
Remember me


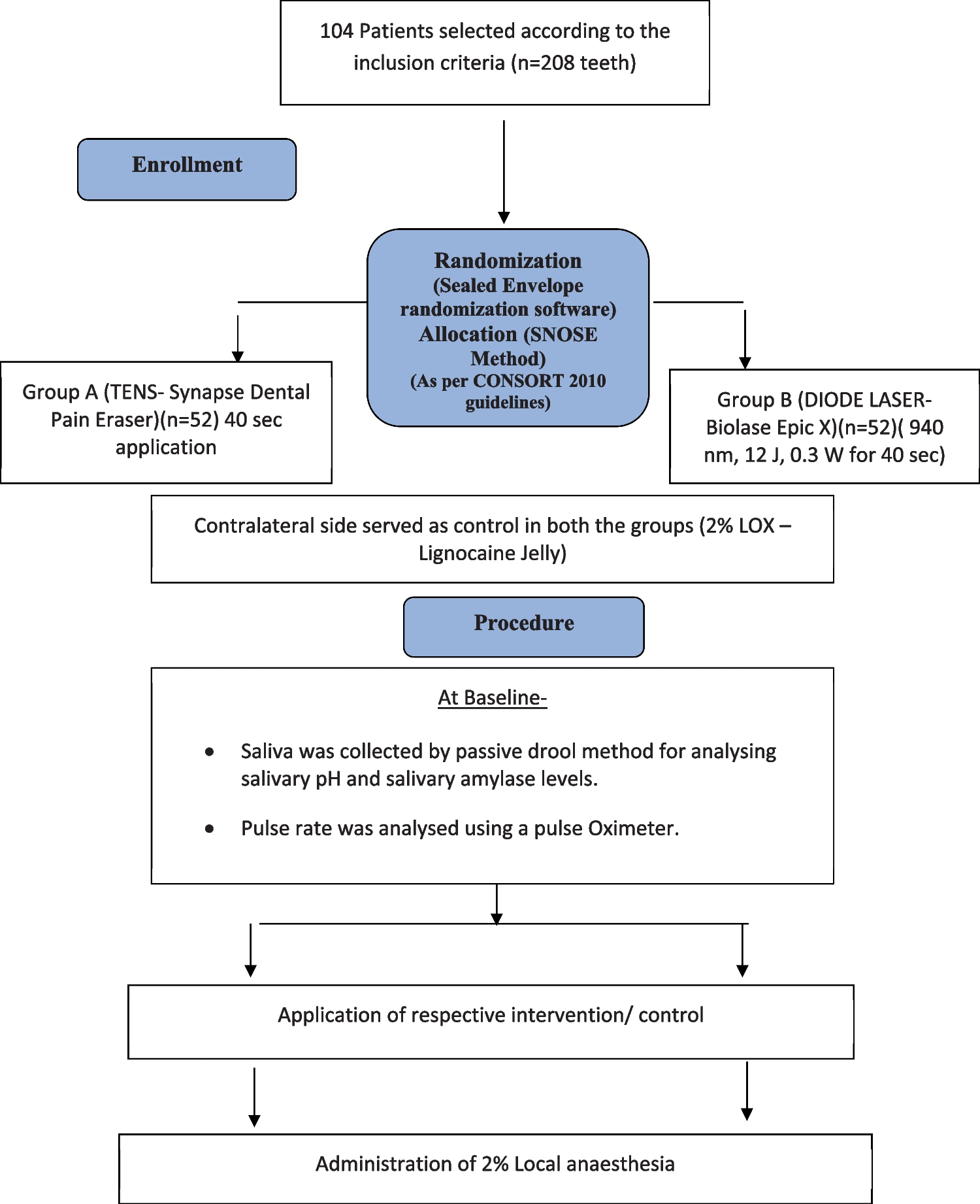
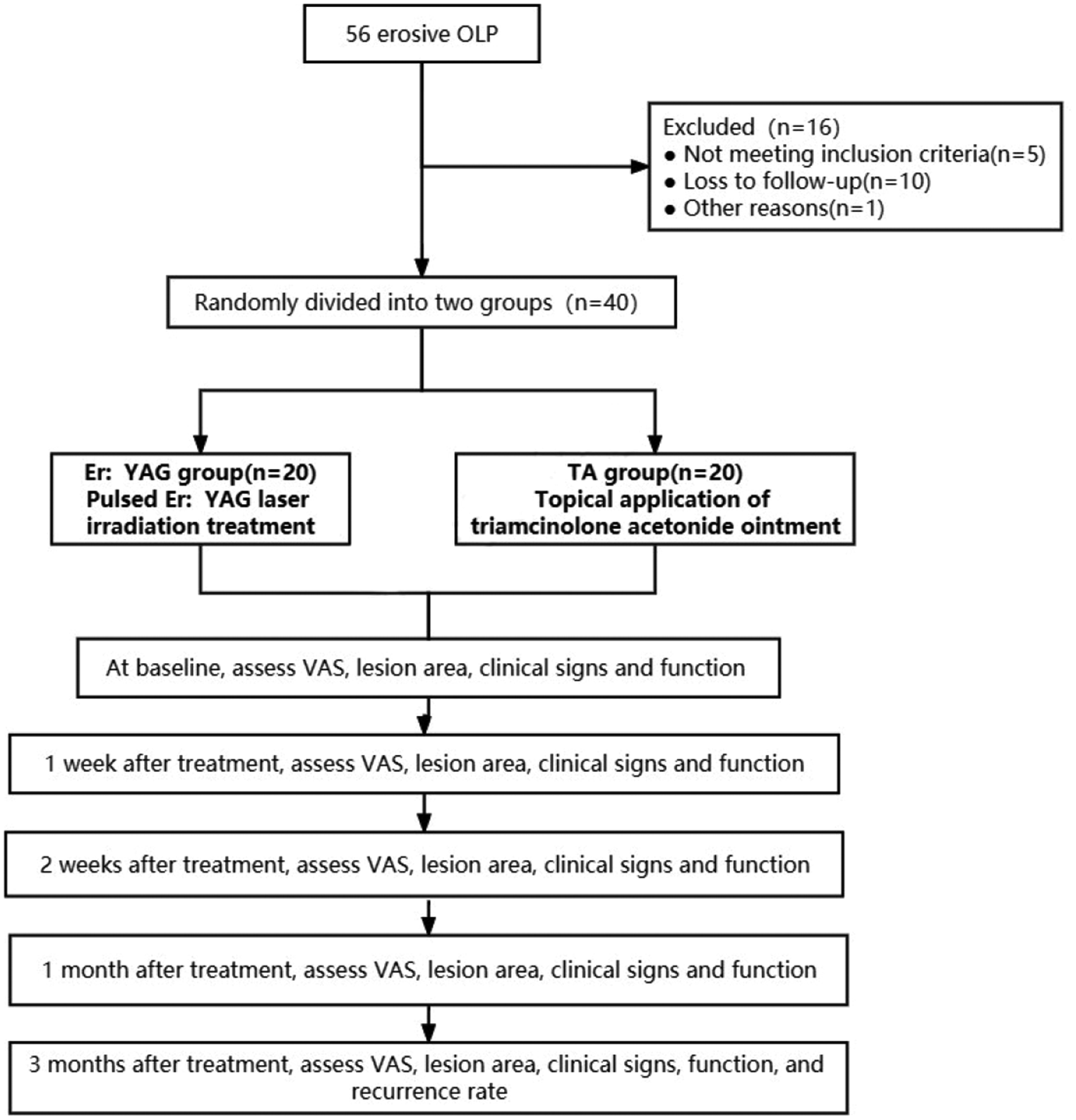
A total of 135 articles were retrieved from database searching. With duplicate removal, 93 articles were preliminary screened with title and abstract. Among them, eleven potentially eligible articles were identified for full-text retrieval, of which nine articles were ultimately included in the analysis. The detailed screening flow chart was presented in Fig. 1.
Fig. 1
Among the 9 articles, there were 2 randomized controlled trials (RCTs) [8, 11], 4 non-randomized comparative studies [9, 12,13,14], and 3 prospective cohort [15,16,17] studies. Four studies were from China [8, 11, 13, 14], 3 studies from Egypt [9, 12, 17], 1 from Iran [16] and 1 from Italy [15]. This study reviewed a total of 451 patients, ranging in age from 3 months to 47 years, with a slight male predominance (58.8%). Based on available data, there were at least 25 cases of bilateral CL/P and 133 cases of unilateral CL/P. Of these, 204 patients underwent primary repair surgery, while 105 patients received secondary repair surgery. Three studies limited patients’ Fitzpatrick skin phototype to III or IV type. Detailed information for each eligible study is presented in the Table 1.
Table 1 Details of included studiesTwo comparative studies [8, 11] exhibited a high risk of performance bias but were rated as low risk in other domains. Meanwhile, two other comparative studies [9, 13] were classified as high risk primarily due to their inadequate control over selection bias and performance bias. The remaining two comparative studies [12, 14] did not display the randomization and blinding process, thereby the relative bias risk is unclear (Fig. 2).
Fig. 2 Laser type
Laser typeThe fractional CO2 laser was the most commonly used laser type (n = 5), typically administered once every 4 weeks, with a total treatment course of 5–7 sessions. In a self-controlled study [11] the 595 nm pulsed dye laser (PDL) was applied every two weeks for 5 sessions. Low power diode laser 806 nm was utilized in a study with a denser interval (three times per week) and more sessions (12). Nocini et al. [15] used Er: YAG laser once every 3 months for two sessions. Peng et al. [14] combined intense pulsed laser (IPL) and fractional CO2 laser, administering the former once a month and the latter once every three months, resulting in a total treatment duration of six months. The intervention detail of each study was presented in the Tables 2 and 3.
Table 2 Detailed intervention information of comparative studiesTable 3 Detailed intervention information of non-comparative studiesVSSSix articles recorded the VSS scores change after laser treatment, with only four of them [8, 12, 14, 17] reporting mean values and standard deviations, which were suitable for data integration. All studies observed a significant decrease in scores after laser therapy, with an overall mean difference of 4.05 (95% CI, 2.10–5.99) (Fig. 3). The overall heterogeneity was significant with a I2 of 99%. The funnel plot displayed an asymmetric distribution, suggesting some publication bias (Supplemental Fig. 1). Further subgroup analysis according to the laser types showed that for factional CO2 laser treatment, the mean difference is 3.36 (95% CI, 2.45–4.07). One study [14] combined IPL and fractional CO2 laser and reported a difference of 7.60 (95% CI, 7.24–7.96).
Fig. 3
Forest plot of VSS scores
We also conducted separate meta-analysis for comparative results. One study [8] set three experimental groups with different intervention initiation time, while another study [12] set two experimental groups. Compared to control group (2 studies [12, 14] used scar creams and silica gel, 1 studies [8] did not provide detailed descriptions), the laser treatment groups have a lower mean VSS score of 1.34 (95% CI, 0.02–2.67) (Fig. 4).
Fig. 4
Forest plot of VSS scores for comparative studies
Two studies did not report data in the form of mean and SD. One study [11] conducted a randomized, self-controlled trial aimed at evaluating the efficacy of 595-nm PDL. At the 6-month follow-up, the relative change in VSS was 0.116 ± 0.336, significantly lower than that in the control group. An open-label study [9] compared low-power 806-nm diode laser with the control group. The median VSS score of laser group (median = 3) was significantly lower than the control group (median = 6.5).
Scar width/area/thicknessTwo studies assessed the scar width. Shadad et al. [12] found that the scar width in the early intervention group (2.51 ± 0.64) was significantly lower than that in the late intervention group (3.17 ± 0.54) and the control group (3.27 ± 0.48). However, in Mohsen's study, there was no significant difference in scar width between the low-power diode laser treatment group and the control group [9]. Mohsen et al. [9] also utilized ultrasound to measure the scar thickness and observed a reduction in scar thickness on the 14th day of laser treatment [9]. Detailed data on scar width or thickness were not provided in this study.
In Chi's self-controlled study, a 3dMD photographic measurement system was used to calculate scar area [11]. The mean area on the laser side (24.20 ± 10.95 mm2) was significantly smaller than that on the control side (31.19 ± 14.51 mm2) after treatment.
Other indicatorsLi et al. [13] utilized a subjective rating scale, grading the efficacy to obviously effective, effective and ineffective according to the change of pliability, color and thickness. In the laser treatment group, there was a notable prevalence of patients exhibiting obviously effective or effective efficacy compared to those in the control group. Quartile grading scale was employed in Jahanbin’s study [16] to assess the improvement of scar texture. 0 means minimal to no improvement while 3 represents near total improvement. The results were evaluated by two blind dermatologists and showed a mean of 1.29 ± 0.86, a median of 1.25 ± 1.38 after treatment. Nocini et al. [15] used patient satisfaction questionnaire as the primary indicator and the average satisfaction level is 8.8 (1: bad;10: high).
Some adjuvant assessments also performed in some studies as efficacy indicators, such as visual analog scale (VAS) [12], patient scar assessment questionnaire (PSAQ) [11, 16]. All the relative results support the efficacy of laser therapy in improving CL/P scar.
Optimal begin time of laser therapyThree cohorts [9, 11, 12] started intervention at the proliferative phase and five cohorts [8, 12, 13] initiated treatment at the remodeling phase. All cohorts that commenced intervention during the proliferative phase exhibited a significant therapeutic effect. Two cohorts [8] that initiated treatment during the proliferative phase (one at 3 months and the other at 6 months after surgery) demonstrated similar improvement post-treatment compared to the control group. The resting cohorts showed significant improvement. A meta-analysis was performed to assess the efficacy of intervention initiation approximately one month postoperatively compared to initiation at three months postoperatively. The results revealed that the VSS score was significantly lower in the former group, with a difference of 1.70 (95% CI, 1.33–2.08) (Fig. 5).
Fig. 5
Forest plot of VSS scores comparing different initiation time of treatment
ComplicationsNo severe complications were reported in included studies. However, transient erythema or swelling following Er:YAG laser treatment is commonly observed [15], with sporadic reports in other types of laser therapy. Additionally, Mossaad et al. documented patients complaining of discomforting pain during the treatment [17]. Overall, laser therapy is considered a safe treatment for preventing and treating CL/P scars.
Comments (0)