
Remember me
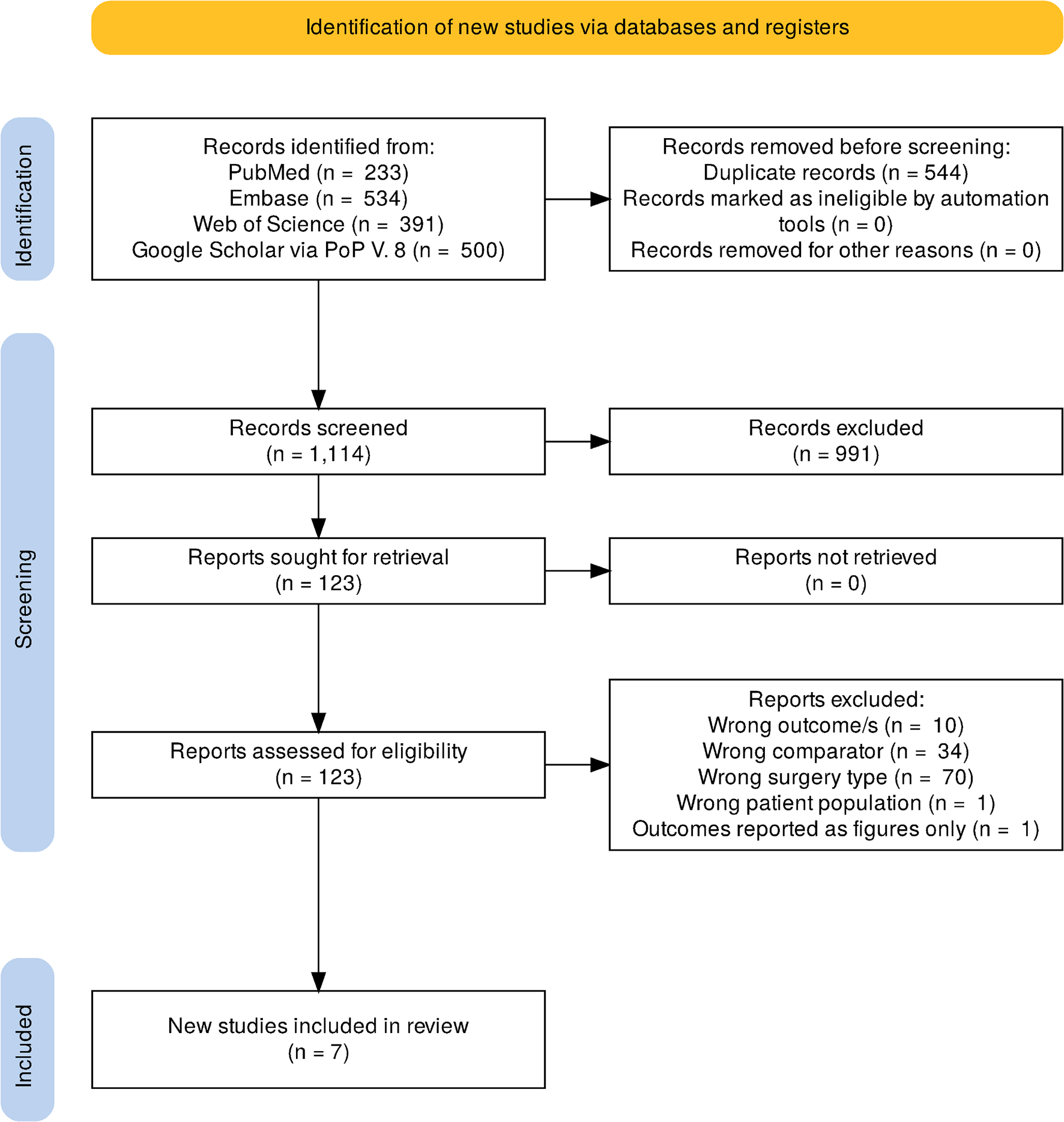

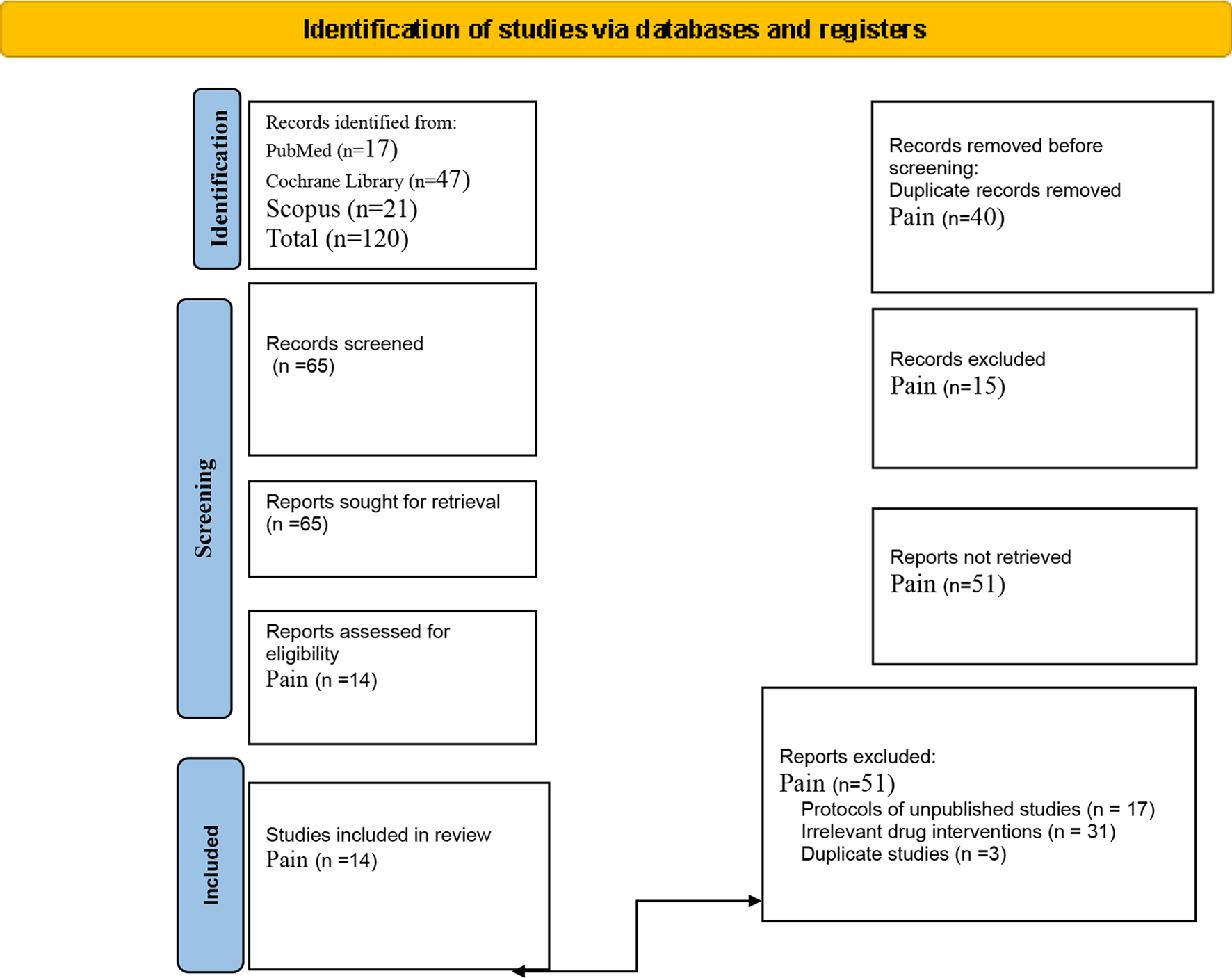

Twenty-two studies were included in our review out of 1281 studies (Fig. 1). With a total of 1429 patients, 703 patients in the ketadex group and 726 patients in the ketofol group. Patients’ age ranged between 2.4 ± 1.2 and 54.9 ± 5.3 years old. Patients in 13 included studies were ≥ 18 years old. Patients were scheduled for procedures such as gastrointestinal endoscopy, cardiac catheterization, elective daycare surgeries, and some other painful procedures in the emergency department. More details about the characteristics and summary of the included studies are shown in Table 1.
Fig. 1 Table 1 Summary and baseline characteristics of the included studiesQuality Assessment
Table 1 Summary and baseline characteristics of the included studiesQuality AssessmentRisk of bias assessment of the 22 included studies indicated a high risk of bias in six studies [8, 9, 13,14,15,16], an unclear risk of bias in nine studies [17,18,19,20,21,22,23,24,25], and a low risk of bias in seven studies [26,27,28,29,30,31,32], as shown in (Fig. 2).
Fig. 2
Summary of Risk of Bias in the included studies
Efficacy OutcomesRecovery TimeThirteen studies reported the recovery time by minutes after the surgery in 823 patients (413 ketadex vs 410 ketofol). The pooled mean difference showed a significant difference between the two groups of 7.59 min (95% CI, 4.92, 10.26; I2 = 94%) indicating longer recovery time in the ketadex group. Additionally, subgroup analysis showed a significant difference between the two groups with the ketadex group having a longer recovery time in pediatrics and adults at 8.34 min (95% CI, 4.43, 12.25; I2 = 93%) and 5.86 min (95% CI, 1.12, 10.60; I2 = 96%), respectively (Fig. 3).
Fig. 3
Forest plot of Recovery time outcome with age subgroups
Furthermore, we performed subgroup analysis according to the procedure and recovery score. Seven studies used the combinations for cardiac catheterization and three studies for UGIE showed a significant mean difference that favors ketofol 10.08 min (95% CI, 2.49, 17.67; I2 = 91%) and 9.86 min (95% CI, 7.86, 11.86; I2 = 70%) (Fig. S1). Six studies used Steward Score ≥ 6 and three studies used Aldrete Score ≥ 9 showed a significant mean difference that favors ketofol (Fig. S2). All included studies showed longer recovery time with the ketadex group irrespective of the type of the procedure and recovery score, except for data from three studies (Yeter et al. 2012, Smisek 2016, and Canpolat 2017) in which the difference was not of statistical significance.
Pain ScoreFour studies reported the pain score by the visual analogue scale (Fig. 4) and showed that 248 patients experienced less pain with the ketadex group than with the ketofol group. The pooled mean difference was statistically significant − 0.72 (95% CI, − 1.10, − 0.34; I2 = 0%). Both age groups experienced less pain in the ketadex group, but the mean difference was significantly lower in adults and the insignificant difference in pediatrics − 0.91 (95% CI, − 1.06, − 0.76; I2 = 0%) and − 0.40 (95% CI, − 1.09, 0.29; I2 = 61%), respectively (Fig. 4). Azizkhani et al. used the combinations for painful procedures in the emergency room in two studies with no pooled difference between the combinations − 0.55 (95% CI, − 1.44, 0.34; I2 = 84%). However, Azizkhani et al. (July) 2021 found significantly less pain in the ketadex group (Fig. S3).
Fig. 4
Forest plot of Pain score outcome with age subgroups
Physician SatisfactionGood or Excellent physician satisfaction scores were reported in six studies. The pooled odds ratio was not statistically significant, being 0.44 (95% CI, 0.15, 1.29; I2 = 73%). Adults had a significantly better physician satisfaction score with the ketofol group, odds ratio of 0.29 (95% CI, 0.12, 0.71; I2 = 0%). But in pediatrics, the pooled odds ratio showed insignificant better physician satisfaction with ketofol in pediatrics (Fig. 5). After the removal of Amer et al. as a potential cause of heterogeneity, we found significant pooled odds ratio in total events and pediatrics 0.25 (95% CI, 0.13, 0.47; I2 = 0%) and 0.21 (95% CI, 0.08, 0.53; I2 = 2%) with no heterogeneity between the studies (Fig. S4).
Fig. 5
Forest plot of Physician satisfaction outcome with age subgroups
Safety Outcomes:Cardiovascular Adverse EventsBradycardia events were reported in eight studies of 488 children. The incidence of bradycardia was significantly higher in the ketadex group at 9.43% than in the ketofol group at 4.5%, odds ratio of 2.12 (95% CI, 1.03, 4.35; I2 = 0%). The difference between the two combinations was not statistically significant in both age subgroups (Fig. 6), and the procedure type (Fig. S5).
Fig. 6
Forest plot of Bradycardia outcome with age subgroups
Tachycardia events were reported in four studies of 249 children. The incidence of Tachycardia was more in the ketofol group 9.6% compared to the ketadex group 4.8% with pooled odds ratio of 0.51 (95% CI, 0.15, 1.76; I2 = 0%), but there was no statistically significant difference between the two combinations in both adults and pediatrics (Fig. 7). The incidence of Tachycardia was insignificant more with the ketofol group after upper gastrointestinal endoscopy, odds ratio of 0.25 (95% CI, 0.06, 1.11; I2 = 0%) (Fig. S6).
Fig. 7
Forest plot of Tachycardia outcome with age subgroups
Hypotension events were reported in 44 patients. The difference in hypotension incidence between the two combinations was not of statistical significance, odds ratio of 1.11 (95% CI, 0.59, 2.08; I2 = 27%) (Fig. 8). Also, hypertension events from two studies reported the same incidence in both combinations leading to statistically insignificant difference, odds ratio of 1.00 (95% CI, 0.35, 2.88; I2 = 0%, P = 1.00) (Fig. 9).
Fig. 8
Forest plot of Hypotension outcome with age subgroups
Fig. 9
Forest plot of Hypertension outcome with age subgroups
Respiratory Adverse EventsBradypnea events were reported in nine patients of three studies. The incidence of Bradypnea in the ketadex was 2.7% while in the ketofol was 5.5%. There was no significant difference between the combinations with an odds ratio of 0.58 (95% CI, 0.18, 1.89; I2 = 58%) (Fig. 10). Additionally, airway obstruction events showed a significant difference between the combinations with an odds ratio of 0.70 (95% CI, 0.22, 2.27; I2 = 0%) (Fig. 11).
Fig. 10
Forest plot of Bradypnea outcome with age subgroups
Fig. 11
Forest plot of Airway Obstruction outcome with age subgroups
Hypoxia events were reported in 129 patients of 12 studies. The incidence of hypoxia was lower in the ketadex group 12.4% than in the ketofol group 20.3%; the difference between the two groups was statistically significant with an odds ratio of 0.49 (95% CI, 0.32, 0.76; I2 = 0%). The difference in the incidence of hypoxia was not statistically significant between the combinations in adult patients, odds ratio of 0.55 (95% CI, 0.29, 1.03; I2 = 4%), while the difference remains statistically significant in the pediatric patients, odds ratio of 0.45 (95% CI, 0.25, 0.81; I2 = 0%) (Fig. 12). The incidence of hypoxia remained higher in the ketofol group throughout all different types of procedures, with no statistically significant difference between the two groups in any type of procedure (Fig. S7).
Fig. 12
Forest plot of Hypoxia outcome with age subgroups
Gastrointestinal Adverse EventsPost-operative nausea and/or vomiting (PONV) was addressed as a single side effect in most of the studies, so we did the same in our analysis. Thirteen studies reported PONV in 78 patients. We found a statistically significant difference between the combinations with a higher incidence in the ketadex group11.2% than in the ketofol group 7% with pooled odds ratio of 1.75 (95% CI, 1.06, 2.88; I2 = 15%). Also, we found that ketadex caused statistically significant higher incidence in the adult group with pooled odds ratio of 2.17 (95% CI, 1.18, 4.00; I2 = 0%), while there was no statistically significant difference between both combinations in the pediatrics (Fig. 13).
Fig. 13
Forest plot of Post-operative Nausea and/or vomiting with age subgroups
PONV occurred more in the ketadex group regardless of the type of the procedure, except with dental treatment, which showed the same incidence in both groups (Fig. S8).
Salivation events were reported in 21 patients of four studies. The incidence of salivation was higher in the ketofol group 13.2% than in the ketadex group 6.7%. However, we found a statistically insignificant pooled odds ratio of 0.48 (95% CI, 0.19, 1.22; I2 = 0%) (Fig. 14).
Fig. 14
Forest plot of Salivation outcome with age subgroups
Neurological Adverse EventsRecovery agitations were reported in 29 patients of ten studies. The incidence in the ketofol group 7.6% was higher than in the ketadex group 4% with significant odds ratio of 0.48 (95% CI, 0.24, 0.98; I2 = 36%) (Fig. 15).
Fig. 15
Forest plot of Recovery agitations outcome with age subgroups
Hallucination events were reported in only two studies in ten patients. Hallucination events appear to occur more in the ketofol group 11.3% while 4.8% in the ketadex group. However, there was insignificant odds ratio between both combinations 0.43 (95% CI, 0.11, 1.63; I2 = 2%). Both studies performed painful procedures in the emergency department (Fig. 16).
Fig. 16
Forest plot of Hallucination outcome with age subgroups
Comments (0)