
Remember me

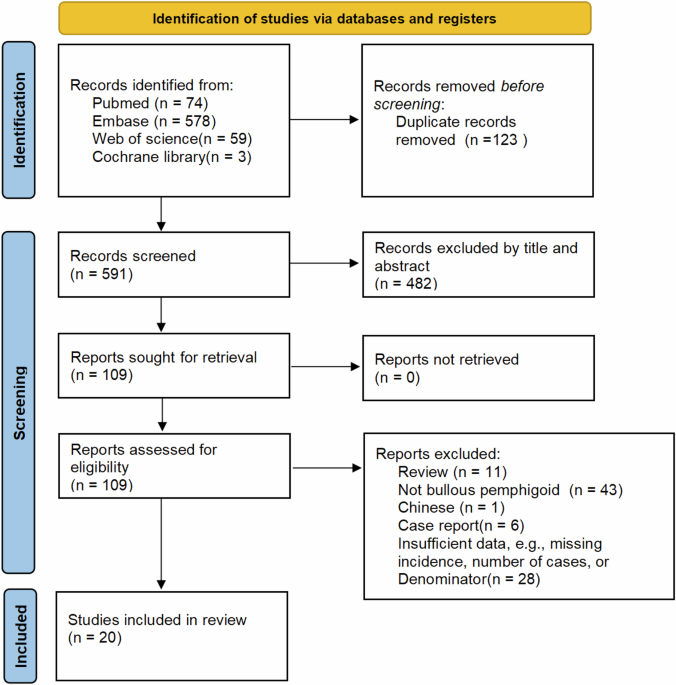
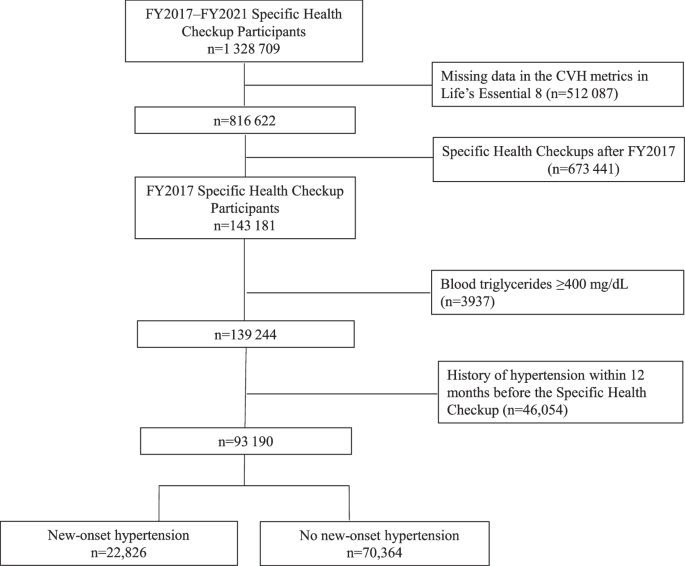
Figure 1 details the PRISMA flowchart. The search generated 1782 articles, with 244 potentially eligible articles identified during the title and abstract screening. The full text screen identified 20 articles that met the inclusion criteria for the review. Of these articles, 18 were from peer-reviewed journals and two were PhD theses. The main reasons for exclusion were study design not meeting the inclusion criteria (31%), articles not in English (18%), or outcomes outside of the inclusion criteria (14%).
Fig. 1: PRISMA flowchart.
Flowchart in line with PRISMA guidelines indicating the number of articles originally identified, screened, excluded and included within the systematic review.
Participant characteristicsThe overall characteristics of the 20 included studies are summarised in Table 1. The mean demographics are reported in Table 2. The studies were published between 1975 and 2013, from 10 different countries. There was a total of 988 participants and sample sizes ranged from 15 to 301 participants. The age ranged from 28 to 70 years, with 45% female participants. Ethnicity was reported in 3 articles, of these, 96% were Caucasian. The mean baseline SBP was 149.3 ± 7.8 mmHg and the mean DBP 93.0 ± 6.9 mmHg. Five studies [18,19,20,21,22] did not report data such as sex or age and were omitted from the above summary but were included in the main analysis as they reported key outcomes.
Table 1 Study characteristics and effect of biofeedback on blood pressure.Table 2 Mean baseline measurements and demographics.Types of biofeedback modalitiesThere were six different biofeedback modalities used across the 20 studies (Table 3). The type of biofeedback device used varied across studies and modalities, including finger or forehead electrodes [22,23,24,25], sphygmomanometer [18, 26, 27], finger blood pressure machines [28, 29] and compact disk (CD) players [30, 31]. No studies used a wearable device.
Table 3 Summary of biofeedback intervention components and design used in the included studies.Blood pressure biofeedback was used by six studies and was measured with either a non-invasive beat to beat finger arterial pressure measurement [29] or an automated blood pressure device [18, 20, 26, 27, 32]. Blood pressure biofeedback was typically received by the participant visually (e.g., a screen) [18, 26, 28, 29, 32] and/or auditorily (e.g., a beep) [22, 23]. For example, participants in the study by Tsai et al. [29] performed self-regulation techniques, such as deep breathing, and observed their blood pressure on a display.
Electromyographic (EMG) biofeedback detects changes or contractions in muscle. All six studies using EMG biofeedback gave auditory feedback, with some using the tone pitch and frequency to indicate EMG changes [19, 20, 22, 24, 33].
Galvanic skin response (GSR) biofeedback focuses on sweat gland activity and was used by five studies. As an example: Patel et al. [25] delivered the GSR feedback tone in one headphone and played a relaxation tape through the other headphone. The tone grew fainter as the participant relaxed and GSR activity reduced.
Thermal biofeedback was used in four studies. The intervention by Blanchard et al. [34] aimed to teach participants to increase temperature of their hands or feet, therefore strengthening deep-muscle relaxation.
RESPeRATE, a branded auditory based biofeedback device, was used in two studies [30, 31]. It involves listening and breathing in time with a melody to guide slow breathing [30].
Achmon et al. [35] was the only study to use heart rate biofeedback. It used ear lobe capillary pulsations to guide heart rate reductions in normal and tension-provoking situations.
Intervention characteristicsTable 3 details the biofeedback intervention characteristics of the included studies. Biofeedback was mostly delivered one-to-one, with four studies delivering biofeedback to groups of 3–13 participants [19, 28, 33, 34]. Studies varied in the biofeedback session length (12–75 min) and number of sessions (4–48 sessions). The post-study follow up ranged from 2 weeks to 12 months, with ten studies not reporting any follow up. Biofeedback training was delivered by psychologists in four studies [27, 34, 36, 37] and by a trained nurse or therapist in two studies [32, 35]. Three studies used an experimenter or research assistant to deliver biofeedback [18, 20, 24], with the remaining eleven not detailing who delivered biofeedback training.
There were eight different control conditions used across studies, the most common were self-recorded blood pressure measurements and placebo. Six studies [22, 24, 26, 34, 35, 38] had multiple comparison groups (i.e., biofeedback and treatment as usual, placebo biofeedback, normotensive comparators). For data extraction, the treatment as usual group was prioritised as a comparator, followed by placebo biofeedback.
There was large variation across intervention design making it difficult to compare different designs and understand the most effective biofeedback intervention.
In terms of measuring how intervention delivery corresponded to the protocol, only two studies [29, 34] detailed methods that suggested fidelity checks, including a therapist remaining with the group throughout the intervention and a trained nurse implementing biofeedback under supervision of a qualified biofeedback practitioner. Only five studies [18, 25, 28, 31, 36] reported the use of power calculations to inform the sample size.
The methods used for blood pressure measurements varied across studies; seventeen [18,19,20, 22,23,24,25, 27,28,29,30,31, 33, 35,36,37,38] used clinic readings, and three [26, 32, 34] used home measurements. In the ten studies [19, 20, 23, 24, 27, 30,31,32, 35, 36] reporting medication use, 55% of participants were on anti-hypertensive medications. Medication status was not reported in three studies [25, 33, 37], whilst seven [18, 22, 26, 28, 29, 34, 38] studies reported participants were not taking any medications.
A total of seventeen studies detailed information regarding participant withdrawal or exclusion, with the remaining three studies [22, 26, 38] not reporting if any participants withdrew from the study. Overall, 111 participants withdrew, 44 were excluded and 2 participants died during the study time period. Reasons or details of participant withdrawal was limited, with 4 studies [19, 27, 33, 36] detailing if participants withdrew from the control or biofeedback group, and six studies detailing the specific stage participants withdrew at i.e., before or after baseline measurements [27, 37], after randomisation [30, 33, 35] or “within 2 weeks” [32]. Nine studies [18,19,20, 23, 24, 28, 29, 34, 36] did not detail at what stage participants withdrew. Reasons for participant exclusion included overly high blood pressure [
Comments (0)