a concentration of 0.23mg/g extract. A recent review explored the diverse mechanisms of action of rutin against DM. First, rutin reduces glucose level by reducing its absorption from the intestine, increasing the tissue glucose uptake, reducing gluconeogenesis, increasing insulin secretion and protecting islets of Langerhans against deterioration [65]. Moreover, rutin protects against DM complications by reducing sorbitol accumulation, reactive oxygen species, advanced glycation end-products and inflammatory cytokines [66]. Rutin was reported to increase the liver's antioxidant status by raising catalase, glutathione peroxidase and superoxide dismutase levels [67]. It also reduced serum levels of liver enzymes and corrected the histological damage to hepatocytes [68]. Rutin-induced insulin receptor kinase activity and GLUT4 translocation in differentiated myotubes enhance glucose uptake [69]. Furthermore, querectin, isoquercetin and rutin had α-glucosidase inhibiting activity [70].
In STZ diabetic rats treated with rutin (100 mg/kg), there was a decrease in plasma glucose and a rise in insulin levels, as well as a restoration of glycogen content and the activity of carbohydrate metabolic enzymes. The pancreas' histological examination demonstrated rutin's protective function. Meanwhile, the islets became larger, and the fatty infiltration of the islets decreased. [71]. In another study, flavonoids extract from mulberry leaves containing rutin as the main ingredient (1mg/mL) remarkably increased the protein expression levels of p-IRS-1, p-PI3K, p-AKT, total GLUT4 and membrane GLUT4 in 3T3-L1 adipocytes insulin resistance model [72]. Moreover, it has been shown that rutin (23 µg/mL) reversed the high glucose-induced insulin resistance caused in hepatic FL83B cells via enhancing AKT phosphorylation, which thereby enhanced GLUT2 translocation and glucose uptake [73].
Rutin was effective in clinical trials. Consuming 1g of rutin in patients with type 2 diabetes mellitus resulted in a significant decrease in heart rates, mean arterial pressure, pulse pressure and blood pressure. Moreover, there is a substantial rise in the antioxidant enzymes catalase, glutathione peroxidase and superoxide dismutase as well as quality of life (QOL) parameters (emotional limitations, mental health, energy and freshness, social performance and general health) [74].
Rutin was effective when combined with other oral synthetic antidiabetics. When given separately, rutin effectively decreased hyperglycemia in acute assays in a way comparable to oral antidiabetic drugs (OADs). In the subchronic assay, rutin also helped to lower the HbA1c% and hyperlipidemia. In all treatments, rutin and OADs effectively reduced hyperglycemia, as seen by the decline in the percentage of HbA1c and lipid profile. consequently, rutin showed significant activity when combined with antidiabetic medications, which is a first step toward creating novel DM treatments [75].
Rutin and quercetin increased glucose uptake in insulin-resistant FL83B liver hepatocytes. This effect was mediated by the upregulation of p-AKT and GLUT2, reduction in oxidative stress and prevention of the degradation of PPARγ [76]. Quercetin aglycone and its derivatives (quercetin-3-O-glucoside and quercetin-3-O-galactoside) isolated from berry extract, enhanced insulin-independent glucose uptake and stimulated AMPK in muscle cells [77]. Over a period of 28 days, quercetin at dosages of 25 and 50 mg/kg significantly decreased blood glucose and glycosylated hemoglobin (Hb), while increasing the levels of Hb in plasma and hepatic glycogen. After receiving quercetin, the hexokinase and glucose-6-phosphatase activity in diabetic rats were also markedly restored [78].
When isoquercetin (quercetin-3-O-glucoside) was supplemented to STZ-induced diabetic rats, the insulin levels increased significantly, and the glucose levels returned to normal. Additionally, liver enzymes were reduced. Glycogen synthase GK and GLUT2 expressions were markedly upregulated, while glucose-6-phosphatase expressions were significantly downregulated. The levels of gluconeogenesis enzymes were significantly lower than those in negative control. Insulin, IR, IRS-1, IRS-2 and AKT mRNA expressions were also elevated. Indeed, isoquercetin efficacy was similar to that of glibenclamide [79].
Administration of kaempferol (K) and its glycosides rich fraction decreased the area under the curve in glucose tolerance test in genetically type 2 KK-Ay mice. Moreover, the liver had lower triglycerides level and fatty acid synthase activity [80]. By controlling mitochondrial calcium absorption, K stimulates Akt activation and enhances insulin production. Moreover, K directly restores AKT activation. Subsequently, reversing the effects of AKT inactivation causes the upregulation of gluconeogenesis, the downregulation of glycogen synthesis and the uptake of glucose. Additionally, the antioxidant K controls both apoptosis and autophagy [81].
Myricetin caused upregulation of p-IR, p-IRS-1 and p-AKT in the liver of high-fat diet-fed and STZ-induced type 2 diabetic rats. These effects were mediated by suppressing PTP1B's activity and expression; PTP1B is the tyrosine phosphatase that adversely regulates insulin signal transduction. These effects were evident when myricetin was administered alone and not in combination with horsegram protein [82]. Moreover, hexokinase, glycogen synthase, glycogen phosphorylase, glycosylated hemoglobin, glucose-6-phosphatase and plasma glucose were all inhibited from a significant increase [83]. It has been determined that myricitrin, glycosylated myricetin, activates the IRS-1/PI3K/AKT/GLUT4 pathway in the soleus muscle of type 2 DM-affected rats as well as in L6 muscle cells exposed to high glucose [84].




Comments (0)