
Remember me
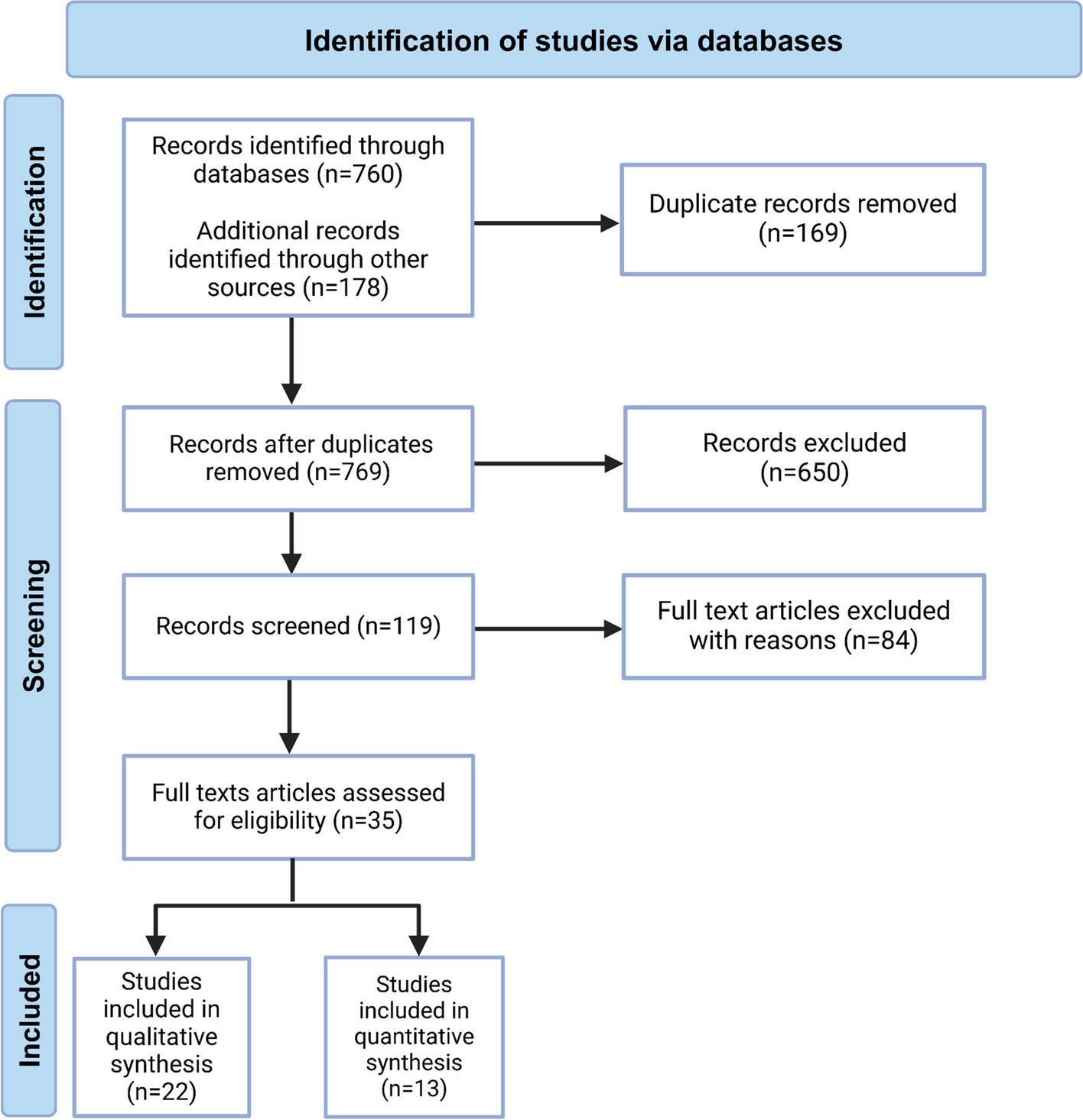

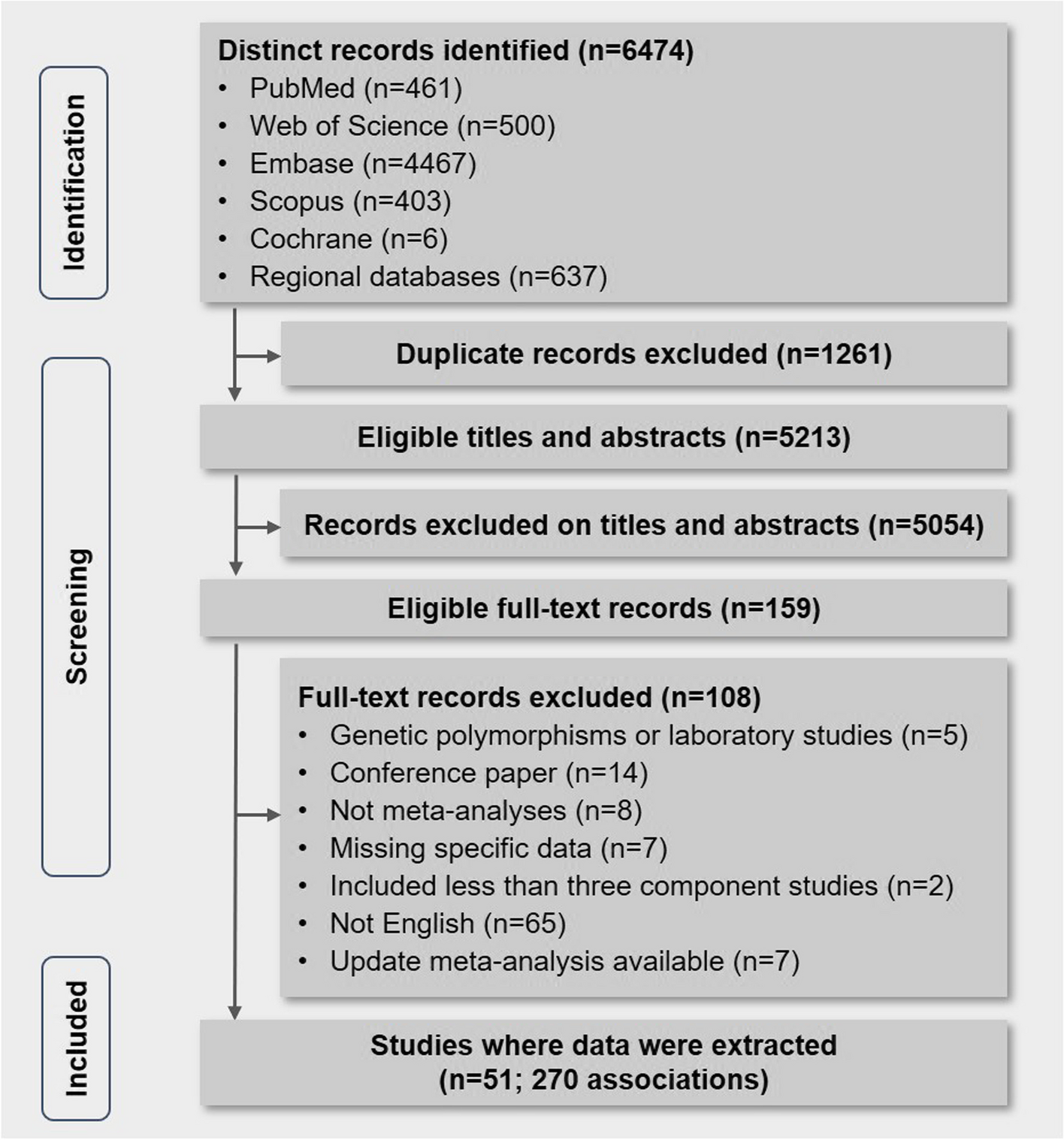
The detailed formation of the study cohort is shown in Additional file 3: Fig. S1. A total of 12,100 HCWs were included in this primary analysis.
Description of the analysed study sampleTable 1 shows the demographic and occupational characteristics of the analysed sample. The median age was 45 years (IQR: 34–54); most respondents were female (76%). 29.8% of respondents were overseas-born, and 30% were from non-White ethnic groups (19.2% Asian, 4.3% Black, 4.2% Mixed, 2.1% Other). The socioeconomic status of the study sample was higher than the UK population average, with almost half the sample (46.7%) residing in the least deprived areas (IMD quintiles 4 and 5) and only 8.8% in the most deprived quintile. Allied Health Professionals (AHPs, including healthcare scientists, ambulance workers, pharmacy staff and those in optical roles) were the largest group of participating HCWs by occupation (42%), followed by those in medical (23%) or nursing (21%) roles.
Table 1 Description of the UK-REACH cohort — results from the baseline questionnairePrevalence of long-term conditions (LTCs)The prevalence of each long-term condition is listed in Table 2. Anxiety (n=1804, 14.9%, 95%CI 14.3–15.6%), asthma (n=1471, 12.2%, 95%CI 11.6–12.8%), depression (n=1296, 10.7%, 95%CI 10.2–11.3%), hypertension (n = 1056, 8.7%, 95%CI 8.2–9.2%) and diabetes (n=486, 4.0%, 95%CI 3.7–4.4%) were the most prevalent conditions.
Table 2 Prevalence of long-term conditions (LTCs) reported by UK healthcare workers in the baseline questionnaire of the UK-REACH cohort studyAssociation of prevalent long-term conditions (LTCs) with ethnicity and migration statusAdditional file 4: Table S2, shows the frequency (%) of participants reporting the five most common conditions, stratified by ethnic/migrant group. Figure 1 shows odds ratios for the association of ethnicity and migration status with these conditions after adjustment for sociodemographic/occupational factors (Fig. S 2 shows the same figure, including the aOR and 95%CI values as text).
Fig. 1
The association of ethnicity and migration status with the five most prevalent long-term health conditions reported by healthcare workers in the UK-REACH study. Associations are derived from logistic regression models presented as odds ratios (circles) and 95% confidence intervals (spiked bars). White UK-born is the reference group. Odds ratios are adjusted for age, sex, index of multiple deprivation quintile and occupation. N=12,100 for all models. Panel D: results for the association between the “Other UK-born” group and diabetes are omitted due to low numbers (<5) in this group producing a very wide 95% confidence interval range (0.07–4.13)
The pattern of association between ethnicity and migrant status with reporting a mental health condition was similar for anxiety and depression (Fig. 1A and B, Additional file 5: Fig. S2A and S2B). Compared to White UK-born HCWs, the odds of reporting either mental health condition were lower in most other studied ethnic/migrant groups. Within ethnic groups, the odds ratios for mental health conditions for overseas-born HCWs tended to be lower than their UK-born counterparts when compared to the White UK-born group (e.g. for anxiety: Asian UK-born aOR 0.67, 95%CI 0.53–0.84; Asian overseas-born aOR 0.48, 95%CI 0.38–0.59).
The relationship between ethnicity and migrant status with reported diabetes and hypertension displayed a different pattern, with Asian and Black HCWs having higher odds of these conditions than White HCWs (Fig. 1C and D, Additional file 5: Fig. S2C and S2D). Within each ethnic group, odds ratios of developing diabetes and hypertension for overseas-born HCWs tended to be higher than their UK-born counterparts when compared to the White UK-born group with the exception of Black ethnic groups and diabetes (e.g. for hypertension Black UK-born aOR 1.77, 95%CI 1.05–2.99; Black overseas-born aOR 2.99, 95%CI 2.18–4.10; for diabetes: Asian UK-born aOR 1.70, 95%CI 1.11–2.63; Asian overseas-born aOR 2.97, 95%CI 2.30–3.83).
Figure 1E and Additional file 5: Fig. S2E show the differences between ethnic and migrant groups for odds of reporting asthma. Adjusted odds ratios were greater than 1 for all UK-born ethnic minority groups in comparison to the White UK group but reached statistical significance only in the Mixed and Other ethnic groups. In contrast, adjusted odds ratios for all overseas groups were less than one, and this was statistically significant for the White, Asian and Black groups.
Co-occurrence of long-term conditions (LTCs)Heatmaps illustrating the pattern of prevalence of two LTCs according to migration status (UK-born, overseas-born) are shown in Additional file 6: Fig. S3. For UK-born respondents, anxiety and depression had higher co-occurrence (48.3%) than in overseas-born respondents (37.5%). There was a high co-occurrence of hypertension with other LTCs in both UK-born and overseas-born, including organ transplant, diabetes, heart disease, stroke, kidney disease, liver disease and lung diseases other than asthma (20.2–47.1% for UK-born respondents, 10.0–50.0% for overseas-born respondents). The co-occurrence of diabetes with liver disease (17.8% for UK-born, 66.7% for overseas-born) and hypertension with kidney disease (34.4% for UK-born, 50.0% for overseas-born) was more marked for overseas-born HCWs than for UK-born HCWs, but care must be taken not to overinterpret the observed patterns of co-occurring LTCs due to small numbers reporting certain conditions (e.g. organ transplant n=15, stroke n=44).
Association of multiple long-term conditions (MLTCs) with ethnicity and migration statusTable 3 shows results from two logistic regression analyses to explore factors associated with reporting two or more LTCs listed in Table 1. The first regression (A) includes demographic and occupational covariates only, while the second (B) additionally includes health and lifestyle covariates. Overall, the prevalence of reported MLTCs was 15.0%. Raw prevalence was lower in all ethnic/migrant groups compared to the White UK-born reference group. When adjusting for sociodemographic covariates only (regression A), significantly reduced odds of MLTCs were noted in the White, Asian, Black and Other overseas-born groups compared to the White UK-born group (White overseas-born aOR 0.68, 95%CI 0.55–0.83; Asian overseas-born aOR 0.75, 95%CI 0.62–0.90; Black overseas-born aOR 0.52, 95%CI 0.36–0.74). This effect was more pronounced (in all groups apart from White overseas-born) after adjustment for health and lifestyle covariates (regression B), where significant differences were also found for Asian UK-born and Black UK-born groups (White overseas-born aOR 0.69, 95%CI 0.56–0.85; Asian overseas-born aOR 0.63, 95%CI 0.52–0.77; Black overseas-born aOR 0.39, 95%CI 0.27–0.56; Asian UK-born aOR 0.69, 95%CI 0.54–0.87; Black UK-born aOR 0.47, 95%CI 0.28–0.79).
Table 3 The association of ethnicity, migration status, sociodemographic and health and lifestyle factors with MLTCs (≥2 long-term conditions): (A) adjusted for ethnicity, migration status and sociodemographic covariates only, and (B) additionally adjusted for health and lifestyle covariates (n=12,100)Additional file 7: Table S3, shows the results of a negative binomial regression to explore the association of ethnicity, migration status, sociodemographic and health factors with long-term condition count. Results suggested the same associations as found in the logistic regressions (Table 3), albeit with a stronger relationship suggested for the effect of sex, with women reporting MLTCs at a lower rate than men.
Multiple long-term conditions (MLTCs) and duration of UK settlementFigure 2 shows how reporting of MLTCs changes for migrants by the duration of settlement in the UK. Odds ratios are adjusted for demographic factors and occupation. Migrants had significantly lower odds of reporting MLTCs upon arrival in the UK up to ≥20 years of residence, after which odds of MLTCs do not significantly differ from the UK-born respondents.
Fig. 2
Relationship between time since migration to the UK and risk of multiple long-term conditions (≥2 long-term conditions) expressed as odds ratios stratified by duration resident in the UK, compared to UK-born study participants (n=12,100). Odds ratios are adjusted for ethnicity, sociodemographic, health and lifestyle covariates. ref, reference group. Eighty-five missing values for years in the UK were imputed
Comments (0)