
Remember me



A 71-year-old woman with Human Papilloma Virus (HPV)-related anal squamous cell carcinoma received atezolizumab. Two months after anti-PD-L1 initiation, she developed a grade (G) 2 ankle arthritis, followed by G3 hyponatremia 7 months after the onset of treatment, both diagnosed as irAEs. In addition, dizziness and postural instability appeared during active atezolizumab treatment, 14 months after its initiation. Symptoms progressed in the subsequent 2 months, as she developed dysarthria, gait ataxia, retropulsion, and upper limbs dysmetria. Lumbar puncture (LP) revealed normal protein content and cellularity, but CSF-restricted OCBs were detected. Neuronal Abs were negative. Contrast-enhanced brain MRI did not reveal any cerebellar abnormality. Lower limbs nerve conduction studies were unremarkable. High-dose corticosteroids (CS) were administered (8-day-course of IV methylprednisolone 500 mg/die, followed by oral taper), and a significant improvement of gait and limb ataxia was noticed. However, during CS oral taper (50 mg/die) she experienced neurological worsening, including limb ataxia, dysarthria, and dysphagia. From an oncological standpoint, the patient was disease-free at latest follow up, over three years after ICI withdrawal. However, her neurological status kept worsening: at a 4-year follow-up, she was wheelchair-bound and had developed frank truncal ataxia (Video 1); both upper and lower limb ataxia appeared; dysarthria became severe and ocular dysmetria added up to the clinical picture.
Patient 2A 60-year-old man with lung adenocarcinoma received pembrolizumab, with concomitant platinum and pemetrexed chemotherapy. Five weeks after ICI initiation, pancerebellar symptoms appeared subacutely, including dysarthria/scanning speech, oculomotor disturbances, gait, trunk, and limb ataxia. LP revealed mildly increased protein content (53 mg/dL) and pleocytosis (19 cells/mm3). Anti-Yo Abs were detected. Brain MRI was unremarkable. Pembrolizumab was withdrawn and the patient was treated with CS and intravenous immunoglobulins (IVIg), with no improvement. Oncological disease progression was observed, and the patient eventually died (follow-up time: 4 months).
Patient 3A 52-year-old woman with ovarian clear cell carcinoma was treated with pembrolizumab; concomitant bevacizumab and doxorubicin therapy was administered. Three weeks after ICI initiation, she developed dysarthria and trunk, gait and limb ataxia. LP revealed increased protein content (59 mg/dL) and pleocytosis (64 cells/mm3). Anti-Yo positivity was identified, while MRI was normal. Pembrolizumab was withdrawn, while CS, IVIg and rituximab (RTX) were administered, with no effect on her neurological status. The underlying cancer progressed, and she eventually died (follow-up time: 17 months).
Patient 4A 66-year-old woman was treated with a combination of nivolumab and relatlimab for a retroperitoneal leiomyosarcoma. Eight weeks after starting ICI therapy, she developed gait and limb ataxia. LP revealed increased protein content (368 mg/dL), pleocytosis (261 cells/mm3), and type II OCBs. Neuronal Ab and microbiological testing as well as brain MRI were negative. ICI combination therapy was withdrawn, and CS and IVIg were administered, leading to symptoms improvement despite residual disability. Oncological disease recurred (follow-up time: 8 months).
Patient 5A 53-year-old woman with a history of small cell lung cancer (SCLC) was treated with atezolizumab and concomitant platinum-etoposide. Eleven weeks from the initiation of atezolizumab, she developed dizziness, dysarthria, oculomotor cerebellar deficits and limb ataxia. In addition, she became confused and dysphagic. CSF testing revealed normal proteins, pleocytosis (21 cells/mm3), and OCBs positivity. Anti-TRIM9 positivity was detected. MRI showed bilateral III and right VII-VIII cranial nerve contrast enhancement, while no cerebellar abnormality was detected. Despite ICI interruption and treatment with CS, IVIg and tofacitinib (Janus Kinase (JAK) inhibitor), no improvement of cerebellar symptoms was noticed. However, no tumor progression was detected either at oncological follow-up (follow-up time: 5 months).
Patient 6A 79-year-old man with melanoma was treated with 4 cycles of a combination ICIs (nivolumab and ipilimulab), followed by nivolumab alone. During active ICI treatment (eighty-two weeks after ICIs were initiated), gait and limb ataxia were noticed. In addition to ICI-mediated cerebellar toxicity, other irAEs developed, including vitiligo and thyroiditis. LP revealed increased CSF proteins (100 mg/dL), but neither pleocytosis nor OCBs presence. No neuronal Abs positivity was detected, and brain MRI was negative. ICI interruption and CS treatment led to symptoms improvement with residual disability (follow-up: 15 months). Oncological outcome was not available.
Patient 7A 75-year-old man with a history of SCLC was treated with atezolizumab and platinum-etoposide concomitantly with the first 4 cycles of ICI. During active atezolizumab treatment (44 weeks after its initiation), a pancerebellar syndrome developed, including dysarthria, oculomotor cerebellar abnormalities, as well as gait, truncal and limb ataxia. CSF proteins and cell count were normal, while CSF-specific OCBs were detected. Atypical Ab staining was initially observed, and anti-DACH1 positivity was later identified; MRI showed cerebellar atrophy and cerebellar hyperintensities. ICI was withdrawn, and CS and IVIg were started, without any significant improvement (immunotherapy led to mild dysarthria amelioration, but the benefit was transient). From an oncological point of view, tumor progression was noticed (follow-up time: 14 months).
Patient 8A 68-year-old man with stage IV lung adenocarcinoma received nivolumab, after several other anticancer treatment attempts (stereotactic radiotherapy, cisplatin, 5-fluoro-uracyl, and cetuximab). During active nivolumab treatment (25 weeks after its initiation), gait and trunk ataxia, and oculomotor cerebellar deficits developed. LP revealed normal CSF proteins and cell count, and OCBs negativity. Ab screening was negative, while MRI revealed cerebellar hyperintensities involving dentate nuclei bilaterally. Nivolumab was withdrawn, and CS were administered; from a neurological standpoint, he improved with residual disability, and no cancer progression was demonstrated but the patient was lost to follow-up.
Patients 9–12Four cases of cerebellar irAEs were seen during the study period and previously described by our group in a paper focused on CNS adverse events of ICI [7]. These cases were not described at the individual patient level in the initial publication, but rather as a whole. We therefore retrieved clinical and paraclinical data of the individual patients, obtaining a total of 12 original cases.
Clinical Features of Cerebellar irAEs in a Cohort of 35 CasesOverall, 19 articles with 23 individual patients were included in the systematic review, to which our 12 original cases of cerebellar irAEs were added. Relevant characteristics of patients with ICI-mediated cerebellar toxicity are shown in Table 1.
Table 1 Characteristics of patients with cerebellar irAEsAmong a total of 35 cases of cerebellar toxicity following ICI therapy identified, 25/35 (71%) were males, while 10/35 (29%) females. The median age (available in 34/35 cases) was 65 years (age range: 20–82). The most frequent tumor was non-small cell lung cancer (NSCLC), which was present in 12/35 (34%) patients, followed by SCLC (9/35, 26%), melanoma (3/35, 9%), Hodgkin lymphoma (2/35, 6%), head and neck squamous cell carcinoma (HNSCC; 2/35, 6%), Merkel cell carcinoma (MCC; 2/35, 6%), bladder carcinoma (1/35, 3%), renal cell carcinoma (RCC; 1/35, 3%), HPV-related anal squamous cell carcinoma (1/35, 3%), ovarian clear cell carcinoma (1/35, 3%), and retroperitoneal leiomyosarcoma (1/35, 3%).
All patients were treated with single or combination ICI; in particular, anti-PD1 were adopted in 19/35 (54%) (nivolumab n = 9, pembrolizumab n = 9, toripalimab n = 1), anti-PDL1 in 9/35 (26%) (atezolizumab n = 8, avelumab n = 1), CTLA4-inhibitor in 1/35 (3%) (ipilimumab n = 1). Combination therapy was administered to 6/35 (17%) patients and consisted in either anti-PD1 and CTLA4-inhibitor (nivolumab and ipilimumab n = 4), anti-PDL1 and CTLA4-inhibitor (durvalumab and ipilimumab n = 1), or anti-PD1 and anti-LAG3 (nivolumab and relatlimab n = 1). Nineteen patients also received chemotherapy and/or radiotherapy. Cerebellar toxicity developed a median of 11 weeks after the onset of ICI therapy (range: 0.1–82; data available for 33 patients). In 11/33 (33%) patients, toxicity arose after 6 months of ICI initiation.
Full-blown neurological symptoms consisted in “isolated cerebellar ataxia” (gait and/or limb and/or trunk ataxia) in 13/35 (37%), ataxia and dysarthria in 6/35 (17%), ataxia and ocular involvement in 4/35 (11%) and a “pancerebellar syndrome” (ataxia, dysarthria, and ocular involvement) in 9/35 (26%). Symptoms could not be further characterized in 3/35 (9%) patients.
Four patients developed other irAE, namely inflammatory arthritis, diabetic ketoacidosis due to type I diabetes and possible pancreatitis, hyponatremia and arthritis, as well as vitiligo and thyroiditis. Ab testing was not available in 4 patients; positivity was detected in 15/31 (48%) cases. Abs included those binding to unclassified antigens (n = 2), anti-Hu (n = 2), anti-Yo (n = 2), anti-Yo and anti-VGCC (n = 1), anti-PCA-2 (n = 1), anti-Zic4 (n = 1), anti-GAD65 (n = 1), anti-GFAP (n = 1), anti-TRIM9 (n = 1), neurofilament-light chain, neurofilament-heavy chain and alpha-internexin (n = 1), amphiphysin and P/Q VGCC (S) (n = 1), and anti-DACH1 (n = 1).
Lumbar puncture was not available in five patients. CSF findings included raised protein content (21/30, 70%) and pleocytosis (15/30, 50%). OCBs were tested in 14/30 (47%) patients and were present in all but 3 of them. Overall, CSF was inflammatory in 25/30 (83%). Search for malignant cells was negative in all cases.
Brain MRI was available for all patients; 8/35 (23%) showed cerebellar hyperintensities, 4/35 (11%) cerebellar atrophy, and 2/35 (6%) cerebellar edema. Additional findings included early tonsillar herniation and hydrocephalus (n = 1), brain small vessel disease (n = 1), multiple spot-shaped periventricular, leptomeningeal and parenchymal contrast enhancements (n = 1), leptomeningeal enhancement (n = 1), bilateral III and right VII and VIII cranial nerve enhancement (n = 1), cortical ribbon interruption (pre-existent) and supratentorial metastases (n = 1), T2/FLAIR hyperintensity of the left oculomotor nerve with contrast enhancement (n = 1).
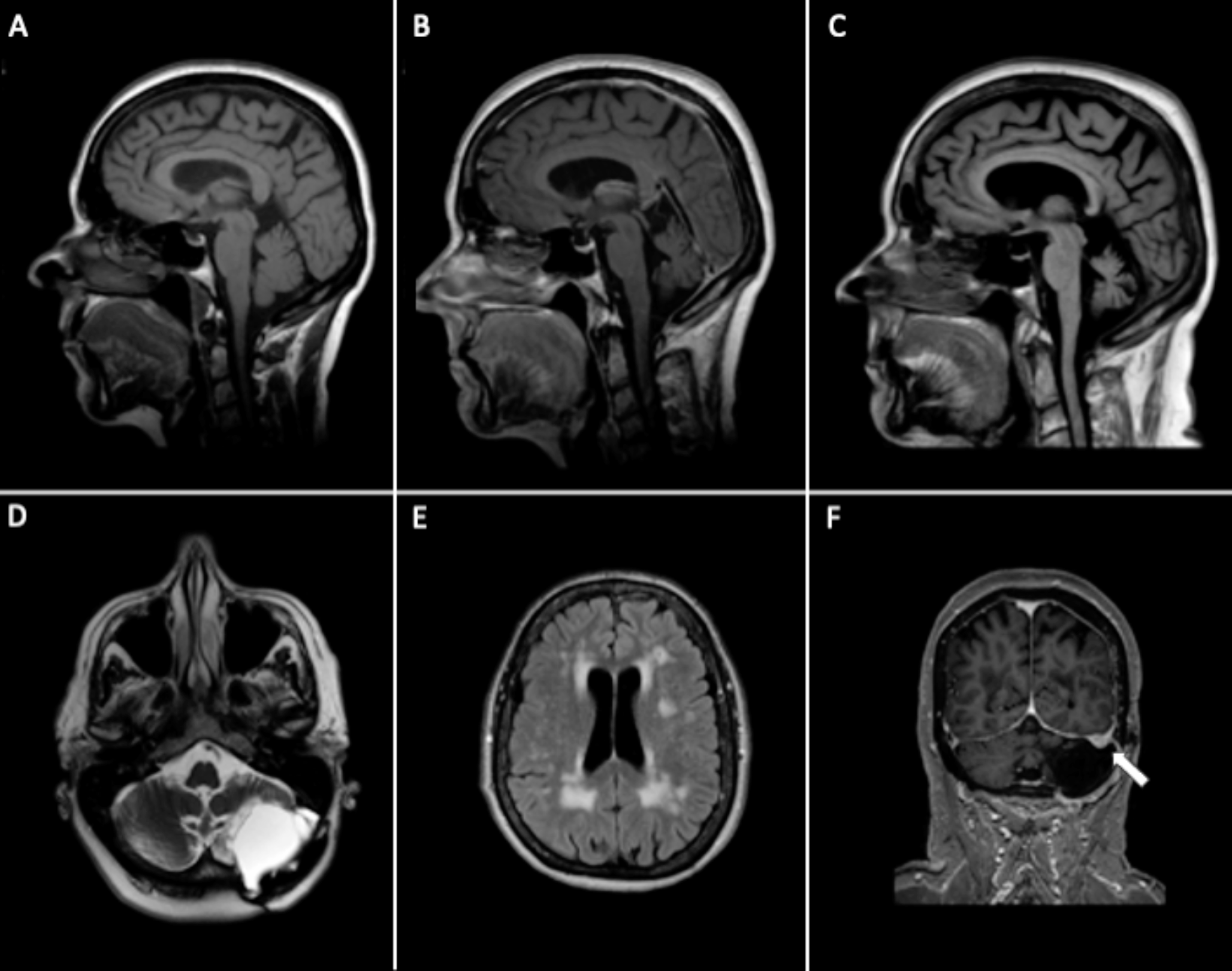
Brain MRI findings of patients with cerebellar irAEs are shown in Fig. 2 and compared to those of patients with PCA, while results of indirect immunofluorescence are shown in Fig. 3.
Fig. 2
Representative brain MRI findings. Fluid attenuated inversion recovery (FLAIR) brain magnetic resonance imaging (MRI) findings in patients with cerebellar immune-related adverse events (irAEs) due to immune checkpoint inhibitors cancer treatment (A, sagittal section; B and C, axial sections) showing cerebellar hyperintensities. Brain MRI findings in paraneoplastic cerebella ataxia demonstrating mild cerebellar hypersignal (D and E, axial sections) as well as atrophy (F, sagittal section)
Fig. 3
Immunological studies. Indirect fluorescent immunostaining on rat brain sections performed using Patient #5 cerebrospinal fluid (CSF) (A, B and C) or CSF from a patient with classical anti-Yo paraneoplastic cerebellar ataxia (PCA) (D, E and F). Patient #5 CSF showed the typical staining pattern of TRIM9-Abs: strong staining of CA3 pyramidal cells in the hippocampus (B), strong reactivity at the level of the molecular layer, the cell bodies, and proximal dendrites of Purkinje cell in the cerebellum (C). Classical Yo-Abs produce a strong staining of the cytoplasm of Purkinje cells. Basket and stellate cells in the molecular layer are also labeled (F). Ca1, ca3: CA1 and CA3 pyramidal cell layer of the hippocampus; dg: dentate gyrus; gl: granular layer, pkj: purkinje cell layer, ml: molecular layer of the cerebellum
ICI was withdrawn in all patients. Immune-modulating therapy was applied in 33/35 patients (94%). It consisted in CS monotherapy in 18/35 (51%), CS and IVIg in 7/35 (20%), CS and infliximab in 1/35 (3%), a combination of three among CS, IVIg, Plasma Exchange (PE) and RTX in 4/35 (11%), CS, IVIg and tofacitinib in 1/35 (3%), and CS, IVIg, PE and RTX in 1/35 (3%). Two patients received no immune-modulating therapy (2/35, 6%).
Concerning neurological outcome, 16/35 (46%) patients improved with residual disability, 9/35 (26%) returned to pre-ICI condition, 7/35 (20%) did not improve and 3/35 (9%) worsened. By applying the PNS-Care Score [14] to patients with cerebellar irAEs, “PNS-like” syndromes were identified. Three patients belonged to the “definite” score category (3/35, 9%), nineteen to the “probable” (19/35, 54%), and thirteen to either the “possible” or “non-PNS” (13/35, 37%). When comparing patients with “definite” PNS-like syndromes to the remainders, a statistically significant worse neurological outcome was identified (p < 0.05) (Supplementary Table 1).
Tumor regression or no progression was observed in 14/35 (40%), while 10/35 (29%) relapsed; oncological outcome was not specified in 11/35 (31%). At last available follow-up, 8/35 (23%) patients had died due to either tumor progression (n = 5) or pneumonia (n = 2); in one case (n = 1) cause of death was undetermined.
Paraneoplastic Cerebellar AtaxiasWe identified 15 cases of PCA at the Udine University Hospital during 7 years (2017–2023). Relevant characteristics of patients with PCAs are shown in Table 2.
Table 2 Characteristics of patients with paraneoplastic cerebellar ataxiaAmong PCA patients, 10/15 (67%) were females, while 5/15 (33%) were males. The median age at neurological disease onset was 70 years (age range: 33–77). The most frequent associated tumor was ovarian cancer (n = 3), followed by breast cancer (n = 2), gastric cancer (n = 2), NSCLC (n = 1), Merkel-cell carcinoma (n = 1), prostate cancer (n = 1), esophageal cancer (n = 1), leukemia (n = 1) and concomitant prostate and SCLC (n = 1). In 2 cases tumor status was unknown. One patient only had a previous cancer (lung adenocarcinoma, diagnosed 8 months prior to gastric cancer). Seven patients were metastatic at tumor diagnosis (7/15, 47%), while in 4/15 (27%) the tumor was localized; data were not available in 4/15 (27%).
Full-blown neurological symptoms consisted in ataxia and dysarthria in 6/15 (40%), ataxia and ocular involvement in 5/15 (33%), a “pancerebellar syndrome” (ataxia, dysarthria, and ocular involvement) in 3/15 (20%), and “isolated cerebellar ataxia” (gait and/or limb and/or trunk ataxia) in 1/15 (7%).
These symptoms developed a median of 39 weeks from histological tumor diagnosis (range: 0-522); symptoms were antecedent to tumor diagnosis in 7/15 (47%) cases, while in 8/15 (53%) they were detected simultaneously or after oncological diagnosis. Ab positivity was detected in 9/15 (60%) cases, namely anti-Yo (n = 6), anti-Ma2 (n = 1), anti-Hu (n = 1), and anti-neurofilament medium chain (n = 1). Lumbar puncture was performed in 7/15 cases (47%). Findings included raised CSF proteins (2/7, 29%) and pleocytosis (1/7, 14%). MRI was not available in 2/15 (13%) patients; 3/15 (20%) showed cerebellar atrophy, and 1/15 (7%) cerebellar hyperintensities; in 9/15 (60%) cases no cerebellar abnormality was detected. Additional findings included gliosis and/or meningioma (not related to the clinical picture) and/or hyperintense lesions in 7/15 cases (47%).
Immune-modulating therapy was applied in 10/15 patients (67%). It consisted in CS in single therapy in 4/15 (27%), CS and IVIg in 4/15 (27%), CS, IVIg and PE in 1/15 (7%), a combination of CS, IVIg, PE and cyclophosphamide in 1/15 (7%); no treatment was applied in 5/15 (33%). Concerning neurological outcome, 1/15 (7%) patients returned to baseline condition, 4/15 (27%) improved with residual disability, 7/15 (47%) did not improve and 1/15 (7%) worsened. Outcome was not available in 2/15 (13%) cases. When calculating the PNS-Care Score [14], 5/15 (33%) had a definite PNS, 5/15 (33%) a probable PNS, and 5/15 (33%) a possible PNS.
Oncological follow up was not available in 4/15 (27%) cases. Tumor regression or no progression was observed in 8/11 (73%), while 2/11 (18%) relapsed; in 1/11 (9%) a tumor was not found.
Comparison between Cerebellar irAEs and Paraneoplastic Cerebellar AtaxiasA comparison between cerebellar irAEs and paraneoplastic cerebellar ataxias is presented in Table 3. Female patients were significantly more represented in the PCA group (p = 0.01). Ab positivity did not differ between the two group, while high-risk Abs were significantly more represented among PCA patients (p < 0.05), and so were anti-Yo Abs specifically (p < 0.05). Gynecological and breast cancers were significantly more frequent in the PCA group (p < 0.01), while lung cancer in the cerebellar irAE group (p < 0.01). As far as concerns the clinical presentation, “isolated cerebellar ataxia” was more common in the cerebellar irAE group (p < 0.05), while ataxia associated with either dysarthria or ocular symptoms was more frequent in the paraneoplastic group (p < 0.01). In addition, patients who developed cerebellar toxicity following ICI showed a significantly better neurological outcome (p < 0.05) (a good neurological outcome being defined as neurological improvement or return to baseline condition). Immune-modulating therapy was more frequently applied in the cerebellar irAEs group as compared to the PCA group (p < 0.05).
Table 3 Comparison between cerebellar irAE and PCAFig. 4
Diagnostic algorithm specific to cerebellar irAEs
Comments (0)