
Remember me
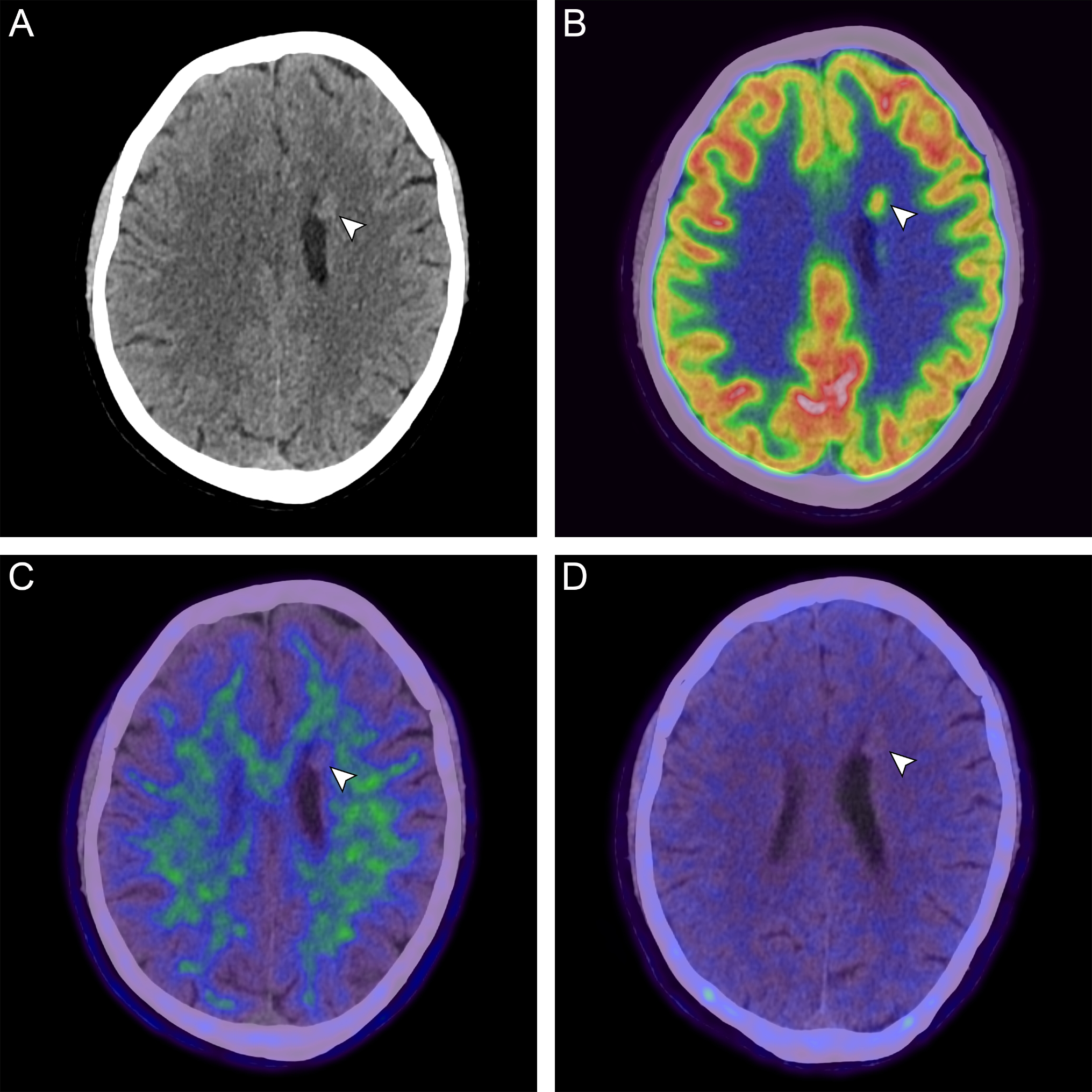
An 84-year-old male presented with transitional meningioma WHO° 1 (Figure part A, prior to resection). After completed therapy (resection, cyberknife radiosurgery, fractionated radiation), he showed right-sided residues infiltrating the transverse and sigmoid sinuses (Figure part B, after multimodal therapy). At follow-up 12 months later, MRI showed a new heterogeneous contrast enhancement in the left occipital resection cavity, suggestive of tumor progression (Figure part C, follow-up) [1]. Due to limited availability of somatostatin receptor (SSTR) PET imaging, [18F]FET PET was performed as an alternative method. The left occipital lesion showed minor radionuclide uptake on [18F]FET PET (TBRmax: 2.4, TBRmean: 1.2; red arrow), whereas the right-sided meningioma showed intense uptake (TBRmax: 4.6; white arrow). Analysis of [18F]FET uptake dynamics revealed decreasing time–activity curves (TTPmin:12.5 min) in the right-sided meningioma and increasing curves in the left occipital lesion. Three weeks later, we performed SSTR imaging using [18F]SiTATE, showing typical SSTR expression of the right-sided meningioma (SUVmax: 17.1; white arrow), but no typical SSTR expression in the left occipital lesion (SUVmax: 1.9; red arrow) [2]. Together with the moderate [18F]FET uptake, these findings were interpreted as pseudoprogression, confirmed by further follow-up.
The incidence of posttherapeutic pseudoprogression in meningioma is still unknown but considered rare [3]. With an increasing range of treatment options, diagnostic strategies are required to distinguish tumor recurrence more accurately from pseudoprogression [3]. However, when rapid clinical access to SSTR imaging is limited, this may delay diagnosis [4, 5]. To our knowledge, this is the first case demonstrating the value of dual tracer PET imaging in the detection of pseudoprogression in meningioma.

Comments (0)