
Remember me
The CMRG-DB identified 663 patients with MM refractory to anti-CD38 mAb therapy. From them, 466 (466/663, 70%) patients initiated a subsequent regimen, 145 (145/663, 22%) pursued palliative care, and 52 (52/663, 8%) were lost to follow-up. Of the 197 patients not receiving subsequent treatment at the time of progression or lost to follow-up, the median age was 72 years, and the median overall survival from the time of index regimen progression was 1.3 (95% CI 0.4–1.7) months. Of these untreated patients, 137 (137/197, 70%) had TCR MM, and their median age at progression on the index regimen was 71 years (range 42–91) with a median of 4 (range 2–9) lines of treatment including the index regimen. Overall, 42 patients (42/663, 6.3%) were had penta-refractory MM at progression on the index regimen; 22 did not undergo further treatment and 20 received subsequent treatment on a clinical trial (n = 11) or with SoC regimens (n = 9).
Treatment post CD38-mAb progressionOf the 466 patients receiving subsequent treatment, 120 patients were treated on clinical trial and were excluded. Therefore, 346 patients treated with SoC regimens were included in this study, as shown in Fig. 1. Most patients (338/346, 98%) had MM refractory to daratumumab, with only a minority (8/346, 2%) receiving isatuximab as part of the index regimen. Seven patients progressed on a first-line regimen containing daratumumab. Sixty-three percent (218/346) of included patients previously received an autologous stem cell transplant, and most patients had MM refractory to lenalidomide or bortezomib (305/346 or 88% and 184/346 or 53%, respectively), as shown in Table 1. Of the 109 patients with disease progression on DVd, 87 had bortezomib (and TCR) refractory disease and 22 had non-TCR MM at progression (18 patients had disease progression on bortezomib, and 4 patients discontinued bortezomib >60 days prior to progression on DVd). The median age at initiation of subsequent therapy was 68 (range 40–90) years. The median time from diagnosis to initiation of subsequent SoC therapy after progression on the index regimen was 57 (range 6–283) months, and the median number of prior treatment lines was 3 (range 1–9). The most common SoC regimen used after progression on the index regimen was a PI/steroid doublet, followed by either a combination of PI or IMiDs with an alkylator (most commonly cyclophosphamide), as summarized in Fig. 2 and Table 2. PFS and OS outcomes, stratified by the most common regimens, are shown in Fig. S1. Twenty-seven patients (27/346, 8%) were re-treated with a CD38-mAb at progression on the index regimen (25 of these patients switched to a different anti-CD38 mAb), with a median washout period of 1.1 (range 0–7.0) months.
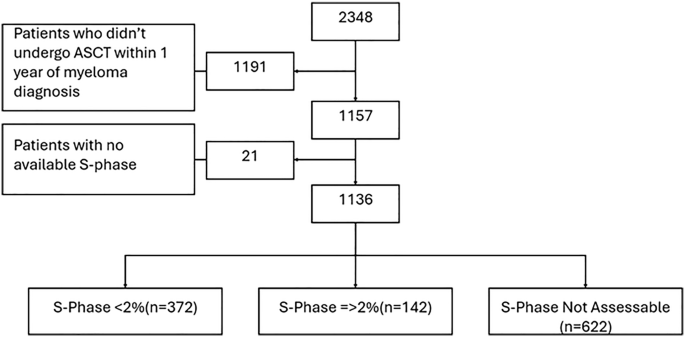
Fig. 1: Consort diagram of included patients.
Abbreviations: monoclonal antibody (mAb) triple class refractory (TCR).
Table 1 Characteristics of patients with anti-CD38 mAbs refractory MM that were treated with subsequent standard of care therapy.Fig. 2: Frequency of standard of care (SoC) drug regimens used after relapse on the index anti-CD38 monoclonal antibody containing regimen.
All regimens were given in conjunction with steroids. Of the patients with MM relapsing on 1st SoC therapy after index progression, 130 were treated with a 2nd Soc therapy and 81 were treated on clinical trial.
Table 2 Characteristics of patients with anti-CD38 mAb refractory MM stratified by the subsequent standard of care therapy received after progression on the index regimen.Efficacy outcomes post CD38-mAb progressionThe median follow-up from the date of initiation of subsequent SoC therapy was 8 months. Among the entire cohort of patients with MM refractory to an anti-CD38 mAb and treated with subsequent SoC therapy (n = 346), the median PFS from start of subsequent therapy was 4.6 (95% CI 4.1–5.6) months, and the median OS was 13.3 (95% CI 10.6–16.6) months (Fig. 3). The median PFS and OS was similar after excluding the 7 patients that had disease relapse on front-line daratumumab (median PFS 4.6 [95% CI 4.0–5.5] months, median OS 13.2 [95% CI 10.4–15.3] months). The overall response rate (ORR) to first subsequent SoC therapy was 48% (131/273), and 7% (18/273) achieved at least a complete response (CR) among patients evaluable for response assessment, as shown in Table 3. Among the 84 patients with high-risk cytogenetic markers at diagnosis, the median PFS and OS from initiation of subsequent therapy after progression on the index regimen were 3.5 (95% CI 2.5–6.3) months and 10.7 (95% CI 7.2–14.2) months, respectively. Response rates for high-risk patients treated with SoC subsequent therapy are summarized in Table S2.
Fig. 3: Outcomes of patients with TCR versus non-TCR RRMM.
A Progression-free survival (PFS) and B Overall survival (OS) from initiation of subsequent standard of care therapy post anti-CD38 mAb progression.
Table 3 Best response (among evaluable patients) to subsequent SoC therapy after progression on the index regimen.Of the 346 patients with MM relapsing on the index regimen and treated with a SoC subsequent line of therapy, 83 (83/346, 24%) were ≥75 years at relapse, and 263 (263/346, 76%) were <75 years. Among patients ≥75 years, the ORR to subsequent line of therapy was 38% (101/263), the median PFS was 4.4 (95% CI 3.5–6.3) months, and the median OS was 9.2 (95% CI 7.3–13.8) months. Among patients <75 years, the ORR to subsequent line of therapy was 36% (30/83), the median PFS was 4.1 (95% CI 3.4–5.1) months, and the median OS was 14.2 (95% CI 11.1–18.3) months.
Outcomes among patients with TCR versus non-TCR MMOne hundred and ninety-nine (58% of the included study cohort, 199/346) patients had TCR MM and were treated with SoC regimens after progression on anti-CD38 mAb. Next line of therapy among patients with TCR MM was most commonly a combination of PI/steroid (53/199, 27%), IMiD/alkylator (46/199, 23%), PI/alkylator (29/199, 15%), or PI/IMiD (24/199, 12%). No patients received anti-BCMA therapy, an XPO1 inhibitor, or venetoclax directly after progression on the index regimen as these were not available as SoC in Canada. The ORR was 40% (65/161) to the first subsequent line of therapy, with 5% (8/161) of patients achieving a CR or better (see Table 3). The ORR of patients with TCR MM stratified by type of subsequent SoC regimen received is summarized in Table S3. Fourteen (14/199, 7%) patients with TCR MM were re-treated with an anti-CD38 mAb in combination with either an IMiD or PI in next line of therapy after progression on the index regimen, and 8 patients achieved at least a partial response (ORR 57%, 8/14 patients). Of the 147 patients who had non-TCR MM at progression on the index anti-CD38 mAb containing regimen, 123 (123/147, 84%) were had TCE MM.
Among patients with TCR MM, the median follow-up from the date of initiation of subsequent SoC therapy was 7.2 months. The median PFS from the start of subsequent therapy was 4.4 (95% CI 3.6–5.3) months, and the median OS was 10.5 (95% CI 8.5–13.8) months. We then performed sensitivity analyses among the patients with TCR MM to identify whether there was a subgroup that had inferior outcomes. Among the 48 patients with TCR MM and high-risk cytogenetic markers at diagnosis (48/199, 24%), the median PFS and OS from initiation of subsequent therapy after progression on the index regimen were 2.8 (95% CI 2.3–6.1) months and 8.5 (95% CI 4.7–12.4) months, respectively. Similarly, patients with TCR MM and a duration of response on the index anti-CD38 mAb containing regimen of less than 1 year had a trend towards a shorter PFS (161/199 [81%], median PFS 3.9 [95% CI 3.0–5.1] months) compared to patients with a response of ≥1 year (38/199 [19%], median PFS 6.1 [95% CI 3.9–7.3] months).
We compared the median PFS and OS from the start of the subsequent therapy for patients with non-TCR versus TCR MM when progressing on the index regimen. Both the median PFS and OS were significantly longer among patients with non-TCR versus TCR MM (median PFS 6.0 versus 4.4 months, respectively, p = 0.009; median OS 17.5 versus 10.5 months, respectively, p = 0.003 (see Fig. 3). Similarly, we compared the median PFS and OS from the start of the subsequent therapy for patients with TCR versus TCE (and not TCR) MM. The median PFS of patients with TCR vs TCE MM was similar (mPFS 4.4 (95% CI 3.6–5.3) months versus 4.5 (95% CI 3.9–7.9) months, p = 0.06), however OS was significantly shorter among patients with TCR vs TCE MM (mOS 10.5 (95% CI 8.3–13.4) months versus 17.4 (95% CI 12.3–26.6) months, respectively, p = 0.01), see Figure S2.
Outcomes of patients with TCR MM treated with a second subsequent SoC regimen (including compassionate belantamab mafodotin (n = 1) and selinexor (n = 5)) after anti-CD38 mAb progression were even poorer (n = 50 TCR patients, ORR 30% [15/50 patients], CR 2% [1/50 patients]; median PFS and OS from start of second subsequent SoC treatment were 2.8 (95% CI1.8–4.6) months versus 6.4 (95% CI 3.7–18) months, respectively).
Predictors of response and outcomesMultivariable regression found no significant association between age at initiation of subsequent therapy, sex, high-risk cytogenetics at diagnosis, the number of prior treatment lines, or the time from diagnosis to progression on the index regimen and PFS (Fig. S3). Patients achieving at least a VGPR on the index anti-CD38 mAb-containing regimen had a significantly longer PFS (HR 0.23, 95% CI 0.13–0.40, p < 0.001) and OS (HR 0.30, 95% CI 0.15–0.58, p < 0.001) after adjusting for confounders. When assessing factors associated with OS from the start of subsequent SoC therapy in a multivariable analysis, not surprisingly, younger patients had an improved survival compared to older patients after adjusting for confounders (HR 0.62, 95% CI 0.42–0.93, p = 0.02). Patients with a more aggressive disease course whose time from diagnosis to progression on the index regimen was shorter (<4 years) had a worse overall survival compared to patients with >4 years from diagnosis to progression (HR 1.59, 95% CI 1.09–2.36, p = 0.020), after adjusting for confounding. There was no association between sex, high-risk status at diagnosis, depth of response on the index regimen (summarized in Fig. S4).
Comments (0)