This retrospective study was approved by the Ethics Committee of the Second Affiliated Hospital, School of Medicine, Zhejiang University, and registered at http://www.clinicaltrials.gov (identification no. NCT04120389). Moreover, this study complied with the tenets of the World Medical Association of Helsinki.
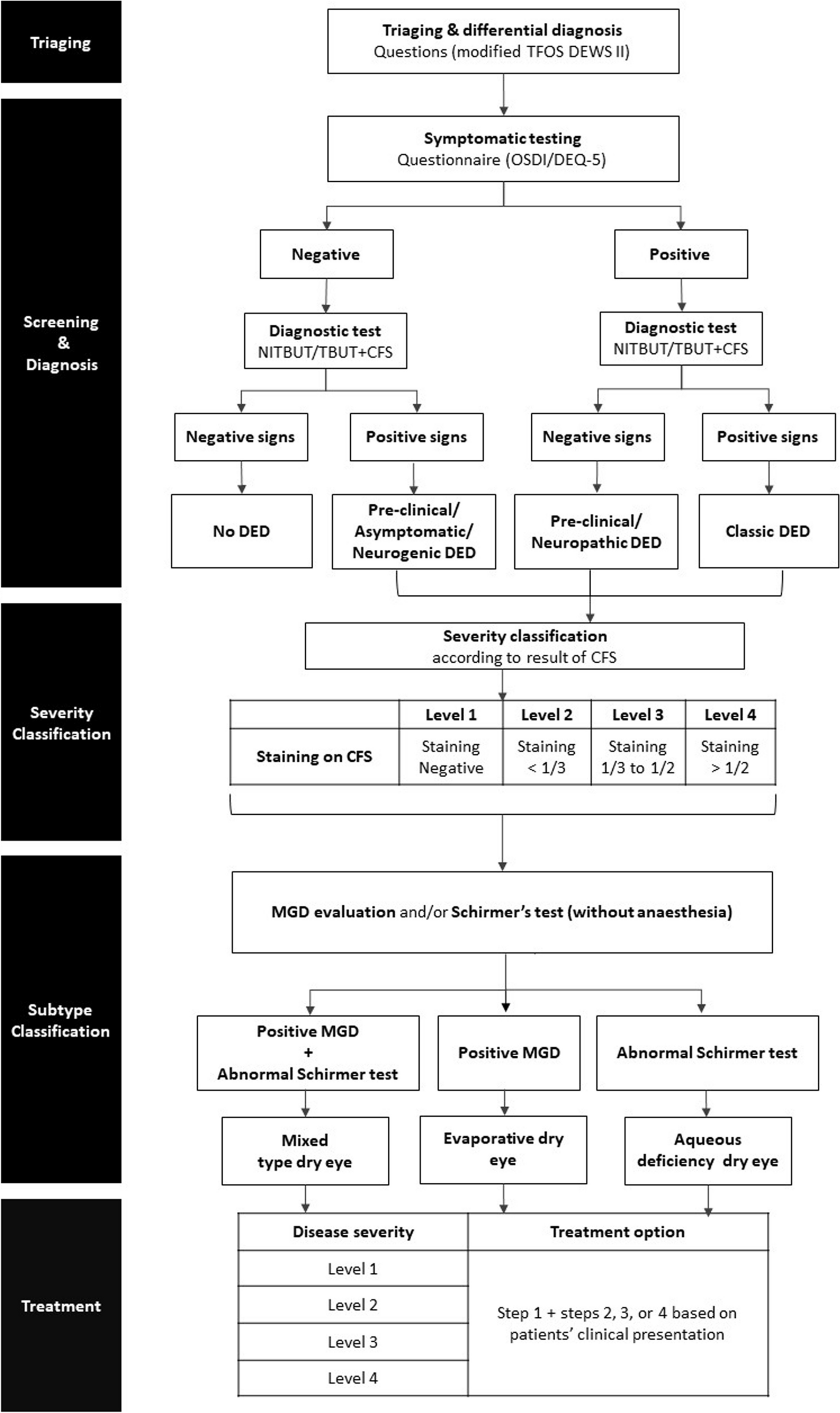
Diagnosis of DED met TFOS DEWS II diagnostic criteria, which required subjective symptoms [Ocular surface disease index (OSDI) ≥ 13] and at least one of the following results: (i) fluorescein break-up time (F-BUT) < 10 s, and (ii) the fluorescein staining score > 5 corneal spots [12].
Dry eye severity can be classified into three categories: (i) Mild: fluorescein staining spots less than 5 and F-BUT of 2 s or more. Defined as level 0. (ii) Moderate: fluorescein staining spots of 6 to 30, with the F-BUT of 2 s or more. Defined as level 1. (iii) Severe: fluorescence staining spots of 30 or more, with a BUT of less than 2 s. Categorized as level 2.
Study population and proceduresInclusion criteria
DED was diagnosed preoperatively, and complicated cataract or/and IOL surgery was required.
Complicated cataract or/and IOL surgery involves the use of multiple surgical techniques performed simultaneously, which may include: (1) phacoemulsification or/and IOL implantation, (2) anterior vitrectomy, (3) IOL scleral fixation, (4) capsular tension ring implantation with/without suture fixation and (5) iris repair or pupilloplasty.
Exclusion criteria
1.
Patients with immune system diseases (systemic immunosuppressants or long-term hormone use) and diabetes.
2.
Patients who postoperative lost-to-follow-up.
Ophthalmological assessments
OSDI questionnaire was adopted to assess subjective dry eye-related feelings. The OSDI questionnaire consisted of 12 questions and was divided into three sections as follows: (1) ocular subjective symptom subscore (items 1 to 5), (2) visual function subscore (items 6 to 9), and (3) environment-related visual subscore (items 10 to 12). Finally, the total score was calculated using the formula: (total score of all answered questions x100) / (total number of answered questions x 4).
Fluorescein breakup time (F-BUT) was performed to assess tear film stability. Briefly, a single fluorescein strip (Meizi, Liaoning, China) was placed in the conjunctival sac of the eye after instilling a drop of normal saline, and the patient was asked to stare straight ahead without blinking. The time from the last blink to the first appearance of a randomly distributed dry spot was measured in triplicate, and the mean value was recorded.
Corneal fluorescein staining was performed as previously described. If there were no punctate epithelial erosions (PEEs), the score was 0. If one to five PEEs were seen, the corneal score was 1, six to thirty PEEs were scored as 2, and > thirty PEEs were scored as 3. An additional point was added if (1) PEE occurred in the central 4-mm diameter portion of the cornea, (2) one or more filaments, or (3) one or more patches of confluent staining, including linear stains. The maximum possible score for each cornea was 6 [13].
The keratography analysis was performed by using a keratograph (Oculus, Wetzlar, Germany) to determine the bulbar redness score, tear meniscus height (TMH), noninvasive first break-up time (NIF-BUT), noninvasive average break-up time (NIAvg-BUT) and meibography structure.
The redness score was determined based on the area percentage ratio of blood vessels in the bulbar conjunctiva, which indicated the inflammatory condition.
TMH below the central pupil was determined by the keratography analysis to assess the secretion of tears and the patency of the lacrimal ductal system.
The degree of meibography losses was scored on the following scale: 0 (no loss of meibomian glands); 1 (area loss less than one-third of the total meibomian gland area); 2 (area loss between one-third and two-thirds of the total meibomian gland area); and 3 (area loss more than two-thirds of the total meibomian gland area). The total score was the sum of the scores of the upper and lower eyelids and was recorded as 0 to 6.
Schirmer I test was performed to assess the basic tear secretion function. The Schirmer tear test strip (Meizi, Liaoning, China) was placed in the middle of the lower eyelid, and the length of the test strip was recorded 5 min later.
Data collection
The study observation period spanned from the date the patient started receiving care at the study site until the last data point was recorded. All these ocular data were collected before the surgery and at 1 week and 1 month postoperatively.
Complicated cataract or/and IOL surgery
Preoperatively, levofloxacin 0.5% (Santen, Osaka, Japan) was instilled four times daily for 3 days. Pupillary dilation was achieved with one drop of tropicamide every 15 min, three times before surgery. The anesthesia method was parabulbar injection. All cataract or/and IOL surgeries were performed by the same ophthalmologist (X.W.).
The BCLs (Air OptixNight &Day Aqua-Soft Contact Lenses) were worn by the surgeon on the operating table to ensure sterility at the end of surgeries and removed by doctors at a 1-week follow-up postoperatively. Patients who did not have their own BCLs were covered with sterile gauze on the operating table by doctors.
Postoperatively, all patients were instructed to take methylprednisolone tablets (Pfizer Italia Srl, AP, Italy) orally at a dose of 12 mg per day for 3 days. Additionally, prednisolone acetate ophthalmic suspension (Allergan, Co., Mayo, Ireland), levofloxacin 0.5% (Santen, Osaka, Japan), and diclofenac sodium 1% (Qiyan, Shenyang, China) were instilled four times daily for 1 week after surgery. In the BCL group, while wearing the BCL, the eye drops were dropped into the fully exposed lower conjunctival sac after gently pulling the lower eyelid downwards. At the 1-week follow-up, the medication prescription was changed to 0.1% pranoprofen (Senju Pharmaceuticals, Kobe, Japan) and carbomer eye gel (Dr. Gerhard Mann, Berlin, Germany) four times daily until consumption.
The corresponding number of surgical techniques among the 69 patients included in the study is shown in Table 1.
Table 1 Surgical techniques involved in this studyStatistical analysis
Statistical analysis was performed using SPSS software (version 22.0, SPSS, Inc., Chicago, IL). The Chi-square test was used to compare the sex and laterality between the two groups. Normal distribution was confirmed using the independent-sample t-test to compare the differences between the two groups. Otherwise, the Mann-Whitney Utest was used. A repeated measures analysis of variance (ANOVA) test was performed to compare changes at all time points. Correlations between parameters were tested with the Pearson correlation coefficient (r). A P value of less than 0.05 was considered statistically significant.





Comments (0)