Primary Fallopian Tube Cancer: A Rare Interesting Case Report
Introduction
Primary fallopian tube carcinoma is a very rare gynaecologic malignant tumour and accounts for approximately 0.14–1.8% of female genital malignancies (Rexhepi et al. in Open Access Maced J Med Sci 5:344–348, 2017). Histologic, molecular and genetic evidence shows that 60–70% of tumours that were classified as high-grade serous carcinomas of the ovary or peritoneum might have originated in the distal fimbrial end of the fallopian tube.
Case Details
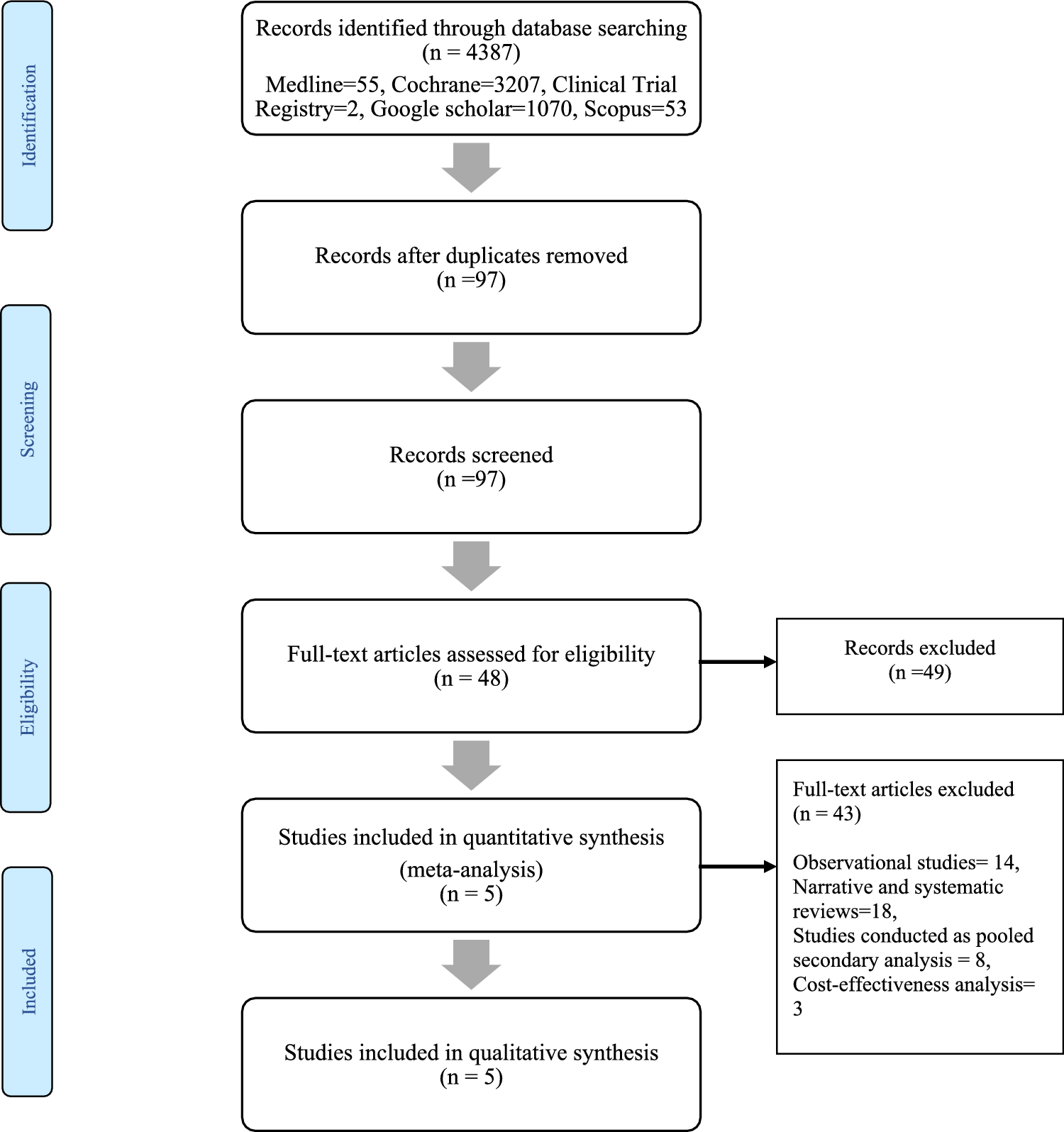
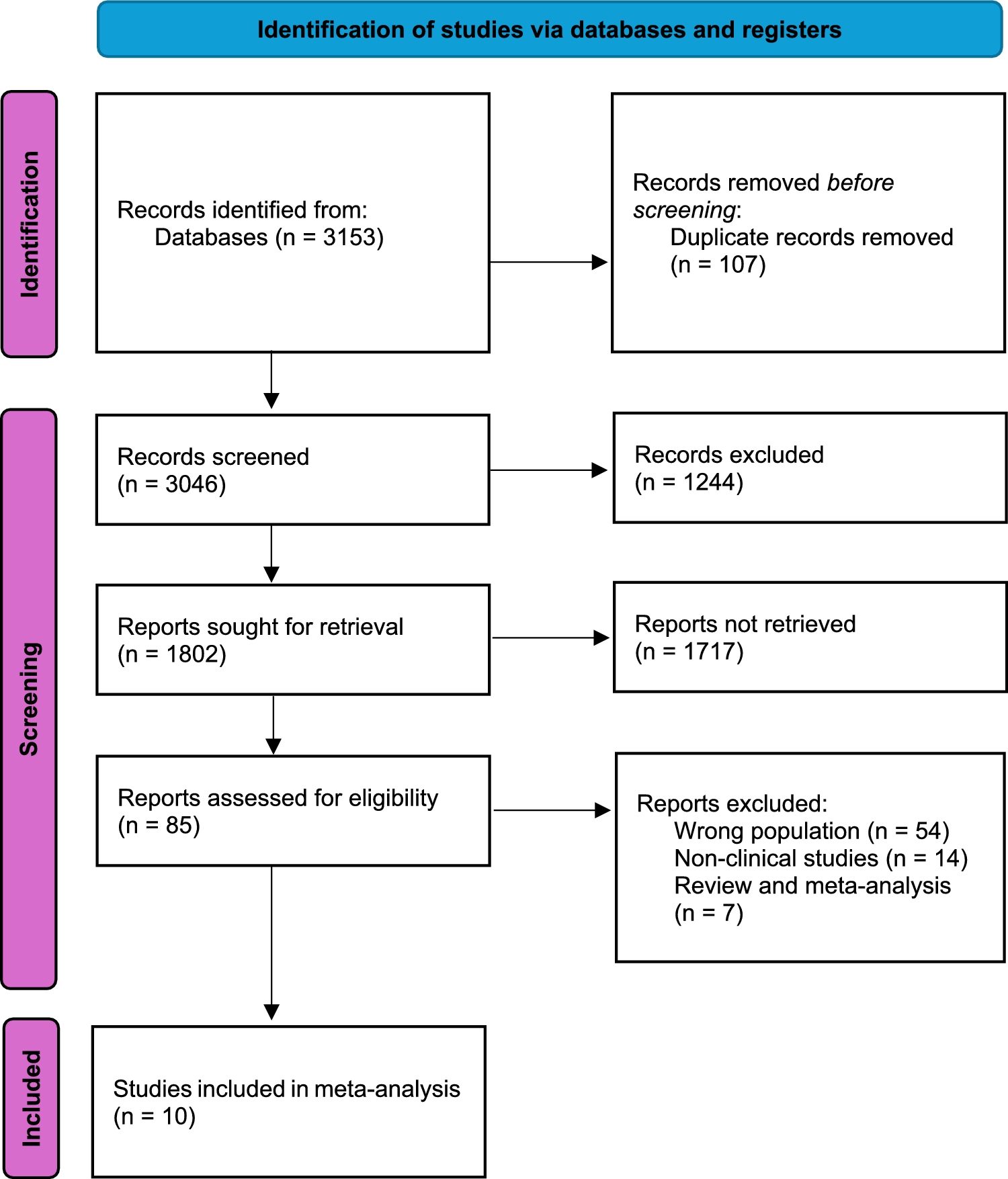
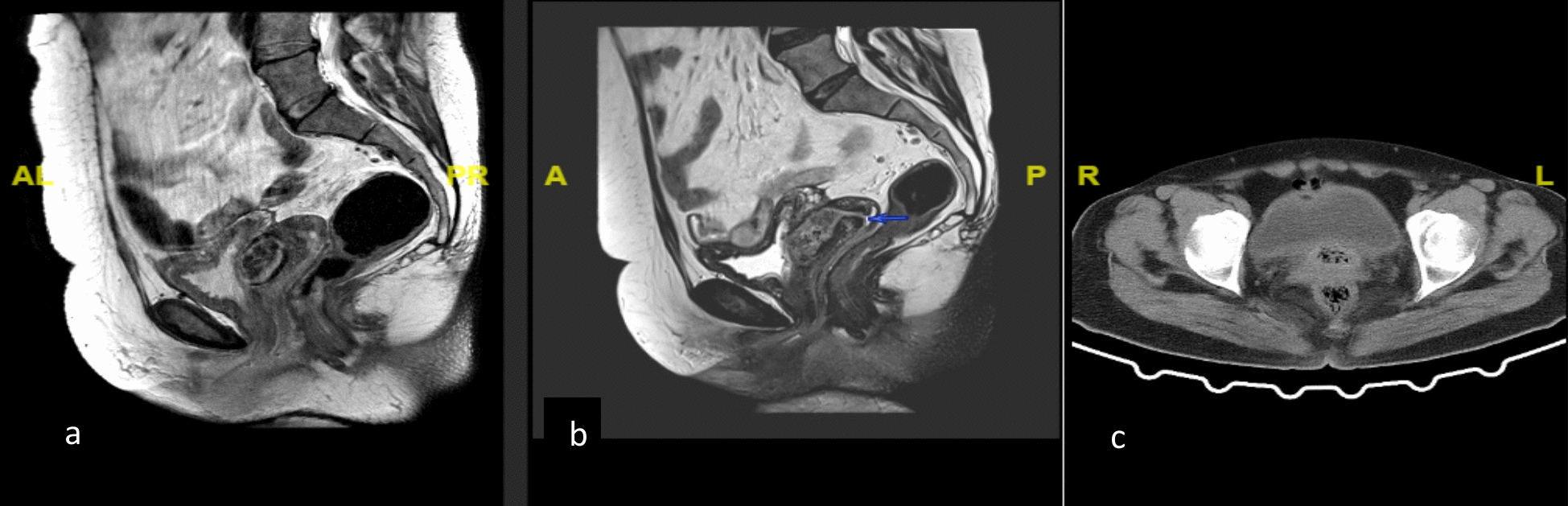
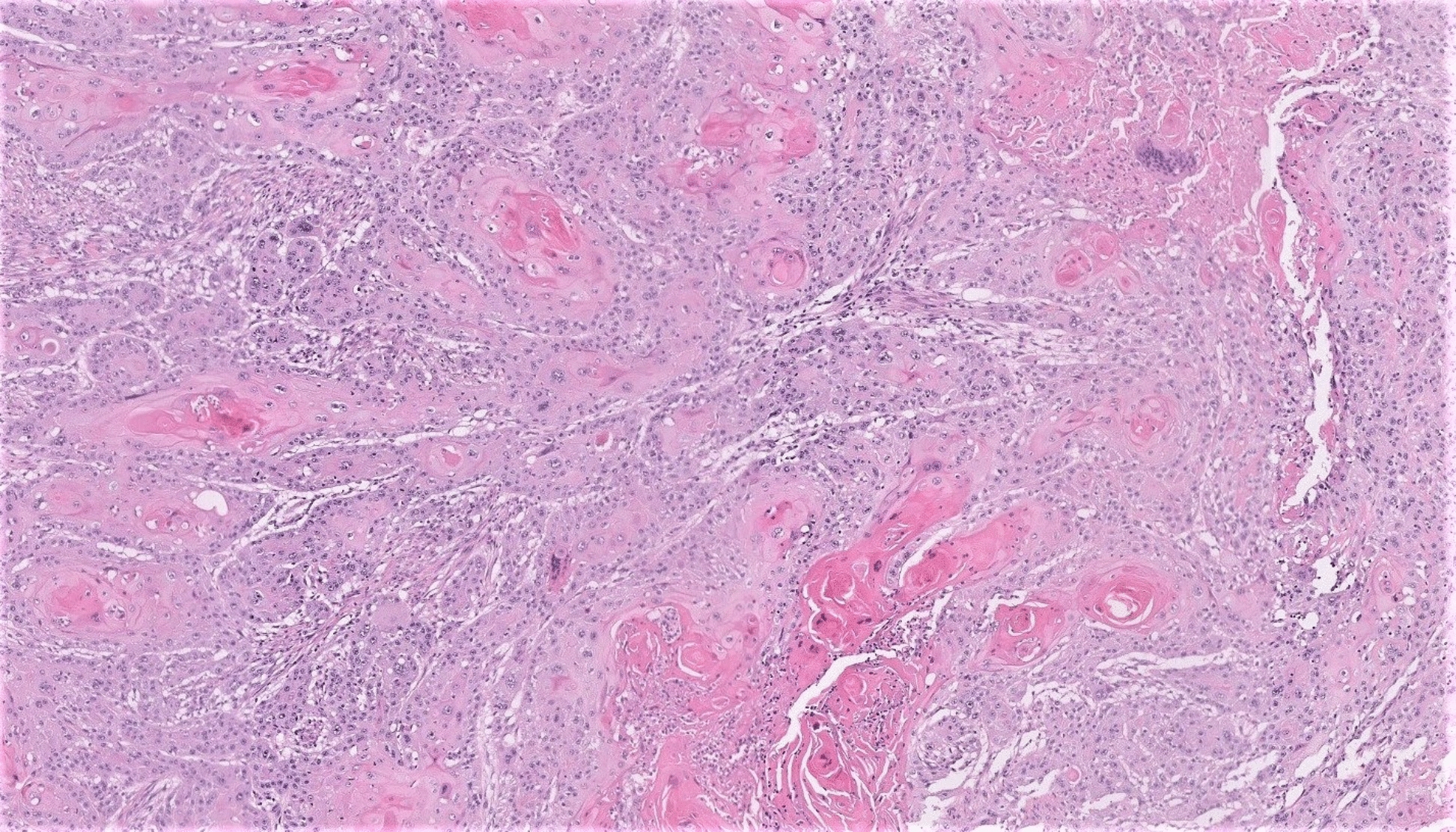
A 54-year-old post-menopausal female presented to the gynaecology OPD with complaints of pain in her abdomen for 5–6 months, relieved partially on medication, bloating for 3 months and abdominal distension for 2 months. The patient was planned for a primary cytoreductive surgery with Staging Laparotomy with Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy with Infracolic Omentectomy with retroperitoneal lymph node dissection. The final histopathology report showed primary high-grade serous cystadenocarcinoma of the fallopian tube spread to bilateral ovaries and omentum—FIGO Grade—III. Surgical Staging—FIGO Stage IIIA2.
Discussion
Pelvic (extrauterine) high-grade serous carcinomas including ovarian, tubal and primary peritoneal serous carcinomas have increased death:incidence ratio due to presentation at an advanced stage, rapid progression, poor prognosis and high morbidity. Ambiguity regarding their pathogenesis and lack of a proper screening method is the cause of their late detection and high fatality rate.
Conclusion
It is important to realise that the origin of a majority of serous cancers is from the distal fimbrial end of the fallopian tube, and thus, it is a partially preventable cause of high-grade serous cancers. This needs to be translated into the reporting by pathologists and subsequently to find out the true incidence of fallopian tube cancers.


Comments (0)