To our knowledge, only one study group (Chinese APL Cooperative Group) has reported multicenter randomized studies comparing RIF and ATO in adult APL [2, 3]. This study is the first multicenter and randomized trial comparing oral RIF and intravenous ATO in the treatment of pediatric APL. With a median 6-year follow-up, children with APL in all risks treated on SCCLG-APL protocol had long-term OS and EFS of 100% and 96.6%, respectively, at 8 years, and the EFS were not significantly different between the two groups regardless of risk stratification at diagnosis.
The incidence of infection or FUO was significantly lower in the RIF group. RIF can be taken orally in an outpatient setting when the disease is stable, which decreases the risk of cross-infection in the hospital and iatrogenic infection due to PICC line placement, altogether resulting in shorter hospital stays. Moreover, the total incidence of cardiac adverse events during consolidation tended to be lower in the RIF group than in the ATO group (p = 0.054) (Table 3 and Suppl. Table S4), which supports the result obtained by a retrospective study in children [14]. However, the advantages of less infection and cardiac toxicity in APL treatment with RIF than with ATO were not observed in trials conducted in adult patients [2, 3], which again highlights the distinctions between pediatric and adult patients with APL.
Treatment intensity can be further reduced in the arsenic and ATRA era, as reported recently that chemotherapy-free treatment was used for patients with NHR APL, and intrathecal may not be required for those without central nervous system leukemia or intracerebral hemorrhage [3, 11, 12, 15, 16]. There is concern that the use of the two differentiating agents (arsenic and ATRA) without chemotherapy in induction may result in an increasing risk of leukocytosis and differentiation syndrome [17]. Previous studies suggested that the incidence of leukocytosis (>10 × 109/L) in pediatric patients with NHR APL was 84%–100% [9, 10] and much higher than 35%–47% [10,11,12] occurred in adult counterpart, if treated with the CHT-free induction. One study reported CHT-free induction treatment with ATRA and arsenic in children with NHR APL and administering anthracycline only to those with HR APL [15], the total incidence of DS was 41% and much higher than the 6.8% in our cohort (Suppl. Table S3). Another clinical trial also conducted in children with NHR APL showed that the CHT-free induction resulted in 24.5% (24/98) of children having DS [16]. Of those having DS, 70.8% and 50.0% had respiratory distress and hypoxemia, respectively, 16.7% to 29.2% had pulmonary infiltrates, pleural effusion, and hypotension, 8.3% had acute renal failure, and one died of DS. Therefore, to investigate the safety of the CHT-free induction in children with NHR APL, SCCLG-APL has initiated a new randomized study to compare induction treatments with and without an addition of one dose of anthracycline to ATRA and arsenic.
Arsenic retention is another major concern, especially in children treated with arsenic. To our knowledge, there has been no study comparing arsenic retention in children between treatments with RIF and ATO. A single-arm study investigated arsenic levels in plasma, hair, nail, and urine at different treatment time points in children with APL treated with ATO or RIF, and showed that the arsenic levels of the first three (except urine) returned to normal after 6 months stopping arsenic administration [15]. In this study, we used urinary arsenic excretion rate (urine arsenic is adjusted by the creatinine) to assess arsenic retention because it is better than using urine arsenic alone [18], and is positively correlated with plasma arsenic levels as reported in our previous investigation [13]. The present study showed that at the end of maintenance therapy, the median arsenic excretion rate returned to base level in both RIF and ATO groups. Thus, it is not likely to result in long-term arsenic retention regardless of treatment with ATO or RIF in children.
Relapse is uncommon in APL following contemporary treatment. This study proved that FLT3-ITD mutations are not a risk factor for relapse of pediatric APL, which is in line with the results of recent studies observed in adult patients [19]. Our previous studies showed that ATO/ATRA combination can work synergistically to promote ubiquitination-mediated and autophagic degradation of FLT3-ITD protein, selectively kill FLT3-ITD leukemia cells, and reduce the leukemic burden in mice with FLT3-ITD leukemia [20,21,22]. These experimental studies may explain, at least in part, how ATO and ATRA-based therapy can abrogate the negative impact of FLT3-ITD mutations. Some studies mainly on adult patients suggested that CD56+, CD34+, or CD2+CD34+APL subgroup had a higher rate of relapse [23,24,25], however, this was not proved in our pediatric patients treated on SCCLG-APL protocol. We also observed that urine arsenic excretion rate tended to be lower in relapsed than in non-relapsed patients (p = 0.090) (Suppl. Tables S5), indicating plasma arsenic level was correspondingly lower in the former [13]. As there were only 4 relapses in our cohort, the sample was too small to draw a conclusion that the relapse of the disease is related to insufficient plasma concentration of arsenic. Nevertheless, it is necessary to investigate the relationship between the relapse and plasma arsenic levels in the future. Lastly, there has been no clear guideline till now for how long should MRD be monitored in APL. This long-term study indicated that it is not necessary for MRD monitoring for more than 1.5 years after completion of maintenance therapy if MCR is achieved at the end of consolidation. Given the very low relapse rate of APL with contemporary treatment, MRD monitoring after MCR is only recommended for HR patients [19]. For NHR patients, using a peripheral blood sample instead of bone marrow for MRD monitoring may be considered if needed.
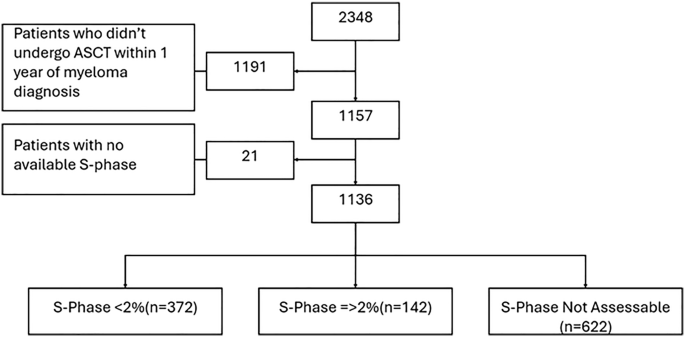
Although we obtained an excellent long-term survival rate in our cohort, there were 10 of 195 (5.1%) patients died before randomization. Among them, 8 died of intracranial hemorrhage, 1 intracranial hemorrhage and pulmonary hemorrhage, and 1 alimentary tract hemorrhage (Suppl. Table S2). The risk of hemorrhagic death during the induction period remains at about 5% in the clinical trial setting even nowadays [26, 27], and the mortality rate before diagnosis is unknown. Therefore, the survival rate of APL patients is lower in the real world. Although not all patients have completed the 5 years of follow-up from enrollment in this report (Fig. 1), the non-inferiority of RIF in efficacy compared with ATO was demonstrated, and both groups had 5-year EFS of 97.6%, after a median follow-up of 6 years. Another important observation was that oral RIF treatment can significantly reduce hospital days and incidences of adverse events.
In conclusion, the final results of the multicenter randomized trial SCCLG-APL confirmed that oral RIF is as effective as intravenous ATO for the treatment of pediatric APL. The substitution of RIF for ATO has the additional advantages of shortened hospital days, less infection risk, and cardiac toxicity in pediatric patients. Given its advantage over ATO in treating APL patients across all age groups, promoting the wider use of oral RIF outside of China is worthwhile.

Comments (0)