
Remember me
The National Health Insurance Service (NHIS) is a governmental single-insurance organization, and the NHIS provides health checkups, among other services. As health insurance members undergo health checkups every 1 or 2 years, the NHIS stores national health checkup data as well as claims data. The NHIS database contains an eligibility database (based on characteristics of age, sex, and socioeconomic status), a health checkup database (including common questionnaires on health-related habits, e.g., smoking status, alcohol intake, physical activity, medical history, and family history), measurement data (e.g., height, weight, and blood pressure), laboratory results (e.g., total cholesterol, fasting blood sugar, and serum creatinine), and a medical history database (e.g., diagnosis and medication). More detailed information regarding the health checkup database has been described previously [13].
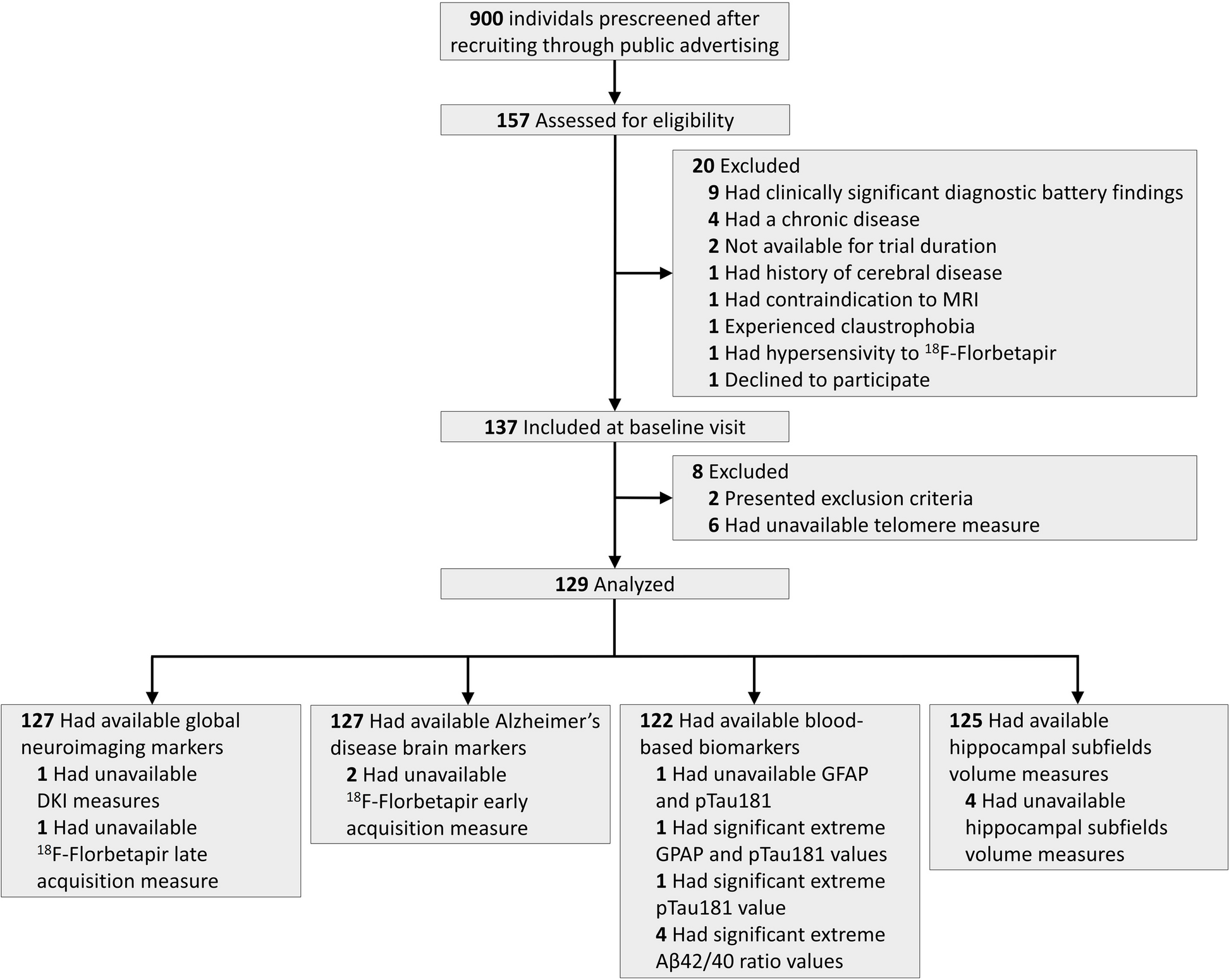
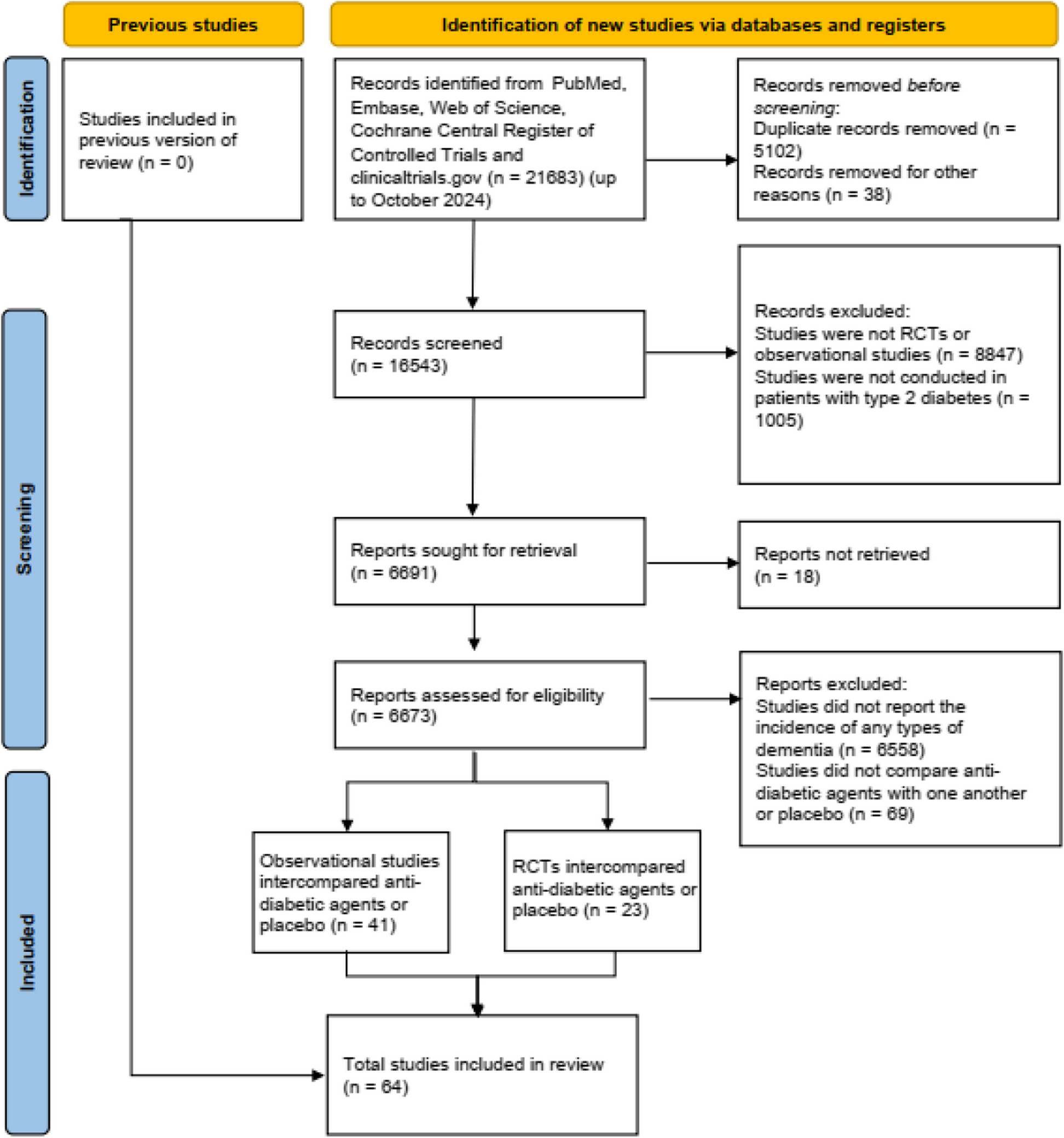
Data from participants aged ≥ 40 years in 2011 who underwent at least five health checkups between January 1, 2002, and December 2011 were screened and a total of 4,687,719 participants were included after the relevant exclusions. We excluded 137,264 participants with a previous diagnosis of dementia between 2002 and 2010/2011. To avoid the possibility of a time lag in the detection of dementia, we additionally excluded participants who were diagnosed with dementia within 5 years before the baseline (2010/2011). Participants were then followed up until the date of dementia onset or December 31, 2020, whichever came first. To achieve the objective of identifying BW variability in midlife and assess the risk of early dementia, we included participants with a baseline age < 65 years, which included 3,635,988 dementia-free middle-aged participants (Fig. 1). Our study focused on investigating how mid-life BW changes influence the risk of developing dementia before the age of 70 years. To assess this association, we included 3,635,988 dementia-free participants aged < 65 years.
Fig. 1
Flowchart of the study population
This study was conducted in accordance with relevant guidelines and regulations. The Institutional Review Board of Seoul National University Hospital waived the need for informed consent for this study because the analyses used existing data and there was no contact with individuals (IRB waiver No: E-2311-055-1483).
BW changeIntra-individual BW variability was assessed using variability independent of the mean (VIM) was k×standard deviation (SD)/meanT)β, where β was calculated from mean and SD using a fitting curve based on the model where SD = constant/meanβ [14, 15]. The BW cycle was evaluated with multiple thresholds (≥ 3%, ≥ 5%, ≥ 7%, and ≥ 10% of BW), defined as when BW changes in either an upward or a downward direction above a specified threshold percentage [12].
Clinical definitionsThe primary outcome of this study was newly diagnosed, physician-diagnosed dementia. Dementia was defined according to the International Classification of Diseases, 10th revision (ICD-10) codes: F00 (dementia in Alzheimer’s disease), F01 (vascular dementia), F02 (dementia in other diseases), F03 (unspecified dementia), F05 (senile dementia with delirium), and G30 (Alzheimer’s disease).
Information on health-related behaviors (smoking status, alcohol intake, and physical activity) and family history of hypertension (HTN), type 2 diabetes mellitus (DM), heart disease, and stroke was obtained from self-reported questionnaires. Smoking status was categorized as never smoker, ex-smoker, or current smoker. Alcohol intake were classified as none, < 10 g/day, 10–19.9 g/day, 20–39.9 g/day, and ≥ 40 g/day. Physical activity was defined using the long-form International Physical Activity Questionnaire (IPAQ), where individuals were classified based on metabolic equivalents (METS) value of < 600, 600–3000, and ≥ 3000 [16].
HTN was defined as systolic/diastolic blood pressure ≥ 140/90 mmHg or at least 3 months of medication. DM was defined as fasting blood sugar ≥ 126 or at least 3 months of medication. Further details of past medical history (HTN, DM, heart disease, and stroke) information was obtained from self-reported questionnaire.
Statistical analysisThe participants were classified into 36 groups according to the BW variability (VIM quartiles) and BW cycles. Data were presented as mean ± SD for continuous variables and counts (%) for categorical variables.
Hazard ratios (HRs) and 95% confidence intervals (CI) for incident dementia in relation to the BW change were estimated using a Cox proportional hazards model with follow-up time as the timescale. In the current study, the follow-up time was calculated as the time from the participants’ last health checkup between 2010 and 2011 until dementia diagnosis or the last health checkup. The time of dementia diagnosis was defined as the first date in the claims history containing the diagnosis codes.
We considered age, sex, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol, estimated glomerular filtration rate (eGFR), health-related behaviors (smoking status, alcohol intake, and physical activity), medical history (HTN, DM, heart disease, and stroke), and family history (HTN, DM, heart disease, and stroke) to be potential risk parameters of dementia in Cox-models. Stratified analyses using BMI, sex, and medical history of HTN and DM were conducted to examine the effect of modification of the variables.
Two-tailed P-values < 0.05 were considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R version 4.0.3 (R Core Team, Vienna, Austria).
Comments (0)